Cellulitis and Soft Tissue Infections Pamela Orr Professor















 / MSSA/")








- Slides: 26
Cellulitis and Soft Tissue Infections Pamela Orr Professor, Internal Medicine, Medical Microbiology and Community Health Sciences
Investigation n n n Blood cultures if fever history/objective fever/chills/systemic symptoms or signs/immunosuppressed Check for Tinea pedis if lower extremity involved Culture any open wounds (including anaerobic culture if deep or necrotic or malodorous) CBC, urea, creatinine, glucose Image – eg. CT of orbit and brain Incise and drain and pack !!
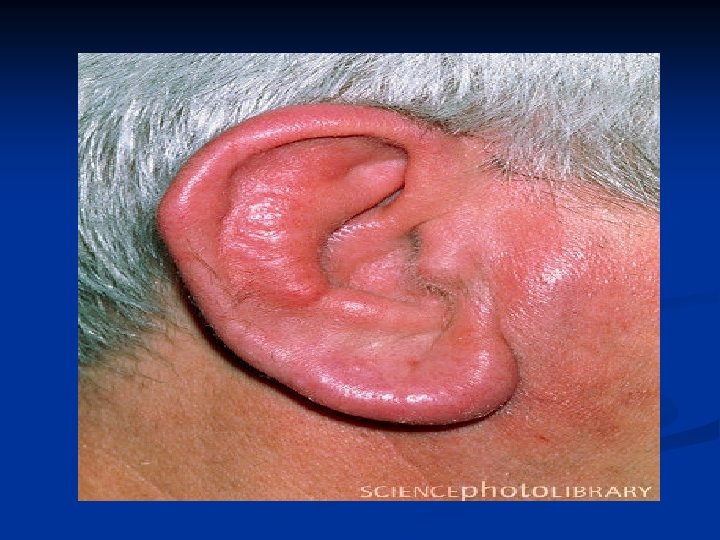
Treatment n Cellulitis not associated with wound – usually Streptococcus A (B/C/G) / MSSA/ MRSA (or Strep Pneumoniae or Haemophilus influenzae in orbital cellulitis) n n n iv Ceftriaxone 2 gm/day +/- iv Vancomycin Pen allergy: iv Clindamycin or Vancomycin Oral: Cloxacillin or Cephalexin (or Clinda if Pen allergic) add Septra or Doxycycline if MRSA is suspected Cefuroxime-axetil in orbital cellulitis Eryripelas – Strep A n n n iv Ceftriaxone (or Pen or Ampicillin) Pen Allergy: iv Clindamycin (or Vanco) Oral: Penicillin V or Amoxil (or Clinda if Pen allergic)
Treatment Diabetic Foot Infection – usually mixed gram +/- /anaerobes. Decide whether osteomyelitis is present, and assess arterial pulses. Often needs iv therapy. Start with (after cultures): n eg. iv Ceftriaxone +iv Vanco+ po Metronidazole n eg. po Amoxicillin/Clavulinic Acid +/- Doxy, or po Septra + Metro Wound Infection – likley mixed infection, as above. Same approach. If Water exposure think of Pseudomonas – use Ceftazidime or Ciprofloxacin instead of Ceftriaxone Head and Neck Region Infections: Be very cautious