Cerebral Vascular Accident STROKE RISK FACTORS FOR STROKES

Cerebral Vascular Accident STROKE


RISK FACTORS FOR STROKES ► Nonmodifiable § Age- incidence ↑ with age until age 75. § Race- higher in African Americans § Gender- higher in men § Heredity- family history increases risk ► Potentially Modifiable § Lifestyle- excessive alcohol, cigarette smoking, obesity, high fat diet, drug abuse. § Pathologic conditionscardiac disease, DM, HTN, migraine headaches, hypercoagulability states.


ETIOLOGY AND PATHO ► Extra-cranial factors- related to the circulatory system. § Systemic blood pressure- <70 and >160 § cardiac output- when reduced by 30% cerebral blood flow is reduced. § Blood viscosity- anemia increases cerebral blood flow and polycythemia reduces it.

INTRACRANIAL FACTORS ► A. Metabolic factors § Increased CO 2 and low O 2 results in vasodilation to restore blood flow to normal. § CO 2 is the most potent regulator of cerebral blood flow. § Increased Hydrogen ion concentration increases cerebral blood flow.

Intracranial factors, cont’d ► B. Blood vessels § The condition of the blood vessels supplying the brain is important!!! ►Potential problems- congenital anomalies (tortuosity, coiling, kinking, and AV malformations). ►The malformations interfere with cerebral blood flow and contribute to atherosclerotic disease ►Collateral circulation develops ►Circle of Willis

Intracranial factors, cont’d ► C. Intracranial pressure § ICP increases with an assault to brain. § Causes of ICP: stroke, neoplasms, inflammation, trauma, and hydrocephalus. § ICP compresses the brain and reduces cerebral blood flow, which may lead to infarct. § Both extracranial and intracranial factors may lead to stroke

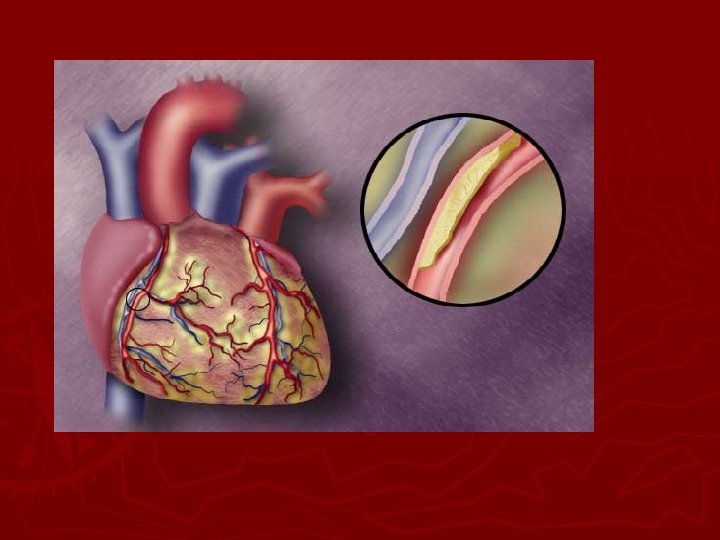
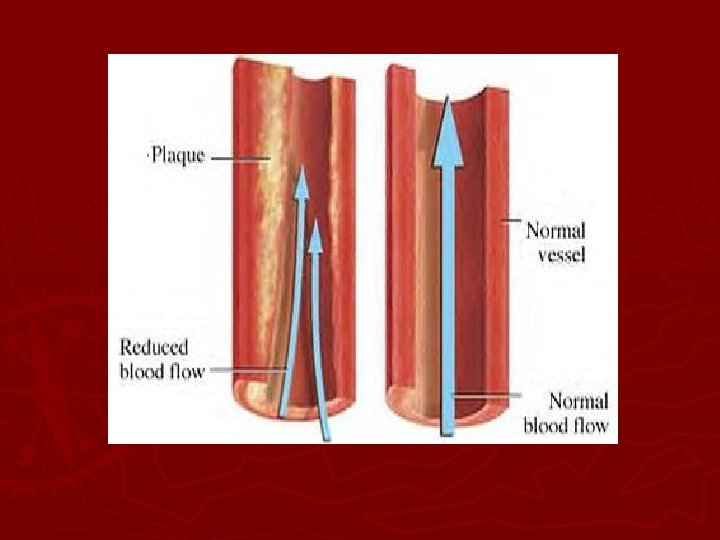
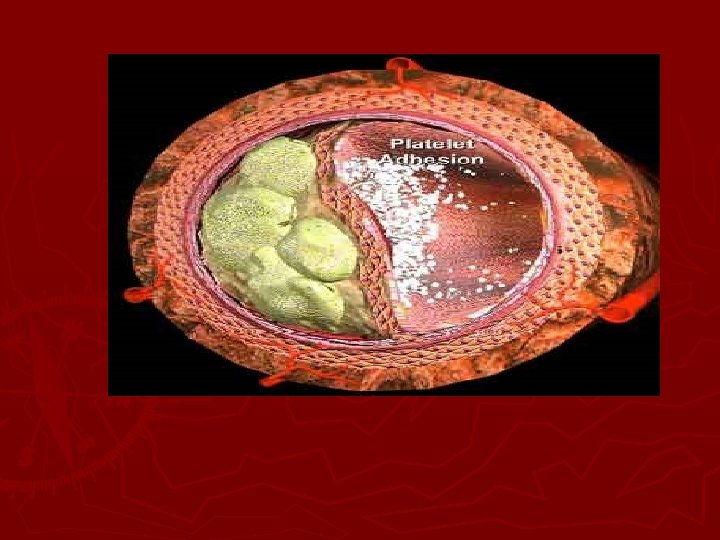
Atherosclerosis ► An abnormal accumulation and infiltration of in the intima of the arteries. ► Plaques develop in an area of high turbulence; which may later damage the plaque. ► Platelets and fibrin aggregate or collect on the surface of the plaque. ► Parts of the plaque breaks off and travel to a narrower distal artery ► Cerebral infarct occurs.

TYPES OF STROKE ► Ischemic: Most common type of stroke! § Occurs due to decreased blood flow to an area of the brain due to partial or complete occlusion of and artery due to thrombosis. § This lack of blood, oxygen and nutrients to an area of the brain causes necrosis of cerebral tissue. § Two types: thrombotic and embolic § See Lewis, page 1648; table 55 -1.

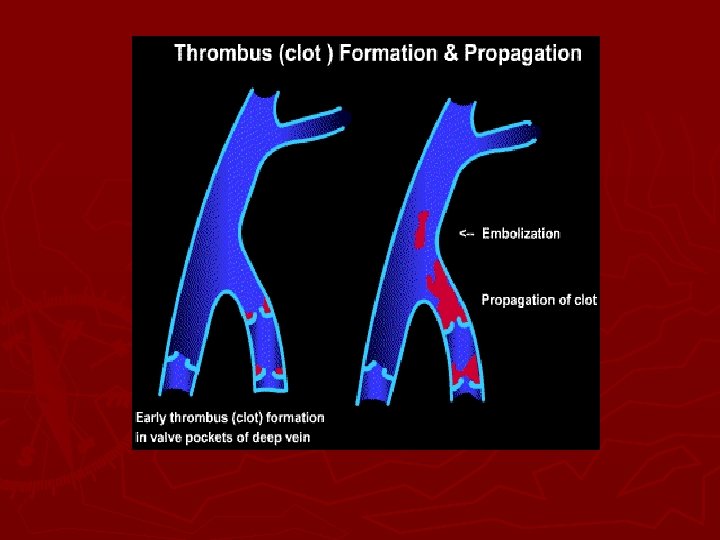
Thrombotic stroke ► Most common cause of cerebral infarct! ► Cause: Due to formation of a blood clot or coagulation of blood that results in narrowing of blood vessel or occlusion. ► 2/3 of strokes due to HTN or DM. (accelerate the atherosclerotic process) ► May also be due to oral contraceptives, coagulation disorders, polycythemia, arteritis, chronic hypoxia and dehydration.
 called TIA’s")
Thrombotic Stroke ► Thrombotic strokes are usually proceeded by prodromal episodes (warnings) called TIA’s (transient ischemic attacks). ► TIA’s last from 5 to 30 minutes. § Include- paresis or decreased strength and motion of an extremity. § Aphasia or disturbance of language function, § Paralysis, mental confusion, or visual disturbances.

Thrombotic stroke ► The extent of the stoke depends on rapidity of onset, size of lesion, and presence collateral circulation. ► There is a pattern to thrombotic stroke! § 1. single attack; symptoms occur over several hours § 2. intermittent progression toward a stroke over hours or days. § 3. partial stroke with permanent neuro deficits § 4. series of TIA’s followed by a stroke with permanent neuro deficits.

Thrombotic stroke ► Symptoms at 72 hours are usually due to resulting edema to tissues; symptoms improve after edema subsides (@ 2 weeks). ► This type of stroke occurs during or after stroke.

EMBOLIC STROKE ► Cerebral embolism results from occlusion of cerebral artery by an embolus. ► Necrosis and cerebral edema results. ► Embolus is the second most common cause of stroke. ► Most emboli originate in the endocardium with plaques or tissue breaking off and entering circulation.

Embolic Stroke ► Emboli are associated with heart conditions such as; § A fib § MI § Infective endocarditis § Rheumatic heart disease § Valvular prostheses § ASD

Embolic stroke ► Less common causes of emboli: § Air § Fat from long bone fracture § Amniotic fluid postpartum § tumors

Embolic stroke ► Prodromal warning less likely; single events ► sudden onset ► Most commonly related to head trauma ► High rate of re-occurrence if cause is not treated.

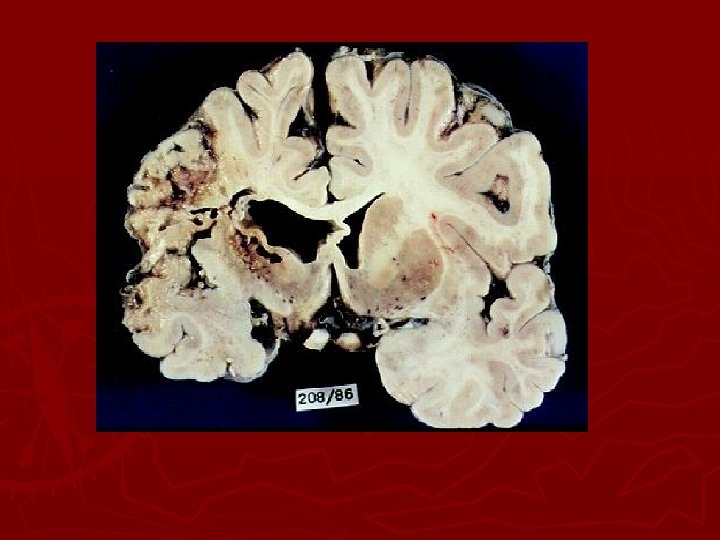
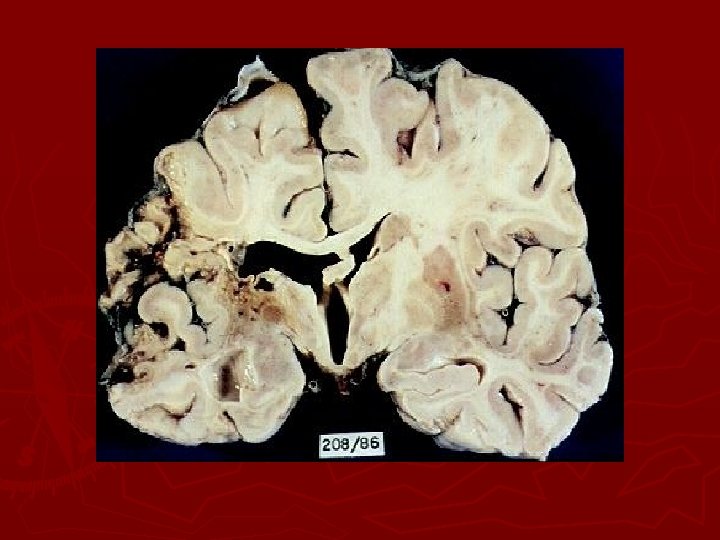
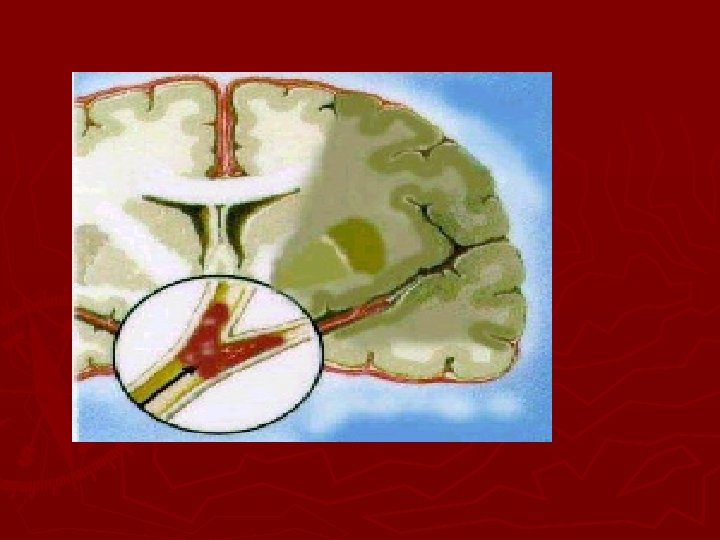
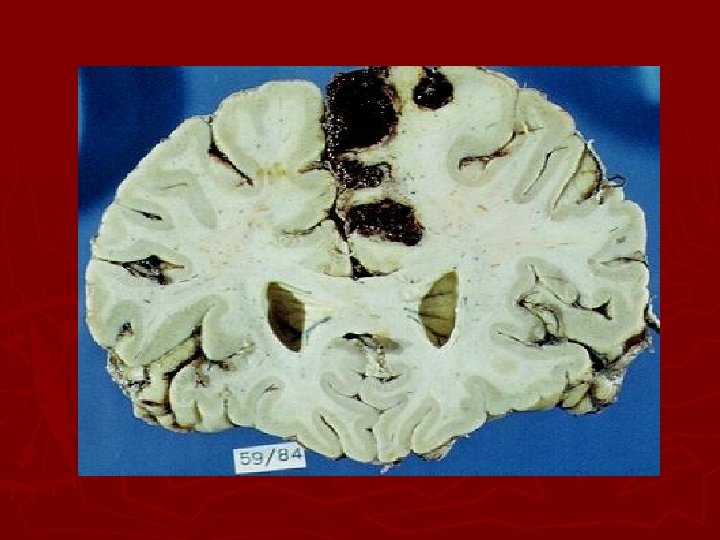
Hemorrhagic stroke ► Intracerebral hemorrhage is bleeding within the brain caused by rupture of a blood vessel that lasts from minutes to days. ► Most commonly caused by HTN ► May be caused by brain tumors, trauma, thrombolytic drugs, and ruptured aneurysms.

Hemorrhagic stroke ► Blood within the closed area of the brain imposes pressure on the brain tissue and displaces brain tissue and decreases blood flow to brain. ► Clinical manifestations depends on the site and amount of hemorrhage and resultant damage. ► Poor prognosis; 70% die

Subarachnoid stroke ► Caused by aneurysms, AV malformations, trauma, and HTN. ► May have prodromal symptoms if ballooning or dilation applies pressure to brain tissue. ► May suddenly rupture, causing neuro changes ► Majority of aneurysms are in the Circle of Willis

Subarachnoid hemorrhage, cont’d ► If aneurysm leaks, pt may have a headache! ► Rupture of aneurysm causes pressure in subarachnoid space due to bleeding. Clinical manifestations: § Headache, lethargy, confusion, nausea, vomiting, fever, neck pain, and backaches, paralysis, coma and death. Massive hemorrhage is defines as 30 to 50 ml of blood. Watch for re-bleeding when clot starts to dissolve. (usually within first 2 weeks post rupture). Reduce activity and prevent straining.
- § Brief episodes of neuro")
Temporal Development of CVA ► Transient Ischemic Attacks (TIA’s)- § Brief episodes of neuro manifestations (less than 24 hours). § Leaves no residual effects § Three categories: ► 1/3 never have another TIA ► 1/3 will have more than one TIA ► 1/3 will have a stroke WARNING SIGNS OF PROGRESSING CVA!

TIA’s ► s/s vary depending on the part of brain affected. ► Treatment: § Medications such as aspirin, Persantine (dipyridamole), Ticlid, and anticoagulant medication. § Long term therapy post TIA § Surgical treatment- carotid endartarectomy, extra-cranial- intracranial bypass (EC-IC bypass), and transiluminal angioplasty.

Reversible ischemic Neurologic Deficit ►A neuro deficit which remains 24 hours after onset; but leaves no residual signs or symptoms. ► Considered a completed stroke with minimal to no residual deficits ►

Stroke –In- Evolution ►A progressive stroke which develops over hours or days. ► Characteristic of an enlarging intra-arterial thrombus. ► A stepwise or intermittent progression of deterioration of neurological symptoms. ► Manifestations do not resolve and leave residual damage.

Completed Stroke ► Neuro defects unchanged over 2 to 3 days. ► Usually embolic in nature ► Also called “stable stroke”. ► Signals readiness for aggressive rehab therapy. (unless an aneurysm is involved).

Clinical Manifestations ► All deficits are directly related to area of brain that is involved. ► See Lewis, page 1650, Table 55 -2.

Neuromotor Function ► Destruction of motor neurons in the pyramidal pathway causes: § Mobility § Respiratory function § Swallowing and speech § Gag reflex § Self-care abilities
. ► Impairment of integration of")
Motor deficits ► Loss of skilled voluntary movement (akinesia). ► Impairment of integration of movements ► Alterations in muscle tones ► Alteration in reflexes ► Initial hypo-reflexia which progresses to hyper-reflexia for most patients.

Patterns of deficits ► Contralateral deficits § A lesion on one side of the brain affects the motor function on the other side of the brain. § The arms and legs on the affected side may be weak or paralyzed to different degrees depending the degree of cerebral circulation compromised. § See Lewis, Page 1651; Table 55 -5

► The affected shoulder tends to rotate internally; the hip rotates externally. ► The affected foot is plantar flexed and inverted. ► An initial period of flaccidity may lasts for several days to weeks. ► Spasticity of muscles follows the flaccid stage and is related to interruption of upper neuron influence.

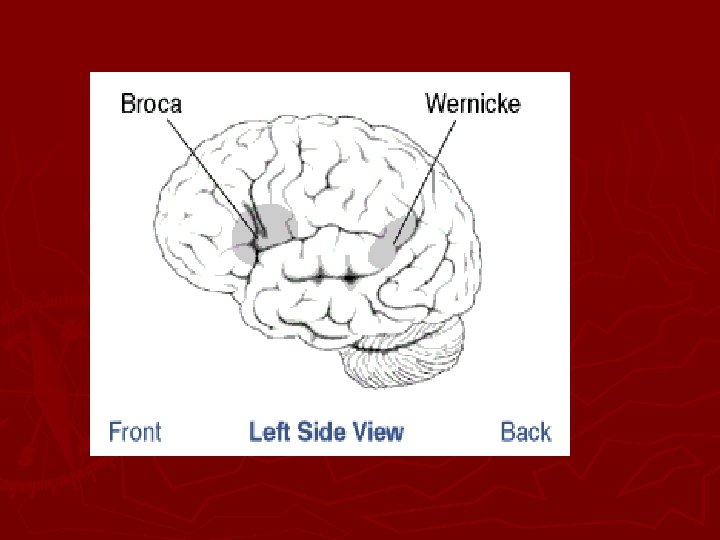
Communication ► Aphasia- total loss of comprehension and use of language due to damage to the dominant hemisphere (left hemisphere). ► Dysphasia-dysfunction related to comprehension or use of language due to partial disruption or loss. § Non-fluent (minimal speech activity with slow speech that requires obvious effort) § Fluent- (speech is present, but contains little meaningful communication).

Communication ► Conductive aphasia- mixture of both expressive and receptive aphasia ► Global aphasia- results from a massive lesion and there is virtual loss of all language ability.

Communication, cont’d ► Wernicke’s area damage § Receptive aphasia where neither the sound or speech or its meaning can be understood. § Impaired comprehension of both spoken and written language. Boca’s area damage Expressive aphasia (difficulty speaking and writing) Dysarthria- disturbance in muscular control of speech. (pronunciation, articulation, phonation) DOES NOT EFFECT COMPREHENSION OF LANGUAGE.

Affect ► May be unable to control emotions ► May be depressed RT body image and loss of function ► May be frustrated RT immobility and communication issues

Intellectual Function ► Memory and judgment may be impaired ► Left-sided stroke patients are more cautious in judgment and movement. ► Right-sided stroke patients more impulsive and move quicker.

Spatial-Perceptual Alterations ► Right sided stroke patient has more spatialperceptual orientation issues: § Erroneous perception of self and illness (may deny illness or body parts). § Erroneous perception of self in space (may ignore affected side; can’t judge distances) § Agnosia or inability to recognize an object by sight, touch or hearing. § Apraxia or the inability to carry out learned sequential movements on command.

Elimination ► Most occur initially and are transient. ► Frequent constipation DT immobility, weak abdominal muscles, dehydration, and diminished defecation reflexes. ► Urinary and bowel elimination may be DT functional inabilities to express needs and manage clothing.

Diagnostic Studies ► CT Scan- indicate size and location of lesion, differentiates between infarct and hemorrhage, effectiveness of treatment, and evaluate the course of healing. ► MRI- considered best method to differentiate between hemorrhage and infarct.

Diagnostics ► PET shows chemical activity and depicts extent if tissue damage. ► DSA- IV or arterial injection of contrast material to visualize blood vessels. ► TDA- transcranial doppler measures velocity of cerebral blood flow in the arteries, also detects micro-emboli. ► LP may be done to detect blood or WBC’s (not done if increased ICP is suspected)

Collaborative care ► PREVENTION § Healthy diet § Weight control § Regular exercise § No SMOKING § Limiting alcohol § Routine health assessment

DRUG THERAPY ► Prophylactic low dose aspirin, daily. ► Persantine 50 mg 3 X day decreases platelet aggregation which helps to decrease risk of thrombus and embolus formation. ► TICLID or PLAVIX- platelet aggregation inhibitors
- the atheromatous lesion is removed from the carotid")
Surgical Therapy ► Carotid endarterectomy (CEA)- the atheromatous lesion is removed from the carotid artery to improve blood flow § Decreases stroke and death in patient with TIA’s. § Done on patient with 70 -99% occlusion

Transluminal Angioplasty ► Insertion of balloon to open stenosed artery to permit blood flow. § Patient with symptomatic stenosis of vertebrobasilar or carotid arteries § Risk of dislodging emboli

EC-IC BYPASS ► Extracranial-intracranial bypass § Used when obstruction cannot be removed directly § A branch of extracranial artery is anastomosed to a branch of intracranial artery just beyond the area of obstruction. § Patients at high risk for stroke and require close -long term assessment and management.

ACUTE CARE ► Table 55 -5; Lewis page 1654. ► Initially § Ensure patent airway DT altered level of consciousness. ►Remove dentures Administer oxygen via nasal cannula or nonrebreather mask DT respiratory distress

Acute Care ► Establish IV access with normal saline to maintain BP ► Remove clothing ► Obtain immediate CT Scan ► Monitor VS, LOC, O 2 sats, cardiac rhythms, Glasgow Coma Scale, pupil size and reactivity.

Acute Care ► Maintain patient warmth ► Reassure patient and family

Ischemic Cascade ► Series of events in response to thrombotic and embolic strokes. § Ischemic area becomes discolored and soft, initially. However, around the border there is an area of perfusion called the ischemic penumbra that maintains perfusion for 3 to 6 hours post stroke. § If adequate blood flow is reinitiated during this period, less neuro damage results

Treatment ► Control fluid and electrolyte balance § Adequate hydration promotes perfusion to the brain; however over hydration may increase cerebral edema! § Total intake (oral, tube feedings, IV etc. , 15002000 per day) § Monitor urine output ( if ADH released urine output will decrease)

Treatment ► IV solutions with glucose and water are avoided. (hypertonic solutions may increase cerebral edema) ► Increased ICP from cerebral edema peaks in 72 hours and may cause brain herniation.

How to manage ICP ► Enhance venous drainage by: § Elevating HOB § Maintain head and neck in alignment § Avoidance of hip flexion Limit cerebral tissue metabolism and vasodilation by: avoiding hyperthermia, avoiding hypervolemia, manage constipation
 § Mannitol (Osmitrol) § Lasix, (Furosemide) § Dexamethasone")
Medications ► Diuretics (decrease cerebral edema) § Mannitol (Osmitrol) § Lasix, (Furosemide) § Dexamethasone for patients with vasogenic edema
 - to re-establish")
Drug Therapy ► Thrombolytic therapy § Recombinant tissue plasminogen activator (t-PA) - to re-establish blood flow and prevent cell death for patients with ischemic strokes. § Patients who receive t-PA within 3 hours after a stroke more likely to have 32% less injury three months after stroke. § T-PA works by lysis thrombus/clot by binding and digesting the fibrin and fibrinogen.

t-PA Clot specific ► Less likely to cause hemorrhage as compared to streptokinase or urokinase. ► Single most important factor is timing!!!

t-PA ► Patients are screened for coagulation disorders, GI bleeding, and hemorrhagic stroke before initiation of treatment. ► Major side effect is cerebral hemorrhage. ► Monitor VS during treatment/ control BP ► O anticoagulants or antiplatelet drug for 25 hours post treatment.
, clopidrogel (Plavix), dipyridamole (Persantine). ►")
Platelet inhibition/anticoagulant therapy ► Heparin, coumadin, aspirin, ticlipidine (Ticlid), clopidrogel (Plavix), dipyridamole (Persantine). ► Contraindicated for patients with hemorrhagic strokes ► Monitor PT/ PTT ► Monitor patient for bleeding

Drug therapy ► Calcium channel blockers are given for patients with hemorrhagic strokes. ► Excess intracellular calcium may be harmful to brain tissue. ► Nimodipine (Nimotop) decreases effects of vasospasm and minimizes tissue damage. ► Aspirin decreases platelet aggregation at site of plaque.

Drug therapy ► Tylenol treats hyperthermia ► Dilantin may be given for seizures
- Slides: 70