Central Nervous System Function of the nervous system








 Which gives the body information about")









 Warmth: Warm receptors (ruffinie’s organ) Central pathway")
 Receptors: Free nerve")







 Abnormal overgrowth of neuroglial tissue associated with cavitation around")





. “final common pathway” for")

. • Muscle tone •")


 Caused")
- Slides: 54
Central Nervous System
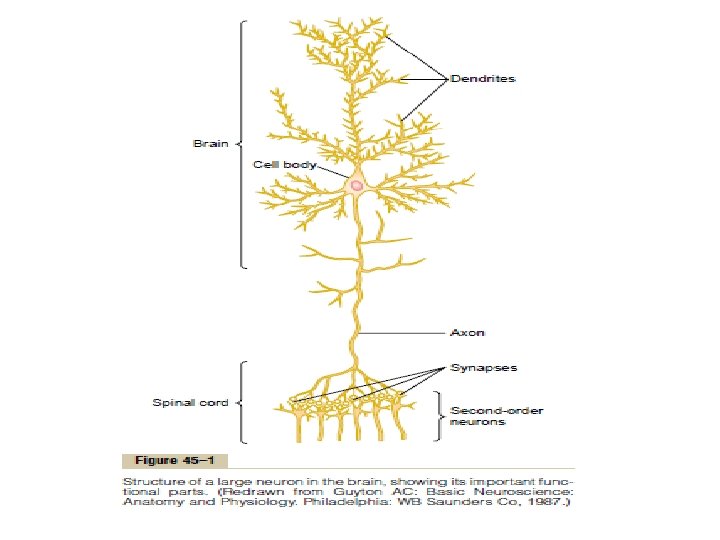
Function of the nervous system • It receives each informations from the different sensory nerves and sensory organs and then • Integrates all these to determine the body responses. • control the various bodily activities The Basic Functional Unit CNS contains more than 100 billion neurons • Input signals Enter the neuron through synapses located on the neuronal dendrites, and the cell body. • Output signals Travels by way of a single axon leaving the neuron
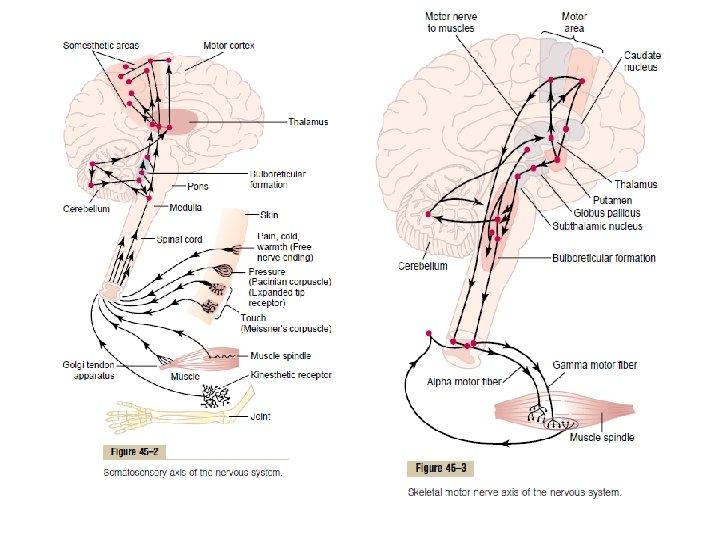
Sensory Part of the Nervous System—Sensory Receptors Most activities of the nervous system are initiated by • Sensory experience → Exciting sensory receptors Causing Immediate reactions from the brain or memory Motor Part of the Nervous System—Effectors • contraction of appropriate skeletal muscles throughout the body • contraction of smooth muscle in the internal organs • and secretion of active chemical substances by both exocrine and endocrine glands in many parts of the body.
Neurological Examination Systemic approach Regional approach Neurological examination is divided in to several components, each focusing on a different part of the nervous system: • General examination • Sensory system examination • Cranial nerves examination • Motor system examination • Cerebellar functions and coordination • Tests of vestibular system
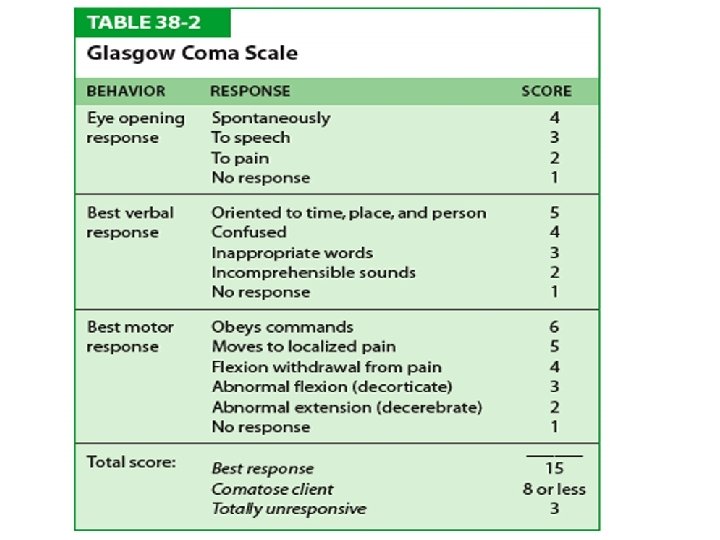
I- General examination 1 - Awareness The level of consciousness may be graded in to • • Normal Drowsy but responds to commands Very drowsy and responds only to painful stimuli Comatose 2 - Memory can be tested by simple questions • Date , full name, Age, address, what the patient hade for breakfast • Digital attention can be tested by reciting a sequence of 5 or 6 numbers and asking the patient to repeat them • Solve simple mathematical problems
I- General examination Handiness Rt or lt handed Speech • Characters of speech • Fluency of speech • Ability to understand carry out simple or complex commands • Read and write Disorders of speech may be • Stutter • Dysarthria • Aphasia
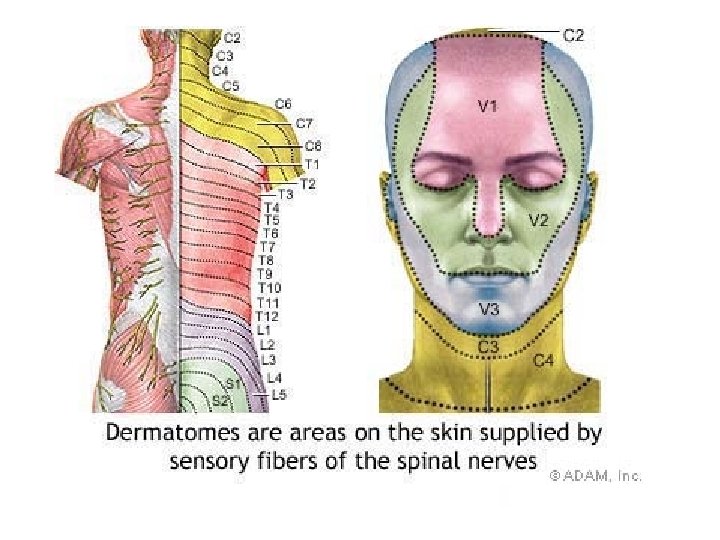
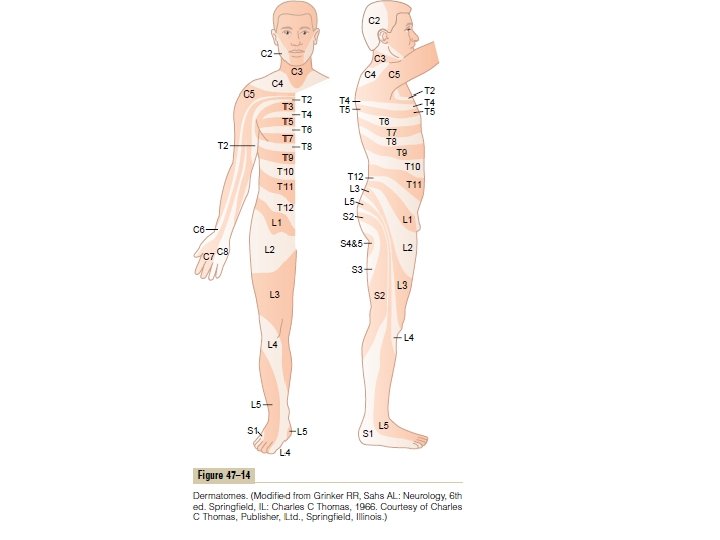
II-Examination of the sensory system Sensory examination involves • Evaluating different types of sensation • Compare the response in different parts or opposite sides of the body Anatomical representation of the various spinal segments on the skin face 5 th cranial nerve neck C 2, 3, 4 arms C 5 to T 3 Trunk T 4 to 8 abdomen T 8 to 12 Leg front L 2 TO L 5 Leg back S 1 to S 3 Genitalia S 2, 3 Perianal region S 4
CLASSIFICATION OF SOMATIC SENSES A- the mechanoreceptive somatic senses • Tactile 1. Touch 2. Pressure 3. Vibration 4. Tickle senses • Position 1. Static position 2. Rate of movement senses That are stimulated by mechanical displacement of some tissue of the body B- thermoreceptive senses which detect heat and cold C- the pain senses which is activated by any factor that damages the tissues.
Other classification A- Cotaneous sensations (superficial or exteroceptive) Which gives the body information about external events (skin sensations) • Temprature • Pain • Touch - Crude touch - Fine touch→ a- tactile localization b- tactile descrimination B- Deep sensation Which refer to innate bodily sensations from skeletal muscles, tendons, joints, bones and ligaments • Proprioceptive sensation - Sense of position - Sense of the rate of movement • Pressure sense • Muscle tension sense C- Combined senses • Steriognosis • Vibration sense
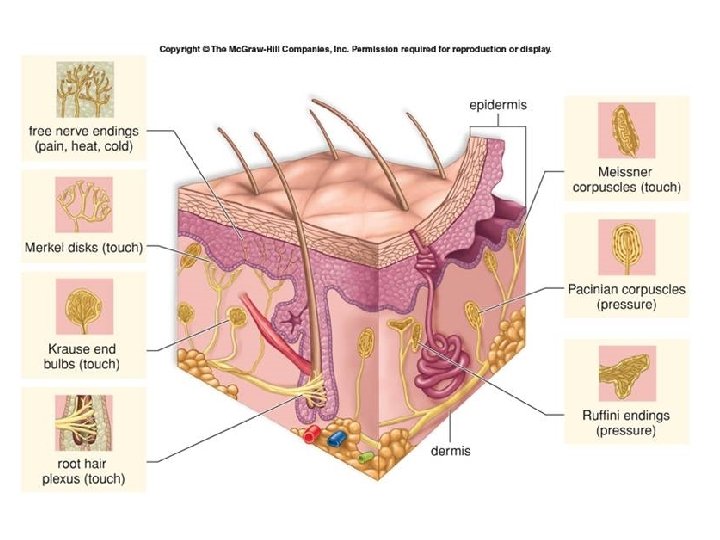
Classification of Sensory Receptors A- Mechanoreceptors 1 - Skin tactile sensibilities - Free nerve endings - Merkel’s discs - Ruffini’s ending - Meissner’s corpuscle - Krause’s corpuscles - Hair end-organs 2 - Deep tissue sensibilities - Free nerve endings - Ruffini’s ending - Pacinian corpuscles - Muscle spindle - golgi tendon organ B- thermoreceptors C- Nociceptors Free nerve endings
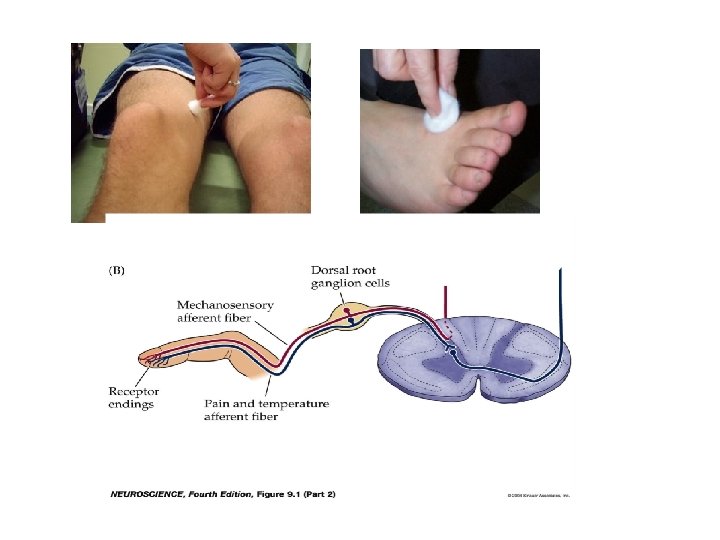
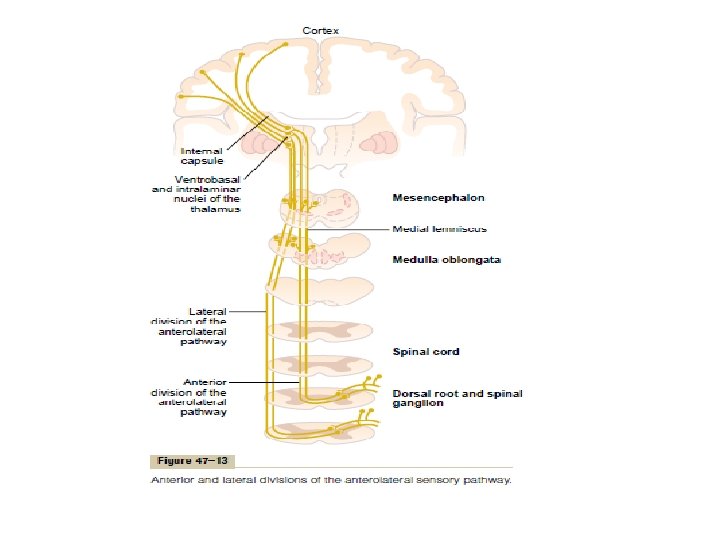
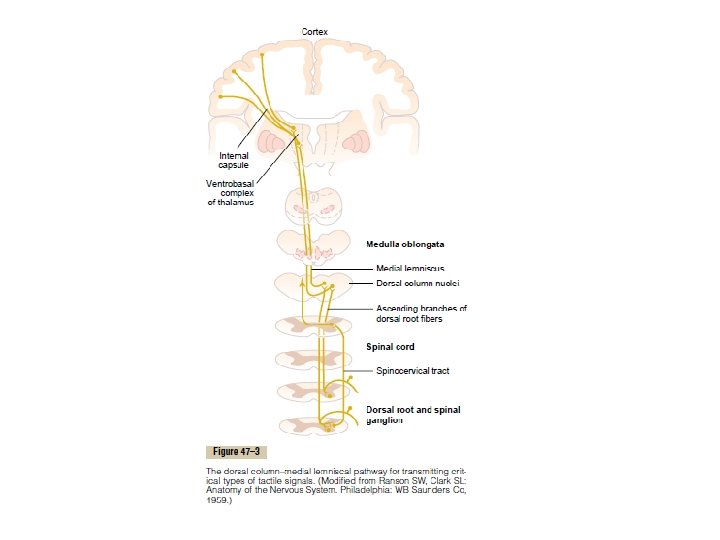
Sensory Pathways for Transmitting Somatic Signals into the Central Nervous System sensory information from the somatic segments of the body enters the spinal cord through the dorsal roots of the spinal nerves → from the entry point into the cord → to the brain THROUGH A- the dorsal column–medial lemniscal B- the anterolateral system Composed of large, myelinated nerve fibers composed of smaller myelinated fibers Transmit signals to the brain at velocities transmit signals at velocities ranging of 30 to 110 m/sec from a few meters per second up to 40 m/sec. has a high degree of spatial orientation of the nerve fibers has much less spatial orientation
Transmit discrete types of mechanoceptive sensation transmit a broad spectrum of sensory modalities— pain, warmth, cold, and crude tactile sensations 1. Touch sensations requiring a high degree of localization of the stimulus 2. Touch sensations requiring transmission of fine gradations of intensity 3. Phasic sensations, such as vibratory sensations 4. Sensations that signal movement against the skin 5. Position sensations from the joints 6. Pressure sensations having to do with fine degrees of judgment of pressure intensity 1. Pain 2. Thermal sensations, including both warmth and cold sensations 3. Crude touch and pressure sensations capable only of crude localizing ability on the surface of the body 4. Tickle and itch sensations 5. Sexual sensations
I-Touch sensation Results from stimulation of tactile receptors in the skin or in tissues immediately beneath the skin A-Crude touch Poorly localized gross tactile sensation Receptors: • Free nerve endings • hair end-organ • Ruffini’s end-organs (heavy prolonged touch) Afferent nerves: • A- delta nerve fibers that conduct at velocities of only 5 to 30 m/sec. Central pathway: Ventral spinothalamic tract Partly in gracil and cuneate tracts Test: With the patient eyes are closed strick the skin lightly with a piece of cotton
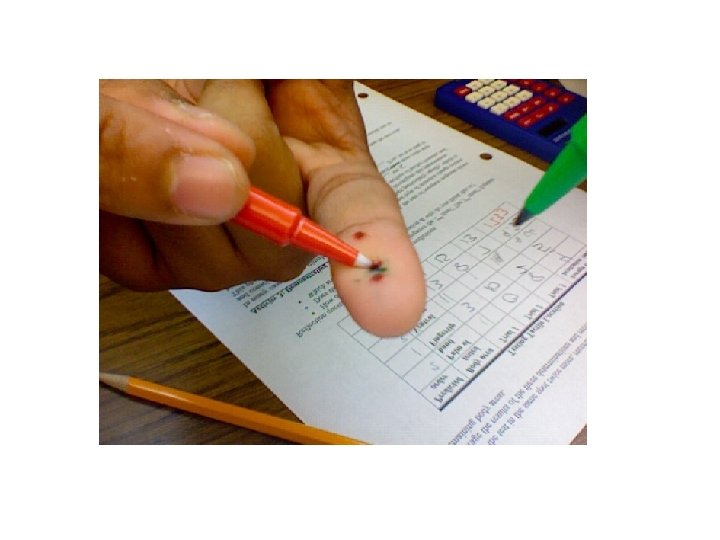
B-Fine touch Receptors • Meissner’s corpuscle: highly sensitive • Merkel’s discs Localize touch sensation to specific surface areas of the body Determine the texture of what is felt Afferent nerves: A-beta nerve fibers Central pathway: Gracil and cuneate tracts 1 - Tactile localization It’s the ability to localize a touched skin point while the eyes are closed. Test Ask the patient to close his eyes Touch the skin lightly with a marker pencil Ask the patient to touch the stimulated point by another pencil The closer the 2 touch point to each other, the more accurate is the localization
2 -Tactile discrimination It’s the ability to perceive 2 touch stimuli applied simultanously to the skin as 2 separate points of touch with closed eyes. Test While the patient close his eyes using weber compass, touch the skin with the two blunt points of a weber compass starting by the two points are wide apart then the distance between them is decreased gradually till finding the two point threshold 3 - stereognosis It’s the ability to recognize the nature of objects by handling them without using vision, from their shapes, size and weight Test With closed eyes ask the patient to recognize the nature of a familiar object e. g coin, key
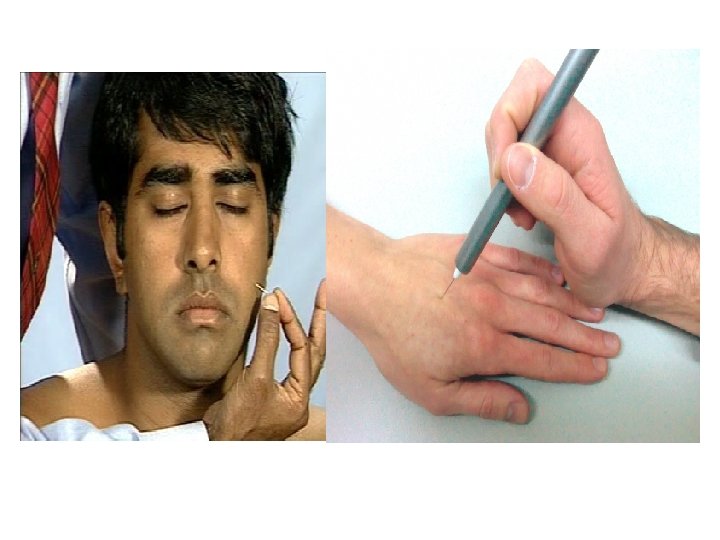
Pain sensation Pain: is a specific unpleasant sensation produced by any noxious stimulus Receptors: Nociceptors Free nerve endings Central pathway: Lateral spinothalamic tract which consists of A-Paleospinothalamic tract for slow pain B- neospinothalamic tracts for fast pain C- trigeminal nerve for the face Test With closed eyes, brick the skin with a pen at different pressure side with side, proximal with distal segment with segment to identify the areas of sensory impairement Or Heating the subject skin and recording the temprature at which pain occurs (normal pain threshold is 45 c)
Temperature sensation Receptors: Cold receptors (Krause’s organ) Warmth: Warm receptors (ruffinie’s organ) Central pathway : Lateral spinothalamic tract Test : With closed eyes ask the patient if he is being touched with test tube containing hot 45 c or cold 30 c water
Pressure sensation Results from deformation of deeper tissues A-Pressure (crude pressure) Receptors: Free nerve endings Ruffini’s end organ present in the skin Central pathway: Venral spinothalamic tract Test Applying weak pressure on the part to be tested B- deep pressure Receptors: Pacinian corpuscle Ruffini’s endimg Central pathway: Gracil and cuneat tracts
B- deep pressure Test Asking the subject to differentiate between various weights without lifting them By placing different weights on the supported hand with closed eyes Muscle tension sensation The sensation evoked by traction on the tendons Receptors Golgi tendon organ Central pathway Gracil and cuneate tracts Test Discrimination of weights during lifting them Ask the subject to differentiate between various weight in his unsupported hands while closing eyes
Proprioceptive sensation Receptors: Muscle spindle and golgi tendon organ Ruffinis endings Pacinian corpuscles Central pathway: Gracil and cuneat tracts A- sense of position Concious perception of the position of different parts of the body with respect to each other Test With closed eyes, place one of the patient’s limbs, toes or fingers in unusual position Then ask him to place the corresponding part in the other side in similar position
B-Sense of passive movement This is the sensation of movement of joints Test With closed eyes, the examiner move one of the patient’s fingers or toes Then ask the patient to determine the start, the end, rate and direction of movement
Vibration sensation Results from rapidly repetitive sensory signals Receptors: • Pacinian corpuscles: signal vibrations from 30 to 800 cycles per second • Meissner’s corpuscles: Low frequency vibrations from 2 up to 80 cycles per second Central pathway Gracil and cuneate tracts Test Apply the base of a vibrating tuning fork on a bony prominence e. g lower end of radius or one of the two maleoli
The sensory pathways 1 - anterolateral system Consists of type A – delta and C nerve fibers Conduct signals from the opposite side A- ventral spinothalamic tracts Transmit – crude touch - crude pressure - itch and tickle sensation B- lateral spinothalamic tract a – paleospinothalamic tract Transmites slow pain and crude thermoceptive sensation B – neospinothalamic tract Transmits fast pain and fine thermoceptive sensation
Dorsal column or lemniscal system it concists of type A-alpha and A- beta nerve fibers It transmits mainly fine sensation from the same side of the body Gracil and cuneate tracts
Abnormal finding of sensation • Glove and stocking type Loss of all sensations in a symmetrical and distal distribution • Mononeuropathy Loss of all sensation in the distribution of one peripheral nerve • Root lesion Loss of all sensation in a dermatome • Dorsal column or its afferent nerves lesion Loss of vibration and proprioceptive sensations glove and stocking sensory impairment
• Central cord (syringomyelia) Abnormal overgrowth of neuroglial tissue associated with cavitation around the central canal of the cord The lesion usually affect the lower cervical and upper thoracic segment Dissociated sensory loss • Bilateral loss of pain and temperature sensation • Fine tactile and proprioceptive sensation are preserved
• Brown sequard syndrom Transection of half of spinal cord Contralateral loss of pain and temprature sensation Ipsilateral loss of proprioceptive and vibration sensations
• Transection of the cord Bilateral loss of all sensations below the lesion
• Thalamic lesion Loss of all sensation on the opposite side of the lesion • Sensory cortical lesion Loss of cortical sensations on opposite side with decrease in other sensations
Tabes dorsalis Attacks of sever sharp pain Degeneration of the gracil and cuneat tracts - Loss of fine tactile sensation and the vibration sense - Loss of concious proprioceptive sensation → sensory ataxia
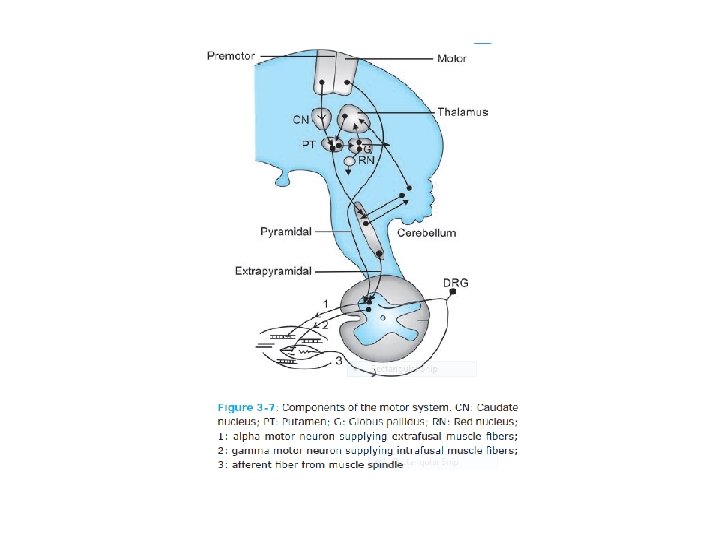
III-Examination of the motor system Types of Motor Activities • Muscle tone and reflexes; mostly spinal mechanisms (involuntary) • Gross and fine, skilled movement (voluntary) • Semiautomatic movements (e. g. chewing, swallowing, swinging of arms while walking). no clear cut demarcation between voluntary and involuntary movements COMPONENTS OF THE MOTOR SYSTEM • motor areas of cerebral cortex • subcortical structures (basal ganglia, cerebellum, reticular formation, vestibular nuclei) • descending motor tracts (the so-called upper motor neurons (UMN), lower motor neurons (LMN)) • the skeletal muscles.
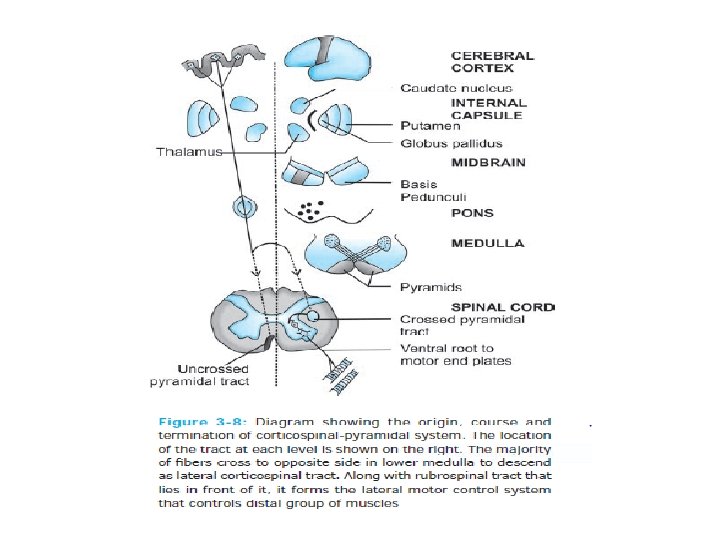
Component of the motor system • Lower Motor Neurons (LMN). “final common pathway” for all motor signals that leave the CNS on their way to skeletal muscle. The anterior horn cells of spinal cord and the motor cranial nuclei in the brainstem that directly innervate the skeletal muscles. • Upper Motor Neurons (UMN). the descending motor fibers are classified into pyramidal and extrapyramidal. 1. Pyramidal tract all fibers descending in the pyramids of the medulla (corticospinal tract) 2. Extrapyramidal tracts (from basal ganglia, etc. ) that indirectly control LMN
Planning and Execution of Movements
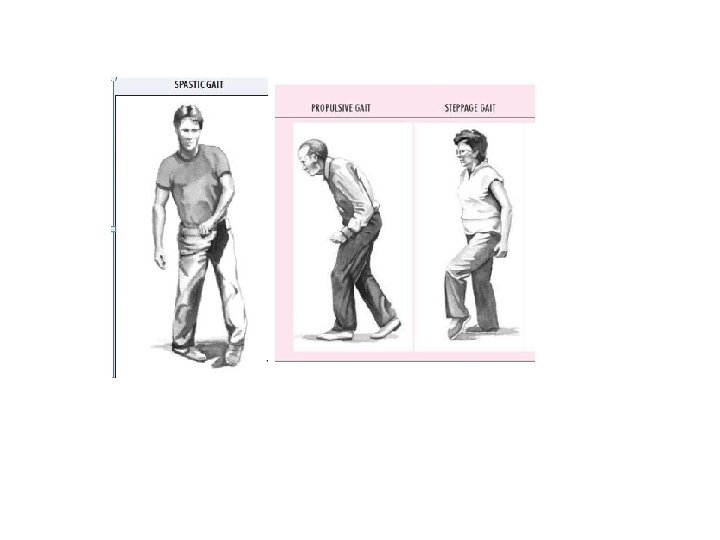
TESTING THE MOTOR FUNCTIONS • Nutrition or bulk (muscle status). • Muscle tone • Power or strength • Presence of abnormal movements • Gait. • Reflexes • Coordination of muscular activity Gait and posture Stance: the way of standing on one’s two feet gait: the manner, style, or pattern of walking. To examine the gait Exclude bone and joint diseases The legs and feet should be exposed Ask the patient to walk away from you and turn around toward you and walk along a straight line
TESTING THE MOTOR FUNCTIONS Some forms of abnormal gait are • Hemiplegic posture and gait • Stamping gait • Shuffling gait • Drunker gait
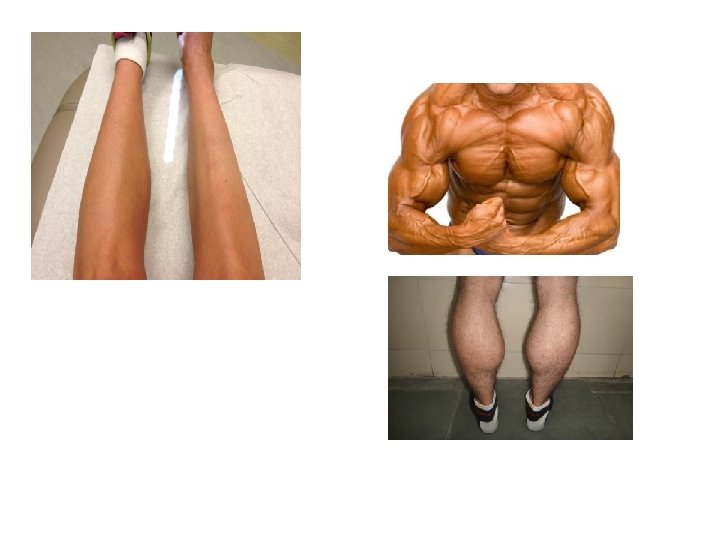
TESTING THE MOTOR FUNCTIONS Muscle status This can be estimated by • Inspection • Palpation • Measuring the circumference of the limbs with a tape measure at certain points, and comparing them on the two sides. In the upper limb the circumference is measured 5 inches above the elbow and 4 inches below it. In the lower limb the circumference is measured 9 inches above the knee and 6 inches below it.
TESTING THE MOTOR FUNCTIONS § Muscle atrophy: muscle mass decrease (smaller and softer) Caused by: generalized: cachexia localized: disuse atrophy lower motor neuron disease § Muscle hypertrophy: muscle mass increase Caused by: muscular exercise certain manual work muscle dystrophy and pseudohypertrophy