Centrally acting analgesics Opioids Biomedicine spring 08 Year

Centrally acting analgesics Opioids Biomedicine spring 08 Year 2 no 2 Frågor till karsten@narkos. se

Pain medication l Paracetamol l NSAIDs l Opioids l Steroids, radiation, TENS, acupuncture

Physiology l Afferent, peripheral nerves C and Ad l C-fibres 0, 5 -1, 5 mm, <1 m/s, unmyelinated l Ad-fibrer 1 -5 mm, 5 -35 m/s, myelinated (larger Ab touch, vibration, proprioception)


Pain pathways l Tissue damage releases bradykinin, serotonin, histamin, lactate, ATP, ADP, potassium (among others) l Glutamate (excitatory) transmittor in dorsal horn synapse l GABA (inhibitory) transmittor interneuron

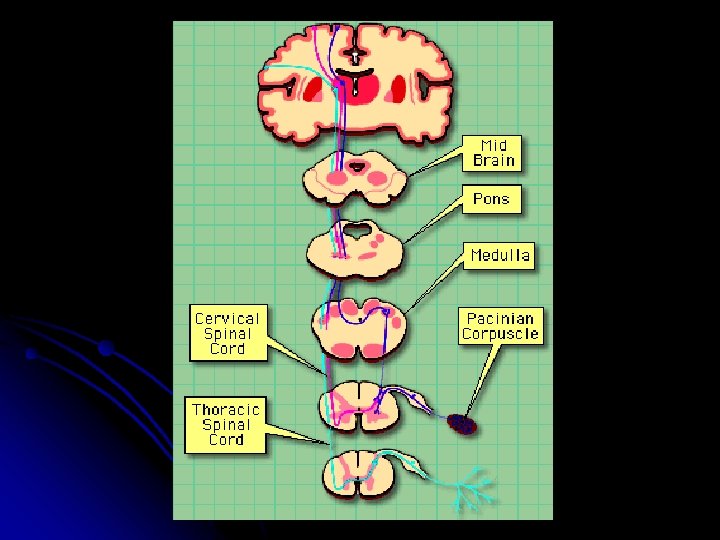
Pain, pathways l l l Nociceptive neurons in dorsal root ganglion Relays via tractus spinothalamicus, spinomesencephalicus and spinoreticularis Reaches thalamus and pons Connects to cortex Inhibitory neurons Inhibitory mechanoreceptors

Pain, pathways l Brain - upwards probably glutamat main transmittor l Downwards neurons GABA, ACh, monoamines (serotonin, NA, DA).

Endogenous opioids l Endorphin, enkephalin, dynorphin l Spinal tract dynorphin interneuron, enkephalin downward inhibitory neurons. l In brain around ”pain centre” but also in areas not involved in nociception and nonneuronal tissues

, d, k")
Opioid receptor Receptors in brain and spinal cord l 4 subtypes: m(my), d, k and NOP (ORL-1) l

Opioid receptor G-protein l Intra/extracellular, intramembranous l Pre- and postsynaptic membranes l

NMDA-receptor N-metyl-D-Aspartate l Learning l Activation makes spinal neurons more sensitive to pain stimulus l Long-term C-fiberstimulation activates NMDA central sensitisation l NMDA-antagonists l

Glutamat l Presynaptic ion channel calcium influx glutamat release l Crosses synapse and binds to NMDAreceptors postsynapticly depolarisation hyperexcitability in nociceptive neurons


Pre- and postsynaptic binding l G-protein inhibits adenylate cyclase l Lower content intracellular c. AMP l Opens K+, inhibits Ca 2+ l Inhibits pre-synaptic release of glutamat

The opioid receptor

The opioid receptor m, d, k l identical around 70% l G-protein binds to 3 rd receptor loop l
 l l l l l Mainly analgesic effects Respiratory")
The opioid receptor m (mu) l l l l l Mainly analgesic effects Respiratory depression Nausea / vomiting Constipation Cough reflex Euphoria Addiction Sedation Most analgesic opioids are m-agonists
 l Probably effects outside the CNS l Some analgetic")
The opioid receptor d (delta) l Probably effects outside the CNS l Some analgetic effekts l Seizures? l Least knowledge
 l Analgesia on mainly spinal cord level l Nausea")
The opioid receptor k (kappa) l Analgesia on mainly spinal cord level l Nausea and dysphoria l Psychotomimetic effects – limits abuse potential

 Less CO")
Side effects - mechanisms l l Respiratory depression Respiratory centre (medulla oblongata) Less CO 2 stimulation Decreased respiratory rate Nausea / vomiting Area postrema (medulla oblongata) (triggerzone vomiting reflex) Stimulation of DA-receptors Stimulation mechano/chemoreceptors GI tract

Side effects - mechanisms l Constipation peripheral and central affection less GI movement and increased tonus No tolerans Laxatives necessary Peroral naloxone possible l Itching Histamine release or centrally mediated

Side effects - Mechanisms l Sedation Overdose Wrong strategy Sleep dept

 morphine, metadon, fentanyl, heroin l Partial agonists buprenorfin, kodein, tramadol")
Drugs l Agonists (m-receptors) morphine, metadon, fentanyl, heroin l Partial agonists buprenorfin, kodein, tramadol l Antagonist naloxone
 or synthetic l Morphine like effekts, inhibited")
What is an opioid? l Alkaloid (plant) or synthetic l Morphine like effekts, inhibited by naloxon

Opium l Narcotic resin from opium poppies: morphine 10%, noskapin 6%, papaverin 1%, kodein 0, 5%

History l 3400 BC Opium puppies grown in Mesopotamia l 460 BC Hippocrates medicine (psychiatric disease and epidemies)

History l 330 BC Alexander the Great introduces opium to Persia and India l 400 AD Opium with traders to China l Parcelsus (1490 -1541) opium as medicine l Laudanum (opium, sherry, cinnamon, clove bud oil, saffron) 17 th century

History Morphin 1806 l Kodein 1832 l Heroin 1832 l

")
Morphin l l C 17 H 19 NO 3 Greek. Morpheus (God of dreams) 1806 from opium 1956 chemical structure
 Distribution")
Morphine l l l Half life 2 -4 hours Bioavailability 10 -50% (30%) Distribution volume 3 L/kg Bioaactive morphine-6 -glucuronid (kidneys) M 6 G half life 4 -15 hours

Heroin l l l l C 21 H 23 NO 5 (morphin C 17 H 19 NO 3) Higher fat solubility Produced 1874 Bayer 1899 Drug Sweden until 1964 Half life 30 minutes Morphine
")
Kodein C 18 H 21 NO 3 (morfin C 17 H 19 NO 3) l Produced 1832 l Low receptor affinity l 10% into morphine M 6 G l 7 -10% non-responders l Half life 2 -4 hours. l 10 mg morfin Kodein 60 mg l
 hours l Active metabolite norpropoxyfen l Metabolite half")
Dextropropoxifen Half time 8 -18 (90) hours l Active metabolite norpropoxyfen l Metabolite half life 30 -45 (100) hours l Alcohol enhances respiratory inhibition l 10 mg morfin 100 mg Dextropropoxifen l

Tramadol Halflife 4 -6 hours l Active metabolite D-desmetyltramadol l Halflife metabolite 9 -12 hours l 5 -10% non-responders l Inhibits reuptake NA / 5 -HT l


Fentanyl ”Complicated kinetics” l Halflife 1 min, 8 tim l Active metabolites unknown l 10 mg morfin 0, 05 mg fentanyl (iv) l

Pethidine l synthetic opioid l Most histamine release. Seizures. l 100 mg 10 mg morphine l Shivering
 l NMDA – receptor antagonist? l Halflife 2 -4 hours l Unknown")
Ketogan Ketobemidon(hydroklorid) l NMDA – receptor antagonist? l Halflife 2 -4 hours l Unknown metabolite activity l Abuse risk l ”Less documented morphine alternative” l ”only” indication renal failure (+NMDA? ) l 10 mg morphine 10 mg ketobemidon l

Oxicodon Halflife 2 -4 timmar l Probably inaktiva metaboliter l 10 mg morfin 5 mg oxikodon l


Metadon NMDA-receptor antagonist ? l Halflife 15 -40 hours l ”Bad reputation” l Advanced pain treatment l

Clinical use Cancer pain l Postoperative pain l Long-term pain ? l Neurogenic pain? l ”Always” in combination with paracetamol and NSAID l Elderly ? l Try not to mix different opioids l
 l Lower conscience l Breathing l")
Intoxication Mios (small pupils) l Lower conscience l Breathing l
 opioid antagonist l reverses endogenous and exogenous substanses and acupuncture")
Antidote – Naloxone (Narcanti) opioid antagonist l reverses endogenous and exogenous substanses and acupuncture l effect within 2 minutes l Iterated l iv + im when abuse overdose l
, shakings, muscular cramps, itching, diarrhea, nausea, vomiting (the")
Abstinence l sweating, fever (”cold turkey”), shakings, muscular cramps, itching, diarrhea, nausea, vomiting (the flu) l At pain treatment because of to quick withdrawal re-medicate!
 60 mgx 2 Tb.")
Cold Case Cancer l Current medication: Tb. Dolcontin (longacting morphine) 60 mgx 2 Tb. Morphine (shortacting) 20 mg as req. inj. Ketogan 5 mgvb Tb. Tramadol 100 mgx 2 l l Pain. What to do?

Patientfall l Patient insatt på Ketogan tablett 5 mgx 6 med god effekt. Översatt till Dolcontin 20 mgx 2. Inkommer efter 1 vecka till akuten: illamående, kräkning Diffdiagnos (opioidrelaterat) ? l Ytterligare status etc? l Vad göra? l


Afterlife …. . l Morphina is currently Golden Standard l Renal failure l Treat pain!
- Slides: 54