CEMENTUM CONTENTS INTRODUCTION DEFINITION PHYSICAL CHARACTERISTICS COMPOSITION CLASSIFICATION













 – Collagenous cementum derived protein • It will")








 and intrinsic fibers")










 This")


























 of")


- Slides: 64
CEMENTUM
CONTENTS • • • INTRODUCTION DEFINITION PHYSICAL CHARACTERISTICS COMPOSITION CLASSIFICATION CEMENTOGENESIS STRUCTURE OF CEMENTUM CEMENTOENAMEL JUNCTION CEMENTODENTINAL JUNCTION CEMENTUM ASSOCIATED CELLS FUNCTIONS
• • • AGE CHANGES IN CEMENTUM CLINICAL SIGNIFICANCE PATHOLOGICAL CHANGES IN CEMENTUM REGENERATION OF CEMENTUM CONCLUSION
INTRODUCTION • Cementum is considered as a part of periodontium, the attachment apparatus of the tooth, because it provide a medium for insertion of periodontal ligament fibers.
DEFINITION • “Cementum is the calcified , avascular mesenchymal tissue that forms the outer covering of the anatomic root”. • It is a highly specialized form of calcified Connective Tissue, which in part resembles bone structurally but differs from bone in several important functional aspect.
PHYSICAL CHARACTERISTICS 1. Hardness: the hardness of fully mineralized cementum is less than that of dentin. 2. Color : is pale yellow in color and can be distinguished from enamel by its lack of luster and its darker hue. Cementum is somewhat lighter in color than dentin.
3. Permeability : • Very young animals both acellular and acellular cementum are very permeable and permits the diffusion of dyes from the pulp and external root surface. • In cellular cementum, the canaliculi in some areas are contiguous with the dentinal tubules. • The permeability of the cementum diminishes with the age.
4. Thickness • Cementum deposition is a continuous process that proceeds at various rates throughout life • Cementum formation is more rapid in the apical region • Thickness of cementum on the coronal half of the root varies from 16 -60 µm • It attains its greatest thickness in the apical third and in the furcation area(up to 150 -200µm) • It is thicker in distal surfaces than in mesial surfaces, probably because of functional stimulation from mesial drift over time.
COMPOSITION • On a dry weight basis, cementum from fully formed permanent teeth contain about, -Organic substance: 50 -55% - Inorganic substance: 45 -50% Inorganic substance Hydroxyapatite crystals(45 -50%)- which is less than that of enamel(97%), dentin(70%), or bone(65%).
Organic matrix is chiefly composed - 90% type 1 collagen - 5%type III collagen and - Traces of type V, type XII, type XIV collagen • The main source of collagen fibres in cementum are 1. extrinsic fibres(Sharpeys fibres)produced by fibroblasts 2. intrinsic fibres –produced by cementoblasts
• Sharpeys fibres which constitute a considerable portion of the bulk of the cementum • Type III collagen appears to coat the type I collagen of sharpeys fibres • Trace amounts of other collagens, including the type V and type XIV, also are found in extracts of mature cementum.
• Non- collagenous proteins Tenacin , fibronectin , osteocalcin and osteonectin, alkaline phosphatase, proteoglycans, proteolipids, and several growth factors • Enamel proteins • Adhesion molecules - Bone sialoprotein, osteopontin • Glycosaminoglycans - chondroitinsulphate, dermatan sulphate and heparan sulphate. .
Cementum related proteins • They promote cell attachment and cell migration. • Stimulate protein synthesis of gingival fibroblasts and periodontal ligament cells. • Adhesion proteins – Bone Sialoprotein Osteopontin Osteonectin • Bone sialoprotein and osteopontin express during early tooth root development, play a major role in differentiation of cementoblast progenitor cells to the cememtoblast
• Cementum attachment protein (CAP) – Collagenous cementum derived protein • It will promote the adhesion and spreading of mesenchymal cell type, with osteoblast and periodontal ligament fibroblast. • Cementum derived growth factor (CGF) – is an insulin like, growth factor 1 -like molecule. • They enhance proliferation of gingival fibroblasts and periodontal ligament cells.
CLASSIFICATION 1. On the basis of its location Radicular cementum: it is the cementum that covers the root. In humans it accounts for the bulk of the cementum. Coronal cementum: it is the cementum that found on the enamel. In human teeth it is thin and poorly developed.
2. On The Basis Of Presence Or Absence Of Fibrils: • Fibrillar cementum: It is the most common form that contains well defined densely packed collagen fibrils. • Afibrillar cementum: Lacks the collagen fibrils and is in contact with the enamel surface.
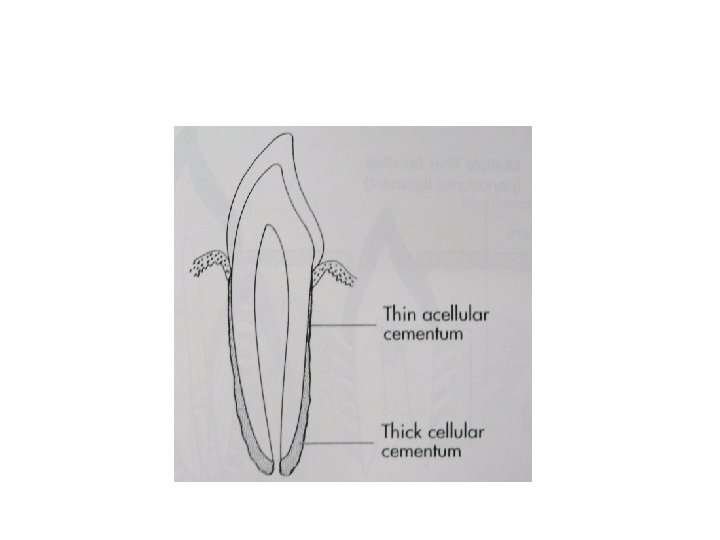
3. On the basis of cellularity: Acellular cementum: • It is the first formed cementum and covers the cervical two third or half of the root. • Does not contain cells • It forms before the tooth reaches the occlusal plane. • Its thickness range from 30 -230 μm.
• Sharpey’s fibers make the most of the structure of acellular cementum • Sharpey’s fibers are completely calcified • Peripheral portion of the Sharpey's fibers are more calcified than interior region • Acellular cementum also contain intrinsic collagen fibers that are calcified and irregularly arranged or lies parallel to the surface
Cellular Cementum: Formed after the tooth reaches the occlusal plane. • Is more irregular • Contain cementocytes • Cellular cementum is less calcified than the acellular cementum. • Cellular cementum is thicker than acellular cementum
• Sharpey’s fibers occupy a smaller portion of cellular cementum and are separated by the other fibers that are arranged either parallel to the root surface or at random. • Sharpey’s fibers may be completely or partially calcified or central uncalcified core surrounded by calcified border • Both cellular and acellular cementum are arranged in lamellae separated by incremental lines parallel to long axis of the root.
Classification of cementum by Schroeder and Page in 1990: 1. Acellular afibrillar cementum: Contains neither cells nor extrinsic or intrinsic collagen fibers, apart from mineralized ground substance. It is a product of cementoblasts and in humans is found in coronal cementum, with a thickness of 1 -15μm.
2. Acellular extrinsic fiber cementum • Composed of almost entirely of densely packed bundles of Sharpey's fibers and lacks cells. It is a product of fibroblasts and cementoblasts. • In humans it is found in the cervical third of the root but may extend further apically. • Its thickness is between 30 and 230μm.
3. Cellular mixed stratified cementum: • Composed of both extrinsic (sharpey’s) and intrinsic fibers and contain cells. It is a co-product of fibroblasts and cementoblasts. • In humans it appears primarily in the apical third of the roots and apices and in furcation areas. • Its thickness ranges from 100 -1000μm
4. Cellular intrinsic fiber cementum: • Contains cells but no extrinsic collagen fibers. • It is formed by cementoblasts. • In humans it is found in the apical third of the root portion (it fills resorption lacunae). • Cellular intrinsic fiber cementum participates in the repair process of previously resorbed roots.
5. Intermediate cementum: • An ill-defined zone near the cementoenamel junction of certain teeth that appears to contain cellular remnants of Hertwig’s sheath embedded in calcified ground substances. • The significance of this layer is that, it contains enamel like proteins, which helps in attachment of cementum to dentin
CEMENTUM ASSOCIATED CELLS Cementoblasts: • Soon after the Hertwig’s epithelial root sheath break up, undifferentiated mesenchymal cells from adjacent connective tissue differentiate into cementoblasts. • Cementoblasts synthesize collagen and protein polysaccharides (proteoglycans) make up the organic matrix of cementum. These cells have numerous mitochondria, a well formed Golgi- apparatus and large amounts of granular endoplasmic reticulum.
Cementocytes: • Are similar to osteocytes. They lie in spaces designated as lacunae. A typical cementocyte has numerous cell processes or canaliculi radiating from its cell body. These processes may branch and they frequently anastomose with those of a neighboring cell. Most of the processes are directed towards the periodontal ligament surface of the cementum.
Cementoclasts • These are multinucleated giant cells which are indistinguishable from osteoclasts. • They are responsible for extensive root resorption that leads to primary tooth exfoliation and for localized cemental resorption in adult dentition.
Developmental and acquired anomalies associated with cementogenisis • Enamel Projections; these are seen particularly in furcation areas , predominantly in mandibular molar area • It is due to the continued activity of amelogens, even after the formation of root start. • So enamel may continue to form over portions of root which are normally covered by cementum, from odontogenic epithelium destined to form HERS • They may predispose teeth to periodontal defects involving furcations
• Enamel Pearls • These are globules of enamel on cervical portion of root • They resemble small pearl • They are formed due to localised failure of HERS to separate from dentin surface which is followed by cementogenesis • This adherent epithelium becomes amelogenetic & deposit globules of enamel, which in turn may become covered with a layer of afibrillar Cementum.
Clinical significance • • They are plaque retentive structures They promote periodontal disease They look similar to calculus, but cannot be scaled off Only grinding will help in elimination
. CEMENTO-ENAMEL JUNCTION • Each tooth has a crown and root portion. The crown is covered with enamel and the root portion is covered with cementum. • The junction between the cementum and enamel at the cervical region of the tooth is termed Cemento-Enamel junction • The relationship between the cementum and enamel at cervical part of the tooth can be of three types
Types of Cemento Enamel Junction: Three types of relationships involving the cementum may exist at the cemento-enamel junction Cementum overlaps the enamel (60% – 65%. ) • This occurs when the enamel epithelium degenerates at its cervical termination, permitting connective tissue to come in direct contact with the enamel surface. • Edge-to-edge butt joints exist (30%. ) Butt joint where enamel and cementum meet at a sharp line
• The cementum and enamel fail to meet (5 %– 10%. ) This occurs due to delayed degenaration of HERS preventing the contact between dental follicle cell &newly formed dentin , in such cases there is no cementoenamel junction • The exposure of the root dentin at the cervical margin can lead to sensitivity at this site, and such morphology may result in increased risk for idiopathic osteoclast-mediated root resorption and root surface caries
CEMENTO-DENTINAL JUNCTION • This is a junction between dentin and cementum • CDJ is relatively stright in permanent tooth and scalloped in deciduous teeth . • This attachment is quite firm although the nature of this attachment is not fully understood. • CDJ is an approximately 1 -3 micrometer.
• In decalcified preparation, cementum is more electron dense than dentin and some of its fibers are arranged in relatively distinct bundles while those of dentin are arranged somewhat haphazardly. • collagen fibrils of cementum and dentin intertwine at their interface in a very complex fashion.
• Sometime dentin is separated from cementum by a zone known as INTERMEDIATE CEMENTUM LAYER, which does not exhibit characteristics features of either dentin or cementum. • This layer is predominantly seen in apical two thirds of roots of molars and premolars and is rarely observed in incisors or deciduous teeth. • It is believed that this layer represents areas where cells of Hertwig’s epithelial root sheath have become trapped in a rapidly deposited dentin or cementum matrix.
FUNCTIONS OF CEMENTUM 1. Attachment: Primary function of cementum is to provide anchorage the tooth in its alveolus. This is achieved through the collagen fiber bundles of the periodontal ligament, whose ends are embedded in cementum. 2. Functional Adaptation: Cementum also plays an important role in maintaining occlusal relationships, whenever the incisal and occlusal surfaces are abraded due to attrition, the tooth supra erupts in order to compensate for the loss and deposition of new cementum occurs at the apical root area.
3. Repair: Cementum serves as the major reparative tissue for root surfaces. Damages to roots such as fractures and resorption can be repaired by the deposition of new cementum. 4. Cementum protects the dentin by forming a continuous layer covering it. 5. Cementogenesis assist in maintenance of width of periodontal ligament 6. Probably helping in eruption process by deposition in apical region
Age changes in cementum 1. Thickness Of Cementum: Cemental deposition is a continuous process that occurs throughout life • Cementum is deposited intermittently and its deposition in later life is mainly in response to stresses to which tooth is subjected • There is triple increase in cementum between 11 and 76 years of age • Average thickness of 95µm at the age of 20 and 215µm at age 60 have been reported
• Relative thick layer of cementum are formed on the roots of unerupted teeth in aged persons 2. Surface Irregularities: • smooth surface becomes irregular due to calcification of periodontal ligament fibre bundles where they are attached to cementum • Local injuries and mechanical stress causes resorptive changes which may be also responsible for surface irregularity
3. Reduced permeability • It became less permeable to dye molecules and ions. • As the permeability reduce the nutritive molecules may not reach the deeper layers of cementum , thus these deeper layers have less cementocytes in them 4. The fluoride content • It may increase with age particularly in the acellular cementum of cervical region, probably because this tends to be exposed to the oral environment
5. Structural changes • Resorption of root may occur with aging which will be repaired by cementum • Cementum also may show alternate periods of resorption and depostion creating reversal lines
CLINICAL SIGNIFICANCE Cementum resorption and repair: • • Permanent teeth do not undergo physiological resorption as do primary teeth. However, the cementum of erupted as well as unerupted teeth is subject to resorptive changes that may be microscopic proportion or sufficiently extensive to present a radiographically detectable alteration in the root contour. Microscopic cementum resorption is extremely common. • Cementum is more resistant to resorption than bone.
• For this reason that orthodontic tooth movement is made possible. • When a tooth is moved by means of an orthodontic appliance , bone is resorbed on the side of the pressure, and new bone is formed on the side of the tension. • Resorption of bone as well as cementum may be anticipated.
• However, in careful orthodontic treatment, cementum resorption is minimal or absent. • But bone resorption leads to tooth migration. • The differences in the resistance of bone and cementum to pressure may be caused by the fact that bone is richly vascularized, where as cementum is avascularized.
Systemic conditions responsible for cemental resorption are : - Calcium deficiency - Paget’s disease - Hypothyroidism - Hereditary fibrous osteodystrophy.
HYPERCEMENTOSIS • Term hypercementosis or cementum hyperplasia refers to a abnormal thickening of cementum. • It is largely an age related phenomenon • It can be localized to one tooth or affect the entire dentition(generalised)
• Because of considerable physiologic variation in the thickness of cementum among different teeth in the same person and also among different person, distinguishing between hypercementosis and thickening of cementum is sometimes difficult.
• If the overgrowth improves the functional qualities of the cementum, it is termed as cementum hypertrophy. • If the overgrowth occurs in nonfunctional teeth or if it is not correlated with increased function, it is termed hyperplasia.
• Occurs as a generalised thickening of cementum , with nodular enlargement of the apical third of the root • It also appears in the form of spike like excrescenses (cemental spikes) created by either the coalescence of cementicles that adhere to the root or the calcification of the periodontal fibres at the site of insertion into the cementum
• The etiology of hypercementosis is not completely understood • The spike like hypercementosis generally results from excessive tension from orthodontic appliances or occlusal forces • Generalised type occurs in -teeth without antagonists -low grade periapical irritation -Pagets disease -acromegaly
• • • Arthritis Calcinosis Rheumatic fever Thyroid goiter Hypercementosis itself does not need treatment It could pose a problem if an affected tooth requires extraction • In multirooted tooth, sectioning of tooth may be required before extraction
Ankylosis • Fusion of the cementum and alveolar bone with obliteration of the periodontal ligament is termed as ankylosis. • Ankylosis occurs in teeth with: - cemental resorption, which suggests that it may represent a form of abnormal repair - after chronic periapical inflammation - tooth replantation - occlusal trauma - embedded teeth
• Ankylosis results in resorption of the root and its gradual replacement by bone tissue. • For this reason, re-implanted teeth that ankylose will lose there roots after a period of 4 -5 years and exfoliate. • When titanium implants are placed in the jaw, healing results in bone that is formed in direct apposition on to the implant without any intervening connective tissue. This may be interpreted as a form of ankylosis.
• Clinically ankylosed teeth lack physiological mobility of normal teeth which is one diagnostic sign for ankylotic resorption. • These teeth usually have a metallic percussion sound. • Teeth will be in infra occlusion. • As the periodontal ligament is replaced with bone in ankylosis, proprioception is lost because pressure receptors in periodontal ligament are deleted or not function correctly
• Radiographically resorption lacunae are filled with bone and Periodontal ligament space is missing • Because no definitive causes can be found in ankylotic root resorption, no predictable treatment can be suggested • Treatment modalities ranges from a conservative approach, such as resotorative intervention to surgical extraction of affected tooth.
HYPOPHOSPHATASIA • Hypophosphatasia is due to an inborn error of metabolism. • The basic disorder is a deficiency of enzyme alkaline phosphatase in serum or tissues • This is characterised by loosening and premature exfoliation of deciduous teeth, mainly anteriors. • Exfoliated teeth show microscopically complete absence of cementum or isolated areas of abnormally found cementum.
Exposure Of Cementum Into Oral Environment • Cementum becomes exposed to the oral environment in the case of gingival recession and as a result of loss of attachment in pocket formation • Cementum is sufficiently permeable to penetrate organic substance, inorganic ions, and bacteria • The surface of the pathologically exposed cementum become hypermineralised because of incorporation of calcium, phosphorous and fluoride from the oral environment • Exposure will cause cementum caries
CEMENTICLES • Cementicles are globular masses(generally less than 0. 5 mm in diameter) of cementum, which forms with in periodontal ligament • They generally exhibit concentric appositional layer of afibrillar and/or fibrillar cementum • They may lie free in the periodontal ligament as free cementicles or become fused to the radicular cemental surfaces as sessile or attached cementicles. • Eventually attached cementicles may become totally incorporated in cementum as interstitial cementicles.
• Cementicles originated from foci of degenerating cells or epithelial cell rests in the periodontal ligament or alveolar bone traumatically displaced into periodontal ligament. • Generally cementicles are not of clinical significance unless they become exposed to the oral environment where they may act as sites for plaque retention.