Cell injury Cell death and Adaptations Manar Hajeer











 plasma membrane alterations (blebbing, blunting) � (2) mitochondrial")


 � Profound disturbances in membrane function � Profound mitochondrial")




 � CNS infarcts � Center liquefies and digested")





- Slides: 32
Cell injury, Cell death and Adaptations Manar Hajeer, MD, FRCPath.
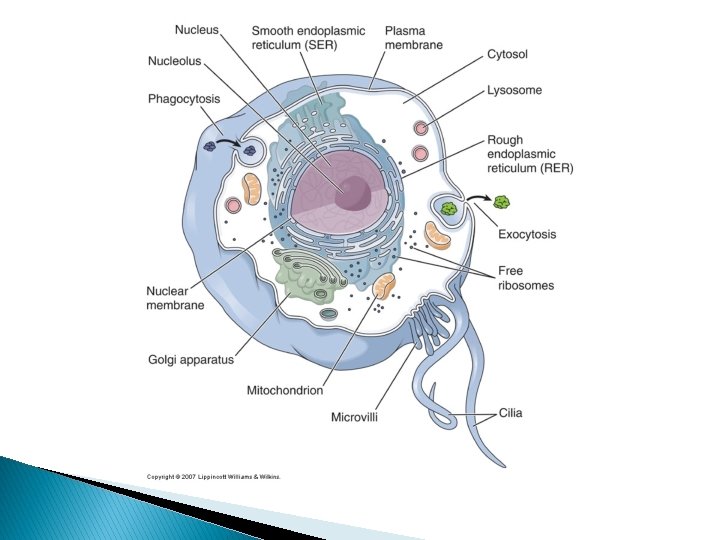
Cells Tissues Organs Systems Organism
Adaptations
Adaptations Forms: Ø Increase in cell size. Ø Increase in number of cells. Ø Change into another type of cell Ø � Adaptation to stress can progress to cell injury if the stress is not relieved.
Hypertrophy • • • Increased size & functional capacity Pure or mixed Increased structural proteins. Pathologic vs physiologic Due to • hormonal stimulation • increased functional demand
Pathologic
Physiologic
Hyperplasia • • • Increase in number of cells Tissues that have proliferative ability Pure vs Mixed Physiologic vs Pathologic vs cancer Due to • hormonal stimulation • Compensatory • increased functional demand • Injury • Infections
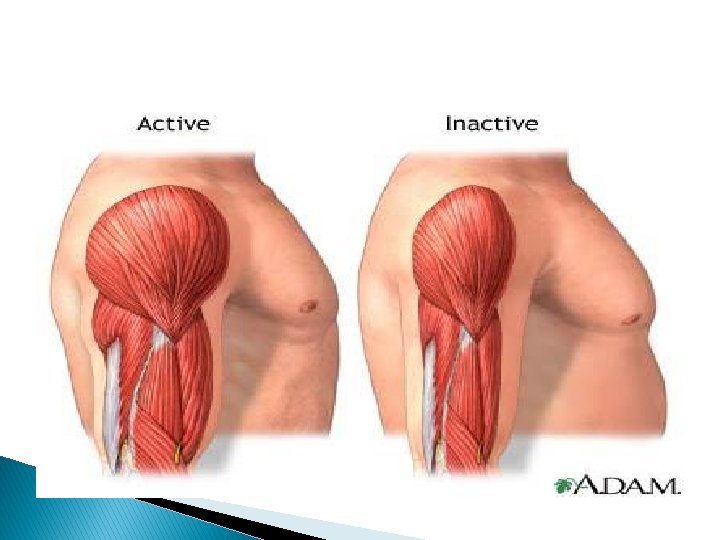
Atrophy Ø Ø Decreased size & function Mechanism: ↓ Protein synth ↑ Degradation ↑ Autophagy Atrophic cells can still function Due to • decreased demand • Ischemia • Disuse • Aging • lack of nerve or hormonal stimulation • chronic inflammation
Metaplasia Ø Ø Ø One cell type to another Altered stem cell differentiation Persistent change increases risk of cancer New cell type copes better with stress but function less. Reversible
Cell injury and death
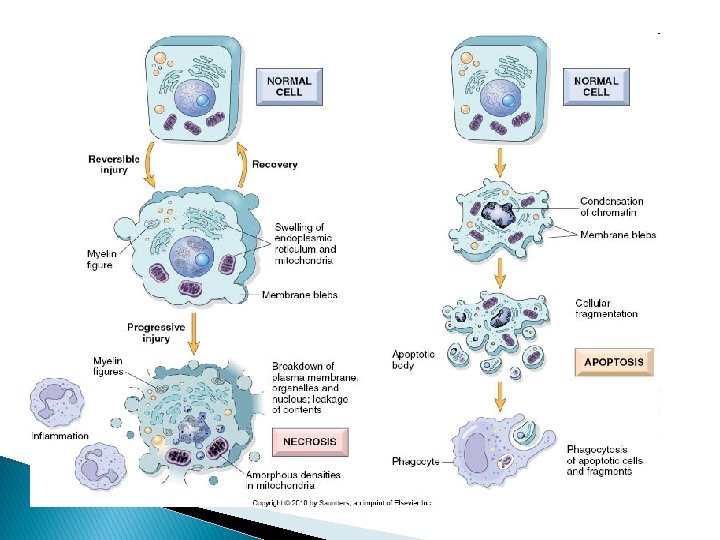
Hallmarks of reversible injury � (1) plasma membrane alterations (blebbing, blunting) � (2) mitochondrial change (swelling and densities); � (3) dilation of ER � (4) nuclear clumping of chromatin. � (5) Cytoplasmic myelin figures
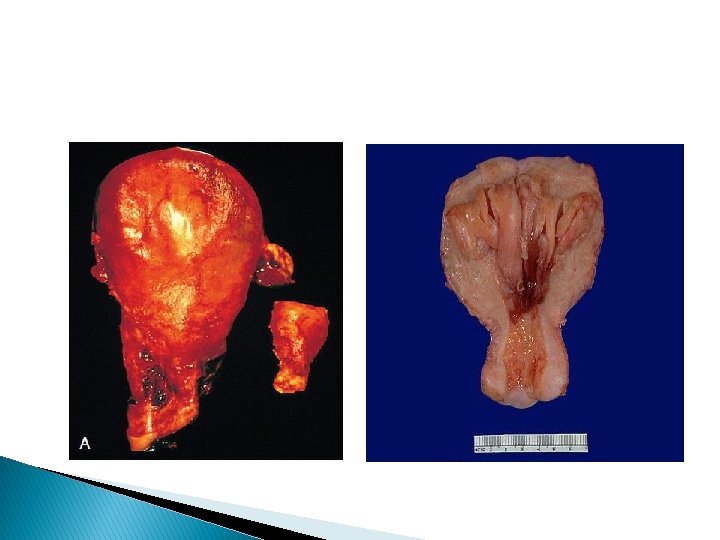
Reversible damage – cellular swelling
Reversible damage – fatty change .
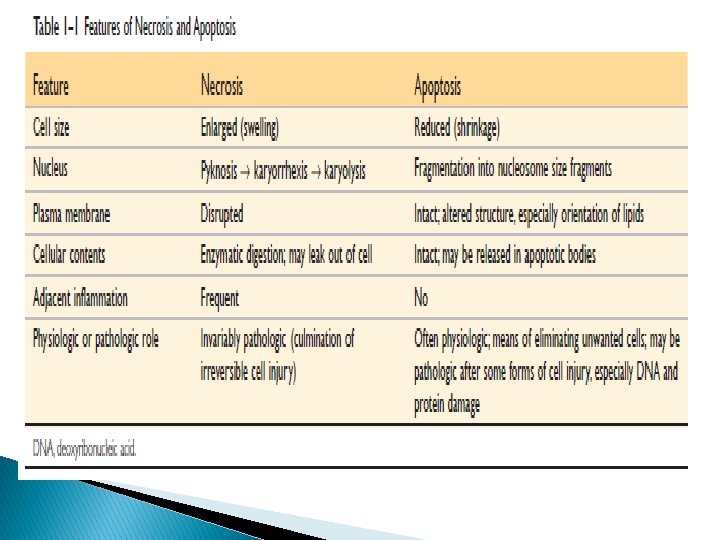
Hallmarks of irreversible injury (Necrosis) � Profound disturbances in membrane function � Profound mitochondrial injury � Increased cytoplasmic eosinophilia. � Marked dilatation of ER , mitochondria. � Mitochondrial densities. � More myelin figures. � Nuclear changes(karyolysis, pyknosis, karyorrhexis)
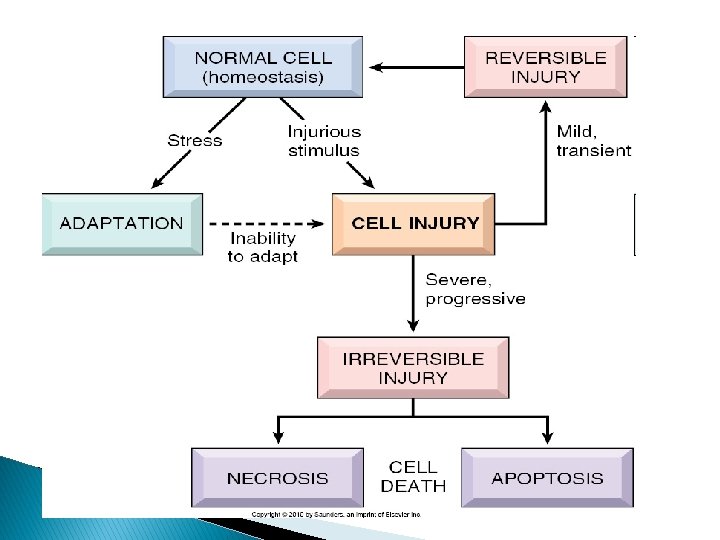
Normal, reversible and irreversible cell injury
Clinical implications � Leakage of intracellular proteins through the damaged cell membrane and ultimately into the circulation provides a means of detecting tissue-specific necrosis using blood or serum samples. � Cardiac enzymes, liver enzymes.
Patterns of tissue necrosis
Coagulative necrosis � � � Conserved tissue architecture initially Anuclear eosinophilic on LM Wedge shaped following blood supply usually Leukocyte lysosomes and phagocytosis required for clearance Characteristic of all solid organ infarcts except the brain
Liquefactive necrosis � Focal infections (pus) � CNS infarcts � Center liquefies and digested tissue is removed by phagocytosis
Gangrenous necrosis � Clinical term � It is coagulative necrosis � Dry vs wet
Caseous necrosis � � � “Cheese like” Combination of coagulative and liquefactive necrosis Tissue architecture is not preserved Acellular center Usually enclosed in an granulomatous inflammatory border Most often seen in TB
Fat necrosis Occurs in acute pancreatitis � Due to release of pancreatic lipases � Focal fat destruction � Released FA’s combine with Ca 2+ (saponification) to produce the whitish chalky appearance �
Fibrinoid necrosis � Visible by LM � Deposits of antigen – antibody and fibrin complexes in arterial walls � Seen in vasculitis
Apoptosis � Programmed cell death � Lack of inflammation