Cerebrospinal Fluid Analysis BY BIJO AUGUSTINE Anatomy and

Cerebrospinal Fluid Analysis BY BIJO AUGUSTINE
 is present within the subarachnoid space surrounding the")
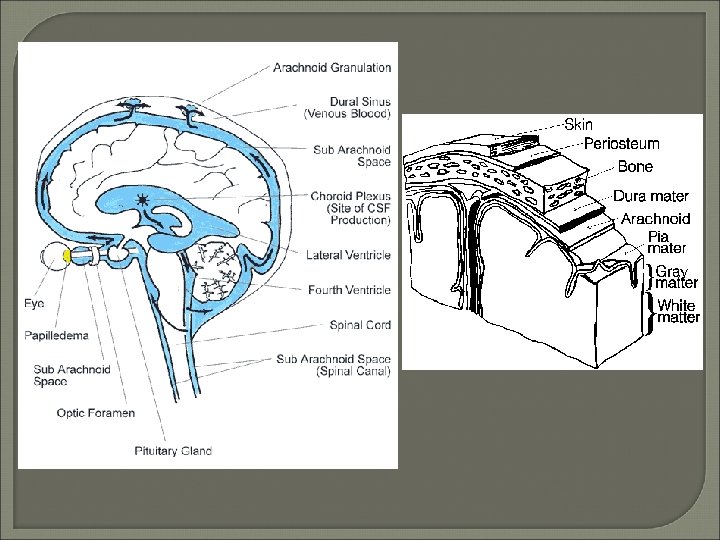
Anatomy and Physiology Cerebrospinal fluid (CSF) is present within the subarachnoid space surrounding the brain in the skull and the spinal cord in the spinal column. Total volumes: – Adults: 140 - 170 m. L – Children: 10 - 60 m. L

Functions of CSF It’s main function is to protect the brain and the spinal cord from injury by acting as a fluid cushion. It is the medium through which nutrients and the waste products are transported between brain/spinal cord and the blood.

Formation and composition of CSF is derived by ultra filtration of plasma and by secretion through the choroid plexus located in the ventricles of the brain. Reabsorbtion of CSF occurs at the arachnoid villi which projects in the venous sinuses in the duramater. CSF is produce at the rate of 500 m. L/day.

Formation and. Composition of CSF Blood brain barrier maintains the relative homeostasis of CNS environment by tightly regulating the concentration of substances by specific transport systems for H+, K+, Ca 2+, Mg 2+, HCO 3 -. Glucose, urea and creatinine diffuse freely between blood and the CSF.

Formation and Composition of CSF Proteins cross freely by passive diffusion along the concentration gradient and is also influenced by molecular weight.

Composition of Normal CSF Protein Glucose Urea Uric acid Creatinine Cholesterol Ammonia - 15 - 45 mg/d. L 50 - 80 mg/d. L 6. 0 - 16 mg/d. L 0. 5 - 3. 0 mg/d. L 0. 6 - 1. 2 mg/d. L 0. 2 - 0. 6 mg/d. L 10 – 35 μg/d. L

Composition of Normal CSF Sodium Potassium Chloride Magnesium Cells - 135 – 150 m. Eq/L 2. 6 – 3. 0 m. Eq/L 115 – 130 m. Eq/L 2. 4 – 3. 0 m. Eq/L 0 – 5 Lymph/μL

Clinical Application of CSF Examination In the diagnosis of a. Bacterial, viral or fungal meningitis. b. Encephalitis. c. Malignant infiltrates like in acute leukemia, lymphoma. d. Subarachnoid hemorrhage. e. Spinal canal blockage leading to elevated intracranial tension. f. Sub acute sclerosing pan encephalitis (SSPE)

Characteristics of normal CSF • • Color - Colorless PH - 7. 28 – 7. 32 Appearance - Clear Sp. Gravity - 1. 003 – 1. 004 No clot formation on standing Total solids - 0. 85 – 1. 70 g/d. L PO 2 - 40 – 44 mm. Hg

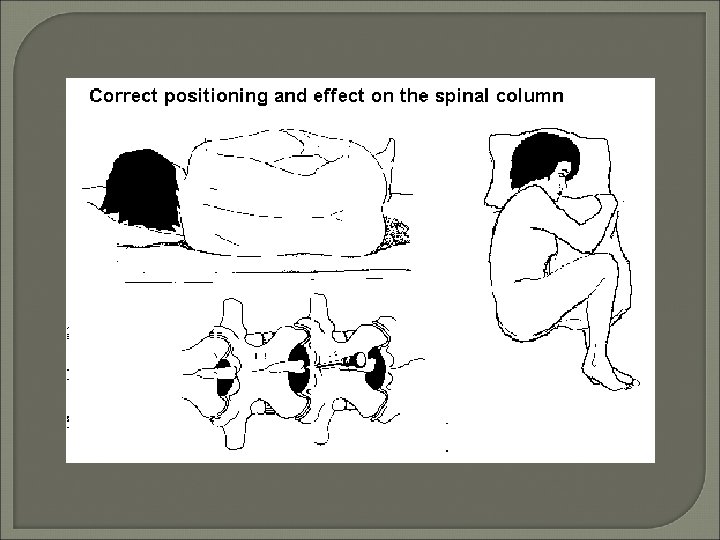
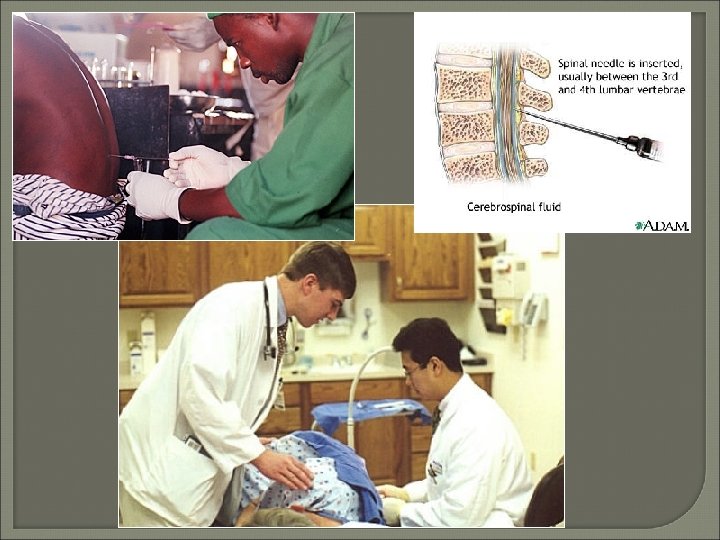
Collection and Processing • Lumbar puncture, cisternal puncture, lateral cervical puncture, shunts & cannulas • Opening pressure = 90 - 180 mm H 2 O (+/-) • Approximately 15 - 20 cc fluid collected • Process within 1 hour without refrigeration - STAT • Three tube set-up: – Tube 1: – Tube 2: – Tube 3: Chemistry and Immunology (Frozen) Microbiology (Room temperature) Cell count, differential, cytology (Refrigerated)

Diagnosis by CSF • High sensitivity, high specificity – Bacterial, TB, and fungal meningitis • High sensitivity, moderate specificity – Viral meningitis, SAH, CNS syphilis, abscess • Moderate sensitivity, high specificity – Meningeal malignancy • Moderate sensitivity, moderate specificity – Intracranial hemorrhage, viral encephalitis, subdural hematoma

Routine Lab Tests • • • Required Opening CSF pressure Macroscopic Examination Total cell count and differential (stained) Glucose (CSF/plasma ratio) Protein Optional Cultures, gram stain, antigens, cytology Protein electrophoresis, VDRL, D-dimers

Gross Examination • • • Normal CSF is clear, colorless Viscosity equal to water Clot seen in traumatic tap, not SAH Viscous CSF with increased protein exudate Turbidity: – WBC > 200 cells/ L – RBC > 400 cells/ L – Microorganisms, increased protein

Clot/Coagulation formation Allow the specimen of CSF to stand over night and examine the sample for fibrin clot, which is formed if the sample contains fibrinogen. Also note the nature of the clot. - Delicate clot, which resembles a cobweb, is characteristically seen in tubercular meningitis due to marked increased in CSF proteins. The clot may have entrapped tubercle bacilli, which could be demonstrated microscopically by staining for acid-fast bacilli.

Clot/Coagulation formation Corase clot is formed in pyogenic meningitis, traumatic tap and in case of complete spinal block. p. H Determination. p. H can be measured by using p. H paper or using p. H meter.

Xanthochromia • • Pink, orange, or yellow discoloration RBC lysis or hemoglobin breakdown May be seen within hours of LP Peak intensity at 24 - 36 hours RBC > 6000/μL (SAH, ICH, infarct, traumatic) Oxyhemoglobin, bilirubin, increased protein Carotinoids, melanin, rifampin therapy

Differential Dx of Bloody CSF • Traumatic tap - blood clears between tubes • Xanthochromia - pink tinge, RBCs • SAH - blood does not clear or clot

Microscopic Exam of CSF Total WBC Count Normal CSF contains 0 -8 lymph and no RBCs. Procedure Glass slides Counting chamber Cover slip of thickness with size of 22 ˟ 23 mm CSF diluting fluid – 1% Toludine blue or 1 % violet – stains the WBC without lysing the RBC, thus enabling to count both RBC and WBC in the

• Same chamber. The stain is mixed with the CSF in the ratio 1: 9 dil. • Dilute acetic acid – 0. 1 gm of crystal violet is added to 1 ml glacial acetic acid is made up to 50 ml by adding distilled water. Few drops of phenol is also added to this. As this fluid lyses the red cells it is useful in case of blood tinged CSF. In such case the RBC count estimated separately using undiluted CSF sample.

Procedure Dilution – if CSF is clear there is no need for dilution and both RBS and WBC can be counted simultaneously in the same chamber. If CSF is cloudy then make a dilution of 1: 10 or 1: 20. One can also pipette out 900μL of CSF diluting fluid in the tube and 100μL of CSF to it.

Counting of cells • Charge the counting chamber properly without any air bubbles. • Wait for 5 minutes before counting, to allow the cells in CSF to settle down. • Count the cells in all 9 squares by using low power objective. Calculation WBC in CSF/cumm(μL)=No. of cellˣdep. ˣdilu. Area counted

Important points • Cells in CSF should be counted immediately with out delay to prevent degeneration of cells which will give false low counts. • Bloody/ traumatic tap adds approximately 1 -2 WBC per 1000 RBCs. Hence in the estimation of total leucocytes count a deduction is made equivalent to 1 WBC for every 700 erythrocytes counted.

Differential leucocytes count • Chamber differential. • Differential cell count • Leishman’s stained smear or Gimsa’s Stained smear.

Reference Intervals for CSF
 Other infections Following")
Increased Neutrophils in CSF • • Meningitis (bacterial, early TB, fungal) Other infections Following seizures Following CNS hemorrhage Following CNS infarct Reaction to repeated LP Foreign materials Metastatic tumor
 • Parasitic infections •")
Increased Lymphocytes in CSF • Meningitis (aseptic, viral, L monocytogenes) • Parasitic infections • Degenerative disorders – Encephalopathy due to drugs, GBS • Other inflammatory conditions – Sarcoidosis, polyneuritis, periarteritis involving the CNS

Plasmacytosis in CSF • • • TB meningitis Syphilitic meningitis Parasitic infection Sarcoidosis Acute viral infections

Immature cells in CSF

Eosinophilic pleocytosis in CSF • • Commonly associated with Parasitic infections Fungal infections Reaction to foreign material Infrequently associated with Bacterial or tuberculous meningitis Viral, rickettsial infection, lymphoma, sarcoidosis

Chemical Analysis • Total protein non-specific marker of disease • Turbidimetric methods based on TCA or SSA & sodium sulfate for precipitation • Simple, rapid, no special instrumentation • 300 different proteins have been isolated from CSF using two-dimensional electrophoresis and silver staining

Conditions Associated with Increased CSF Total Protein • Increased blood-CSF permeability – Meningitis (bacterial, fungal, TB) – Hemorrhage (SAH, ICH) – Endocrine disorders – Mechanical obstruction (tumor, disc, abcess) – Neurosypilis, MS, CVD

Electrophoresis • Identification of oligoclonal bands • 2 or more discrete bands in the gamma region absent or of lesser intensity in concurrently run patient’s serum • Silver stain more sensitive than paragon violet • IFE better resolution and more specific • Sensitivity = 83 - 94%

Glucose estimation in CSF • CSF glucose is derived from blood glucose hence, ideally CSF glucose level should be compared with fasting plasma glucose level for adequate clinical interpretation. • Clinical Significance. • CSF glucose less than 40 mg/d. L or CSF/plasma glucose less than 0. 3 are considered abnormal (normal CSF/Plasma glucose ratio may very from 0. 3 – 0. 9)

• Increased CSF glucose is of no clinical significance. • Causes of decreased CSF glucose • Meningitis-Bacterial, fungal tubercular and syphilitic meningitis. • Tumors involving the meninges. • Subarachnoid hemorrhage. • Cerebral ameobiasis.

Bacterial Meningitis • • • 0 - 1 m: Group B strept & E. coli (GNR) 1 m - 5 y: H. influenzae 5 - 29 y: N. meningitidis >29 y: S. pneumoniae Listeria monocytogenes common in newborns, elderly, and other immunocompromised hosts

Bacterial Meningitis • • Gram’s stain sensitivity = 60 - 90% Depends on organism, experience, Culture sensitivity = 80 - 90% Latex agglutination becoming more widely used due to simplicity and accuracy

Test Appearance Pressure WBC/μL Normal CSF Clear 90 – 180 mm Acute bacterial meningitis Turbid Viral meningitis Clear Protein mg/d. L Glucose mg/d. L Chloride 0 -8 lymph. 15 -45 50 -80 115 -130 m. Eq/L Increased 10000 100 – 500 < 40 Decreased Normal to moderate increase 5 -300, rarely >1000 Normal to mild increased Normal Tubercular Slightly meningitis opaque cobweb formation Increased/ decreased, spinal block 100 -600 mixed or lymph. 50 -300 due Decreased to spinal block Decreased Fungal meningitis Clear Increased 40 -400 mixed 50 -300 Decreased Acute syphilitic Clear Increased About 500 lymph Increased but <100 Normal normal

Bacterial Meningitis

Neurosyphilis • • • Darkfield microscopy for spirochetes CSF FTA-ABS 100% sensitive Negative test rules out diagnosis VDRL nearly 100% specific Positive test rules in neurosyphilis RPR unsuitable for CSF (higher FP than VDRL)

Neurosyphilis
 account for 80% cases • Diagnosis")
Viral Meningitis • Enteroviruses (echoviruses, coxsachie, polio viruses) account for 80% cases • Diagnosis of exclusion, rarely use cultures • Viral inclusions for CMV, HSV • PCR for HSV available • Usually requires brain biopsy

HIV • Wide variety of abnormalities with or without neurological disease • Lymphocytic pleocytosis, elevated Ig. G, and oligoclonal bands • ID of opportunistic (fungal) infections main reason for examining CSF

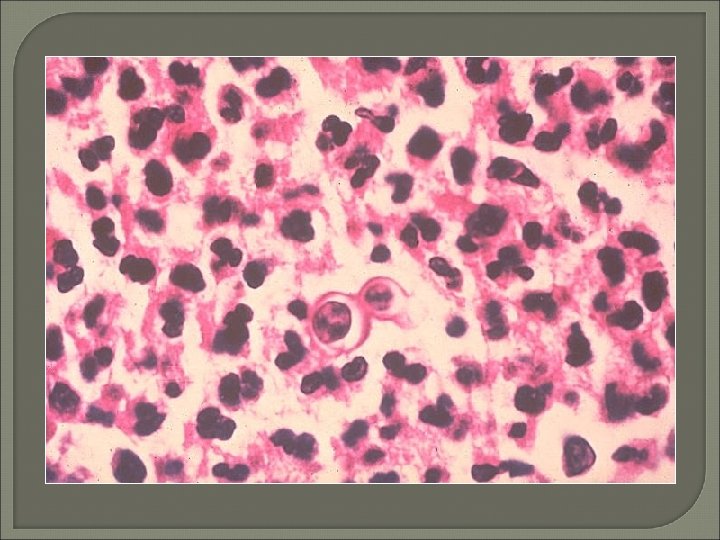
Fungal Meningitis • • India ink for cryptococcal capsular halos 50% sensitivity LA and CF antibodies now available Sensitivity as high as 96%


Tuberculous Meningitis • • Early diagnosis extremely difficult Sensitivity for acid-fast stains 10% Large volumes of CSF recommended Higher levels of adenosine deaminase ELISA and PCR now available Sensitivity = 50 - 82% Specificity = 90 - 100%
 • Rare disease caused by free-living amoeba Naegleria fowleri or")
Primary Amoebic Meningoencephalitis (PAM) • Rare disease caused by free-living amoeba Naegleria fowleri or Acanthamoeba species • Motile Naegleria trophozoites may be seen with light microscope • Acridine orange stain can differentiate amoeba (brick red) from leukocytes (bright green)

CSF Cytology • Cytological evaluation of CSF is an effective means for diagnosing many disorders involving the central nervous system. Preparatory methods for CSF examination are discussed and normal and reactive conditions involving lymphoma, leukemia, meningeal carcinomatosis and the subarachnoid spread of primary brain tumors are evaluated by primary cytological examination of CSF

Thank you
- Slides: 54