CEREBROVASCULAR ACCIDENT CVA PREPARED BY Dr Altayeb Abdulazeem

CEREBROVASCULAR ACCIDENT CVA PREPARED BY: Dr. Altayeb Abdulazeem Idress Ph. D , RN , CNS altayebabdo 9@gmail. com

Cerebral arteries

Cerebrovascular Accident CVA • Cerebrovascular disorders are disorders of the vascular system in the brain. • When the vessels are unable to supply blood and oxygen to brain cells, brain tissue dies, causing a cerebrovascular accident (stroke). • The most common cerebrovascular disorders include transient ischemic attack (TIA), stroke, and subarachnoid hemorrhage (SAH).
 • is a temporary impairment of the cerebral circulation causing")
TRANSIENT ISCHEMIC ATTACK (TIA) • is a temporary impairment of the cerebral circulation causing neurological impairment that lasts less than 24 hours. • It is characterized by a sudden, focal (specific area) neurological deficit caused by a brief period of inadequate perfusion of a portion of the brain.

• A TIA typically lasts minutes to hours, and the patient will have complete recovery. • Symptoms that last longer than 24 hours but do not cause permanent neurological changes are called reversible ischemic neurological deficits (RINDs). • If the symptoms do not reverse because an area of the brain is permanently damaged, then the event is considered to be a cerebral vascular accident (CVA), or stroke.

• Patients who have had a TIA have an increased risk of having a stroke; about 24% to 29% of patients who experience a TIA will have a stroke within 5 years. • TIA should be evaluated urgently to start appropriate therapy as soon as possible in order to decrease the risk of stroke
 of brain tissue caused by")
CEREBROVASCULAR ACCIDENT • Cerebrovascular accident is the infarction (death) of brain tissue caused by the disruption of blood flow to the brain. • It is characterized by focal neurological deficits specific to the area of the brain involved that do not fully resolve. • The patient does not return to baseline functional level. • In order to impress upon practitioners and the community the urgency of treating a stroke quickly, strokes are now being called brain attacks in the public setting.

• This reminds us that, like a heart attack, stroke is an urgent condition that can be treated if medical care is sought immediately. • If patients receive treatment within 3 hours of symptom onset, they may be able to receive medication that has the potential to fully resolve their deficits.

Pathophysiology • Cerebral function is dependent on oxygen and glucose delivery to neurons of the brain. • When blood flow is severely compromised or absent, the oxygen and glucose needed to meet the brain’s metabolic needs are not available. • The brain has no capability to store oxygen or glucose, so it relies on a constant supply of these nutrients. • If the supply of oxygen and glucose is stopped, the brain tissue dies.

• In contrast to TIA, a brain attack can cause permanent damage if it is not reversed with timely treatment. • The particular vessel or vessels involved determine the area of the brain affected and therefore the symptoms that result. • The duration of ischemia determines whether the symptoms are transient or permanent. • A transient ischemic attack may be a warning of an impending stroke.

Etiology • A stroke can be caused by ischemia or hemorrhage. • Most strokes present with sudden or rapidly evolving onset of symptoms. • It is difficult to make a diagnosis of stroke using clinical examination and history alone. • A CT scan or MRI is necessary to make a diagnosis of stroke, and to determine whether the stroke is due to ischemia or hemorrhage. • Etiology must be determined before treatment can be initiated.

Warning Signs • Sudden numbness or weakness of face, arm, or leg, especially on one side of the body • Sudden confusion, trouble speaking, or understanding • Sudden trouble seeing in one or both eyes • Sudden trouble walking, dizziness, loss of balance, or coordination • Sudden severe headache with no known cause 3

Ischemic Stroke • An ischemic stroke can be caused by embolism or thrombosis, with resulting decreased perfusion • When arteries are narrowed due to atherosclerotic plaque, they can become occluded (thrombotic stroke). • If emboli break away from plaque, they can travel and lodge in narrowed cerebral vessels (embolic stroke). • Emboli in the brain may be arterial or cardiac in origin.

the bifurcation of the common carotid artery into the internal and external branches is the most common location for cerebral atherosclerosis and subsequent occlusion from an embolism or thrombosis.

• Patients in atrial fibrillation can have small clots develop in the atria because the blood is not ejected normally, and as a result pools. These clots can be ejected into the circulation and become emboli.

• Stroke due to decreased perfusion occurs with severe stenosis of the carotid or basilar arteries, or with stenosis of the small deep arteries of the brain. • Decreased perfusion may also occur from vasculitis, an inflammatory condition involving the cerebral blood vessels. • Common causes of vasculitis are systemic lupus erythematosus, bacterial or tuberculous meningitis, fungal infection, and herpes zoster arteritis (arterial inflammation).

Hemorrhagic Stroke • Hemorrhagic stroke is caused by the rupture of a cerebral blood vessel. • When a cerebral blood vessel ruptures, the brain tissue beyond the vessel does not receive oxygen and nutrients and can die. • Additional damage can occur to the brain tissue surrounding the rupture from blood being released in the brain outside of the vascular system.
 is poorly controlled")
• The most common cause of an intracerebral hemorrhage (ICH) is poorly controlled hypertension. • Another cause is a ruptured aneurysm. • Hemorrhages tend to occur deep within the brain tissue. • Subarachnoid hemorrhage (SAH) is caused by rupture of blood vessels on the surface of the brain. • This type of infarct has the slowest rate of recovery and the highest probability of leaving the patient with extensive neurological deficits.

• The most common etiology of brain attack in younger patients is illicit drug usage. PCP (phencyclidine), crack, cocaine, amphetamines, and heroin have all been associated • with cerebrovascular accident from subarachnoid or intracerebral hemorrhage because these drugs raise the blood pressure and increase pressure within the cerebral vessels.

Acute Signs and Symptoms of CVA • Symptoms are varied and depend on the area of the brain affected. • Common symptoms include visual disturbances, language disturbances, weakness or paralysis on one side of he body, and difficulty swallowing (dysphagia). • These signs and symptoms are the same for both ischemic and hemorrhagic stroke.

• In addition, the patient with a hemorrhagic stroke may experience rapid deterioration, drowsiness, and a severe headache, often described as “the worst headache of my life. ” • Symptoms can last a few minutes to a few hours or may persist for an indefinite period of time

• Language Disturbances • Aphasia refers to the absence of language • Dysphasia refers to difficulty with speech and is not as severe as aphasia. • The patient may experience trouble selecting correct words, use incomprehensible or nonsense speech, have trouble understanding others’ speech, and have trouble writing or reading. • Aphasia may be expressive, in which the patient knows what he wants to say but cannot speak or make sense or receptive, with an inability to understand spoken and/or written words. • Global aphasia occurs when both expressive and receptive aphasia are present.

• dysarthria. • Slurred or indistinct speech and abnormal pronunciation of words and articulation because of a motor problem

• Motor Disturbances • Paralysis, weakness, or numbness can present as clumsiness, heaviness, and facial droop. • The onset will be sudden and generally involves one side of the body, the side of the body opposite to the damaged area. • The deficits may present on both sides of the body if the patient has experienced a brainstem stroke or a vertebrobasilar stroke. • Another clinical finding that affects mobility is ataxia.

• Ataxia may present as poor balance, a stumbling gait, or staggering. • This can be related to damage to the cerebellum, or to poor coordination due to weakness or paralysis on one side of the body. • If the muscles of swallowing are affected, dysphagia results.

• Visual Disturbances • visual loss is painless and may involve loss of all or part of the vision in one eye The involved eye is on the same side as the diseased artery.

Manifestations of right-brain and left-brain stroke.

Diagnostic Tests • A new assessment tool is now available to assist community members and emergency medical technicians in identifying stroke symptoms quickly. • The Cincinnati Prehospital Stroke Scale (CPSS) was created to facilitate transporting stroke victims to the hospital as soon as possible. • a patient who has one of three positive findings when the CPSS is used has a 72% probability of having an ischemic stroke. • If all three findings are positive, the probability increases to 85%.

• The CPSS has three components to review: • Have the patient smile. Look for subtle signs of facial droop or uneven symmetry of the face. • Ask the patient to hold the arms out straight in front while closing the eyes. Observe the patient’s arms closely for any signs of drifting downward. This can be performed with the patient standing or sitting down. • Ask the patient to repeat a phrase, such as “It is a bright and sunny day in Michigan. ” Did the patient understand? Did he repeat the phrase exactly? Did he exhibit any slurred speech or difficulty saying words?
 scan will be performed immediately. If the cause of symptoms is")
• (CT) scan will be performed immediately. If the cause of symptoms is a TIA, the CT scan will be negative for stroke since there has been no permanent damage to the brain. • (ECG) to determine if atrial fibrillation is present. • (CBC) • (PT) • (INR) • Carotid Doppler testing can determine if stenosis of the carotid arteries exists. The amount of restricted flow determines if the patient would benefit from a carotid endarterectomy to remove the occlusion from the • artery

• If the patient has arrived at the ED within 3 hours of the onset of symptoms, the patient will be evaluated for appropriateness for receiving t-PA (tissue plasminogen activator), a thrombolytic agent recently approved for use in strokes.

Therapeutic Interventions • Initial emergency care is supportive while test results are pending. • ABCs (airway, breathing, and circulation) are monitored. • Oxygen is administered to maintain oxygen saturation greater than 90%. • Vital signs and heart rhythm are monitored. • Diagnostic tests are done without delay. • When test results verify whether the stroke is hemorrhagic or ischemic, therapeutic interventions are initiated.
 is a recent development in the")
Thrombolytic Therapy • Thrombolytic therapy (alteplase or t-PA) is a recent development in the treatment of ischemic brain attack. • Intracerebral hemorrhage must be ruled out before t-PA therapy is instituted because of the risk of worsening a bleeding vessel. • The goal of thrombolytic agents is to actually break down the thrombus causing the occlusion, which can potentially prevent or completely reverse the symptoms of stroke.

• Cerebral hemorrhage is a major complication of thrombolytic therapy; therefore, it is only used if the patient meets strict criteria.

Contraindications of t-PA • Patients who have a history of intracerebral hemorrhage, recent stroke or serious head trauma, surgery within the past 3 weeks, recent lumbar puncture, GI or urinary bleeding, uncontrolled high blood pressure, or any other risk factors for bleeding cannot have t-PA because of the risk of bleeding. • To be effective, t-PA must be administered within 3 hours of the onset of symptoms. This time frame has clear implications for nurses.

Pharmacological Management • Blood pressure control is vital for the patient. • Care is taken not to lower the blood pressure too quickly or too far. • If the patient has long-standing hypertension, lowering the blood pressure to a “normal” level may actually cause further ischemia. • antiseizure medication as a prophylactic measure.

• Sometimes after a hemorrhagic stroke, the patient can experience vasospasm If this occurs, the patient may be treated with a calcium channel blocker like nimodipine, which relaxes smooth muscles of the vessel wall and reduces the vasospasm.

MEDICATIONS USED IN CVA

Post emergent Care • After emergent treatment, medical management focuses on controlling the cause of the transient ischemic attack or stroke. • Surgical Management of Carotid Stenosis

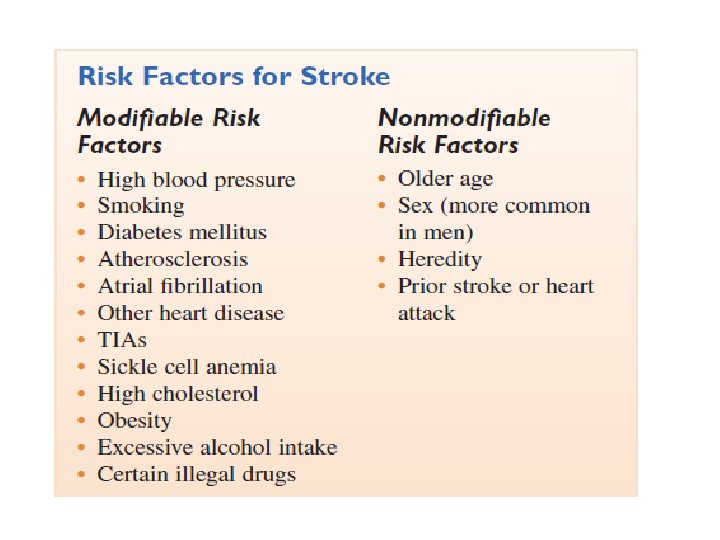
Prevention of Stroke • Incidence of stroke can be lessened by reduction of risk factors

Long-Term Effects of Stroke • • • impaired motor function and sensation aphasia emotional lability or instability impaired judgment unilateral neglect

Nursing Process for the Patient with a Cerebrovascular Disorder • Assessment/Data Collection • Assess the patient for signs and symptoms of decreased cerebral tissue perfusion: decreased level of consciousness, irritability or restlessness, dizziness, syncope, blurred or dimmed vision, diplopia, change in visual fields, unequal • pupils or a sluggish or absent pupillary reaction to light, paresthesias, motor weakness, paralysis, or seizures.

Nursing diagnoses • Impaired physical mobility related to decreased motor Function • Imbalanced nutrition, less than requirements related to impaired swallowing and motor deficits • Disturbed sensory perception related to CNS damage • Risk for impaired skin integrity: irritation or breakdown related to immobility and incontinence • Incontinence related to loss of voluntary control of elimination Self-care deficit related to decreased motor function, spatial-perceptual alterations, and fear of injury

• Impaired verbal communication: dysarthria related to loss of motor function of the muscles of speech articulation, or aphasia or dysphasia related to ischemia of the dominant hemisphere • Disturbed thought processes related to cerebral Ischemia • Deficient knowledge related to diagnosis and treatment

• Impaired physical mobility related to decreased motor Function • EXPECTED OUTCOMES: Patient will maintain physical mobility as evidenced by maximum physical mobility within limitations of deficits. Patient will not experience complications related to immobility.

• Implementation • Consult physical and occupational therapists to assess the patient’s abilities and make specific recommendations related to mobility. • Maintain the patient in good body alignment to prevent contractures and promote comfort. • Support affected extremities with pillows to prevent dislocation injuries and promote comfort. • Perform range of motion exercises as prescribed by physical therapist to prevent contractures and atrophy.

• Follow physical/occupational therapy recommendations for being up in chair or ambulation. • Prolonged bed rest is associated with complications and poor outcomes. • If patient is unable to get out of bed, turn and reposition at least every 2 hours to prevent complications to prevent skin, respiratory, and musculoskeletal complications.

• Imbalanced nutrition, less than requirements related to impaired swallowing and motor deficits • EXPECTED OUTCOME: Patient will maintain adequate nutrition without aspiration as evidenced by stable weight at appropriate level for height.

• Implementation • Keep patient NPO until swallowing can be evaluated to prevent aspiration. • Perform dysphagia screening. This quick assessment can identify problems before a complete evaluation can be done. • Observe for facial weakness or inability to completely close mouth. • Ask patient to stick out tongue and move it side to side.

• If swallowing appears to be intact, have patient swallow a sip of water from a cup before offering other foods or fluids. Observe for coughing, choking, or noisy lung sounds. These are signs of difficulty swallowing. Implement measures to prevent aspiration. • Aspiration can lead to pneumonia, which will greatly complicate the patient’s recovery. • Stay with patient during meals. • Ensure that patient is fully alert before feeding. • Have the patient in high-Fowler’s position or chair for meals.

• Incontinence related to loss of voluntary control of elimination • EXPECTED OUTCOME: Episodes o incontinence are avoided, or if unavoidable, they will be cleaned up quickly and skin complications avoided.

• Implementation • Monitor for incontinence of bowel or bladder so patient can be cleaned promptly and skin protected. • Assess for usual pattern of urinary and bowel elimination. Keeping the patient on his or her regular prehospitalization pattern may help prevent incontinence. • Provide assistance with toileting according to the patient’s usual schedule. The patient who is unable to get up unaided may wait too long for help or try to get up alone and be injured. • Respond quickly to requests for assistance with toileting to avoid accidental incontinence.

• Self-care deficit related to decreased motor function, spatial-perceptual alterations, and fear of injury • EXPECTED OUTCOME: Self-care is accomplished as evidenced by patient’s ADL needs being met, and patient becomes increasingly independent.

• Implementation • Place objects within reach and within visual field. • Place food/fluids within patient’s visual field. • Encourage use of assistive devices. • Assist patient with learning to use nondominant side of body. If dominant side is affected, the patient may have to use the nondominant side. • Provide positive feedback to help reduce discouragement with slow progress. • Provide education for family members and significant others regarding patient’s deficits and recovery

Thank you Altayebabdo@yahoo. com
- Slides: 56