Central Division OEC Instructor Continuing Education Clinic Location






 Human Relations & Communication (Qualities of")
")
































































 Sight, Limb, Paralysis, Hearing. ADA")

- Slides: 79
Central Division OEC Instructor Continuing Education Clinic Location: Chula Vista Resort
Instructor Re-Certification Instructors: Sue Hayes Jeff Olsen Gary Clark Saturday, September 8, 2018
Objectives Review Website sign-in navigation and information tools. Review components of Instructor Development and Adult Learning. Continuing Ed and Spinal Motion Restriction (The Backboard Redefined) Describe the layout of the current OEC curriculum and resources available for teaching Pearson My Lab & Mastering. Identify the role expectations of OEC instructors.
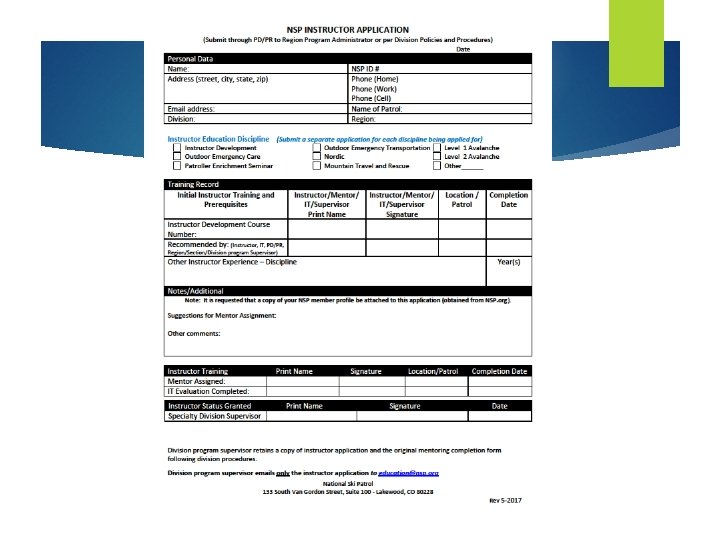
Instructor as Administrator
Instructor online tools Please see the NSP Course Tools documentation HERE
Instructor Logs Be sure to turn yours in today!
Educating groups How Adults Learn (different learning styles) Human Relations & Communication (Qualities of Effective Instructors) Lesson Planning (6 -Pack) Lesson Content/Instructor Resources Monitoring/Evaluation Helping others become instructors Mentoring Program
How Adults Learn (different learning styles)
Video https: //youtu. be/3 Ld. Ew. YDDJBg
Human Relations & Communication Three communication qualities of effective instructors… They have excellent listening skills They are good at interpreting and sending non-verbal communication They provide constructive feedback to their students in a positive manner
Lesson Planning / 6 Pack The Beginning The Heart The Ending The Set The Content Delivery The Student Summary The Concluding Objectives The Learning Activities Monitoring and Evaluation
6 Pack should be taught 1 Topic at a time Topic 1 6 Pack on a Splint • Show Immobilization • A ridged Splint • A traction Splint • A sling Topic 2 6 Pack on CMS Topic 3 6 Pack Reposition • Circulation • Is the Pulse Present • Motion • Can it be moved • Sensation • How many moves • What if it doesn’t work When you teach a 6 Pack 1 topic at a time, and then combine them retention with the candidate is much higher.
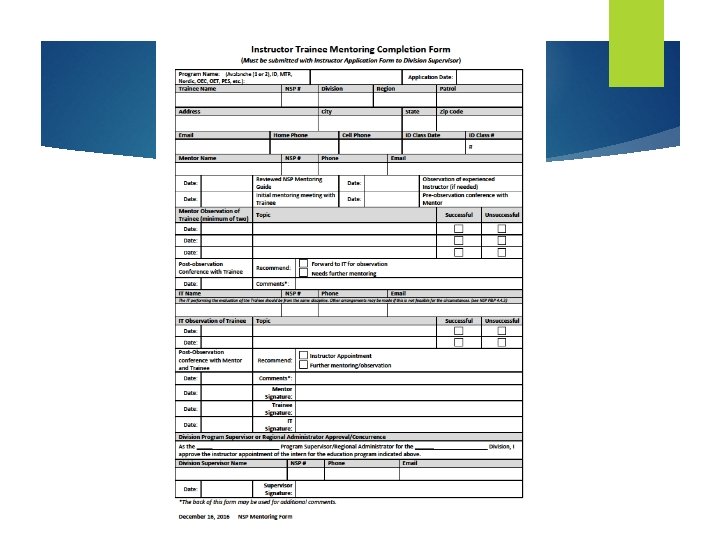
Instructor as a Mentor Is a certified discipline-specific instructor. Possesses exceptional abilities in needs assessment and communication Establishes mentoring relationships with assigned instructor trainees. Provides assessment and determines instructor trainee’s readiness to teach in a specific discipline. Maintains records of meetings and observation assessments. Recommends instructor trainee for Instructor Trainer observation and certification. http: //nspwr. org/programs/oet. php
2017 Division Spring Meeting Language Change Approved “The expectation is that the final observation and sign off for a new OEC instructor be done by an OEC IT from an outside patrol”. “Any exceptions to that must be approved by a candidates mentor in discussion with the ROA and the RD”.
2017 Division Spring Meeting Language Change Approved “The expectation is that the final observation and sign off for a new OEC instructor be done by an OEC IT from an outside patrol”. “Any exceptions to that must be approved by a candidates mentor in discussion with the ROA and the RD”.
National Ski Patrol Continuing Education SPINAL MOTION RESTRICTION THE BACKBOARD REDEFINED
This is Ski Patrol, how can I help…… Radio Call: “Ski Patrol, there has been a bad crash on the slope under the chair. The skier launched and landed really hard on his back and now is laying still in the middle of the slope. He had to have been 20 feet in the air. ”
Recommendation of NSP Medical Committee Spinal Motion Restriction, where backboards with straps are used to secure a conscious victim of trauma during extrication and transport for a possible spinal injury, may be overused or sometimes unnecessary. National Medical Advisory Committee white paper presented to the NSP Board of Directors at Powderfall 2017. Updated August 9, 2018 with the article written in the Prehospital Emergency Care journal.
NSP website-OEC Education Resources
Recommendation of NSP Medical Committee Securing a conscious injured person to a backboard has potential consequences. The patient is subject to pain, apprehension, potential injury to skin from pressure points and some limitations of airway protection when supine (especially if the person vomits)
UPDATE TO OEC 5 This information will be used as a clarification of the standard of training for the NSP Outdoor Emergency Care program (OEC 5 th edition). Patrols are required to follow local or state EMS guidelines, policies or law that would supersede this level of training
Spinal Update Assessment: Use of a Backboard usage in pre-hospital setting has changed Evidence based medicine has shown many patients may not need a hard board May cause additional problems
Use of backboards inline with evidence based medicine Physical application of a backboard is done the same way. Assessment of who goes on the backboard has been clarified. Patrollers using a complete and comprehensive assessment will be better in line with evidence based medicine. If you think about it a backboard does not immobilize an injured persons spine. It only offers SPINAL MOTION RESTRICTION.
Considerations when Assessing for Spinal Protection MECHANISM OF INJURY RELIABILITY OF THE ASSESSMENT RESULTS OF THE EXAM
Concluding Objectives Define what is a spinal protection device: i. e. . Backboard, gurney, vacuum mat, ambulance cot Explain when it is appropriate to use a spinal motion restriction device List and describe examples of some potential significant Mechanisms of Injury for a spinal injury Describe the observations and questions that make up the Reliability of Assessment List the specific items that make up the careful physical exam Demonstrate how to perform a careful physical exam
Concluding Objectives continued Explain what to do when a complete and detailed exam is not possible on the hill Explain the appropriate time and use of a standing backboard List when spinal motion restriction is not needed
Spinal Motion Restriction and the use of a backboard Background: The factual material in OEC 5 e is not wrong. The assessment associated with spinal motion restriction for specific patients must be improved. In particular: The identification of mechanism of injury The evaluation of reliability of assessment Focus on a careful physical exam from the occiput to the coccyx in persons with potential spinal injury
What is a spinal motion restriction device Spinal motion restriction: avoid further injury and to provide comfort. Spinal motion restriction : transfers should be done with careful attention to limiting spinal motion For persons with significant potential for spinal injury a Spinal motion restriction device in many cases is a backboard (and a collar ) However it could also be direct use of a gurney, toboggan or vacuum mat (with collar) Each of these must also include padding and bracing to fill voids and limit movement both laterally and axially. .
Spinal Motion Restriction is required when there is: Exam findings associated with a potential spinal injury. MOI with significant potential for spinal injury WITH an alteration of the mental status such that a reliable physical exam cannot be done. Multiple injuries in an unresponsive trauma patient. A patient who has become unresponsive, without a witness present, so the mechanism of unresponsiveness is unknown.
Determining the use of SMR
Physical exam The physical exam is not different from the current physical exam. In this case we are focusing on what needs to be evaluated as it relates to Neurological, neck and/or Spine injury A full exam is required as with every trauma assessment this is highly focused for the training.
Assessment of a Patient with a Suspected Neurological, Neck, and/or Spine Injury: Mechanism of Injury
Potential Significant Mechanism of Injury Ø High speed collision of skier/rider with a fixed object (high impact trauma) Ø Falling from a ski lift Ø Avalanche burial Ø A fall greater than 2. 5 -3 times a patient’s height
Potential Significant Mechanism of Injury Ø A high-speed motor vehicle accident with a fatality, ejection from the vehicle, or an unrestrained passenger Ø A pedestrian or bicyclist struck by a motor vehicle Ø A major bicycle or motorcycle accident Ø High voltage electrical shock or lightning strike Ø Other serious mechanism of injury
Potential Significant Mechanism of Injury
Assessment of a Patient with a Suspected Neurological, Neck, and/or Spine Injury: Reliability of Assessment • Are they alert and oriented, responding normally to a verbal command? • Can they respond appropriately when asked about a sensory stimulus such as “can you feel me touching your toes? ” • Can you rule out intoxication or altered mental status? • Can the patient respond to your questions and exam? • Can the patient focus on your questions rather than a distracting injury? • Can a younger pediatric patient answer your questions appropriately?
Reliability of Assessment
Results of the Exam Ø Perform a thorough physical exam looking for: Ø Deformity or step-off of the spinal alignment Ø Midline tenderness over the spine (not flank or rib tenderness) Ø Loss of sensation (numbness) or motor function distal to a possible spinal injury
Results of the Exam Ø Flexor or extensor posturing to painful stimuli Ø Skull depression or fracture Ø Cerebral spinal fluid leak from the nose or ears Ø Sacral or posterior pelvic pain when side-to-side compression is performed
Detailed and complete physical exam If the Exam reveals any of these Needs SMR Including ccollar and head blocks.
Thorough and complete Physical Exam Review: Types of Spinal injuries Review: Types of Skull fractures Signs and Symptoms of Spinal Cord injuries Assessing a Suspected Neurological Injury of the Neck and/or Spine
Types of Spinal Injuries Para spinal soft tissue injuries - muscles Bony fractures Spinal cord injuries Spinal disc/nerve injuries
Types of Skull Fractures Linear: Basilar: Single non-displaced fracture line. Occurs along the floor, or base, of the skull. Usually presents with significant soft-tissue swelling and tenderness of the scalp Fairly common in high-velocity blunt MOI such as when a skier strikes a tree. Depressed: Comminuted fracture with displacement resulting in a characteristic “soft spot” Depending on force of injury, fracture fragments may or may not intrude on the underlying brain tissue
Signs and Symptoms of Spinal Cord Injuries Ø Sensory impairment Ø Ø Motor impairment Ø Ø Weakness, paralysis Neurogenic Shock Ø Ø Numbness, tingling Low blood pressure Death
Assessing a Suspected Neurological Injury of the Neck and Spine Checking Level of responsiveness Pupillary exam Best motor response (GCS) which would include: Patient follows commands Localized pain Withdraws from pain Flexor posturing Extensor posturing
Assessment of the Potential Spinal Injury
Assessment of the Potential Spinal Injury
Step Off Deformity
CMS Check
CMS Check
Posturing, a response to painful stimuli indicates the need for spinal protection: Decerebrate-extensor posturing
Posturing, a response to painful stimuli indicates the need for spinal protection: Decorticate-flexor posturing
Assessment of a Patient with a Suspected Neurological, Neck, and/or Spine Injury: Results of the Exam Spinal protection is REQUIRED when there is: Exam findings associated with a potential spinal injury. Mechanism of injury with significant potential for spinal injury WITH an alteration of the mental status such that a reliable physical exam cannot be done. Multiple injuries in an unresponsive trauma patient A patient who has become unresponsive, without a witness present, so the mechanism of unresponsiveness is unknown.
In the rare instance when a complete and detailed exam is not possible on the hill Use a backboard (with collar) with full immobilization as a transportation device Take the patient to the first aid room for further evaluation Complete a thorough and detailed evaluation If no spinal protection is warranted the backboard can be removed according to state and local protocol, and regulations.
The use of Standing Backboard Rarely used. Only used when necessary and indications are appropriate. Can be used as a transportation device when someone that has no physical findings but states “their back hurts” and needs to get off the hill.
Spinal motion restriction is not needed Low energy incidents even with minor physical findings (example: a contusion near the spine). “Just in case” there is an injury or a low level of probability. A headache, brief loss of consciousness or concussion in a patient who is now alert and oriented, and has no findings. Patients who are up and walking at the scene with a mechanism of injury with the potential for spinal injury without documented physical findings or symptoms. Penetrating injuries, unless near the midline spine area. “My back hurts, ” without any of the findings noted above.
Student Summary and Resources Review the concluding objectives Use the OEC Cycle B refresher student workbook printed and distributed Use of the Lesson plans for the Cycle B refresher This is a highly focused spinal assessment review Skills on backboards have not changed Use of other spinal motion restriction equipment will take additional training at the local level
Exercise Using the opening scenario complete a patient assessment and pay particular attention to: Identifying MOI of concern Asking questions of reliability of assessment Complete a physical exam with focus and attention on palpation of the head, neck, and back along the midline of the spine trying to identify any pain or abnormalities.
Questions
Instructor Re-Certification continued. Ø Teaching Tips Ø Resources Ø On & Off line Ø Mandatory skill guide Ø Instructor Roles Ø Pearson (Keys) Ø ADA (American Disabilities Act & NSP Training)
OEC Teaching Tips Teach only to the objectives that are outlined in the front of every chapter The material that covers those objectives can be found in the margin of the text OEC Skills in App. B must be signed Teach smaller skill units to achieve better large skill success Change delivery method to meet the needs of the students
Offline Resources Appendix A – Survival: The Rule of Threes Appendix B – Student OEC Skill Guide o Must successfully complete before evaluation Appendix C – Emergency Care Equipment & Common Medications Glossary Answer Key* Index
Online Resources NSP Website Central Division Region MEMBER RESOURCES BOOKSHELF Region Calendar • OEC Refresher Tools • Current Event Release Contact info • OEC Exam Info • OEC Instructor Guides form • OEC-MSP Registration OEC • FAQs • Online Course help • Pearson Instructions
NSP 5 th Edition Mandatory skill guide for certification
ONLINE… Two places you will find a list of the OEC Skills. INSTRUCTOR RESOURCES ON THE NSP SITE AND CENTRAL DIVISION SITE (OEC)
Roles of an OEC Instructor ü INSTRUCTOR v MENTOR v ADMINISTRATOR
Instructor Roles Actively teaches a representation of the OEC course within the 3 year period. * Attends Region recertification clinic at least once every three years. * Is evaluated by an OEC IT at least once in 3 years* Completes all OEC annual refresher requirements.
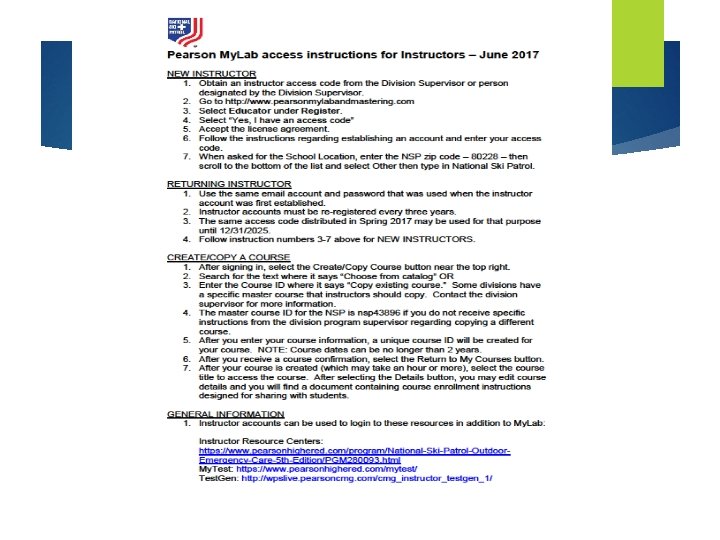
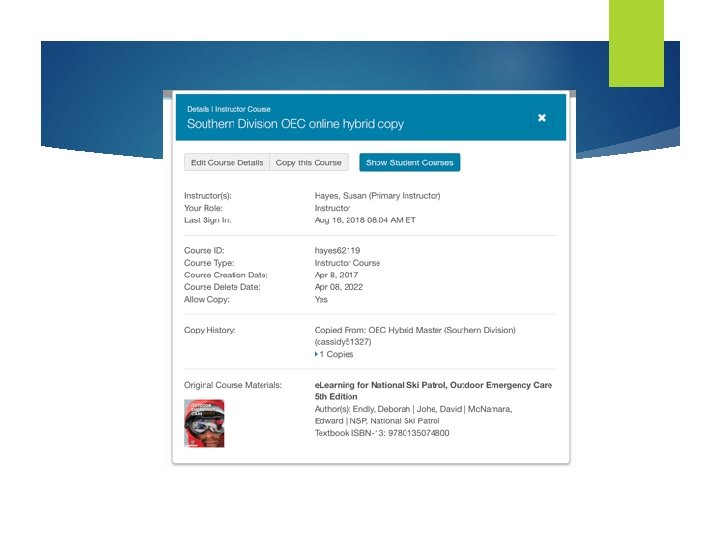
OEC Online Course Tools
IOR Instructor Pearson Code: Pearson’s Access Code HEAIRC-PUREE-AGENE-JAWAN-CRUSH-TAXES
Option 2
The ADA and NSP Training ADA (Americans Disability Act) Sight, Limb, Paralysis, Hearing. ADA works along side the NSP Training in the aid and assistance of any person that may need assistance while at our locations
Conclusion… P Review components of Instructor Development and Adult Learning P Describe the layout of the current OEC curriculum and resources available for teaching P Review “The Backboard Redefined" P Identify the role expectations of OEC instructors