CDC Guideline for Prescribing Opioids for Chronic Pain

CDC Guideline for Prescribing Opioids for Chronic Pain. United States-2016 Gisele J. Girault, M. D. First Choice Healthcare Columbia, SC

Scope and Audience of the Guidelines • Targeted for primary care physicians • PCPs account for almost 50% of all dispensed opioid prescriptions • Growth in PCP prescribing has been above average • PCPs report concern over their insufficient training in opioid prescribing

Other Opioid guidelines • • • SC Medical Board Federation of State Medical Boards American Pain Society American Dental Association American Academy of Family Physicians

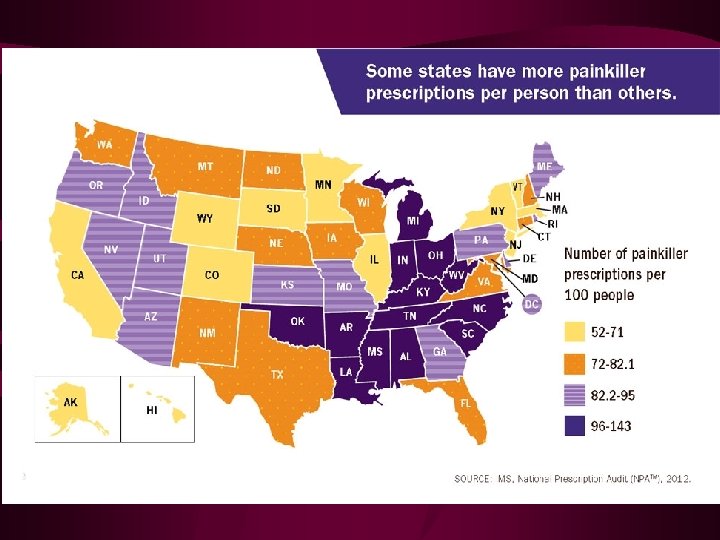
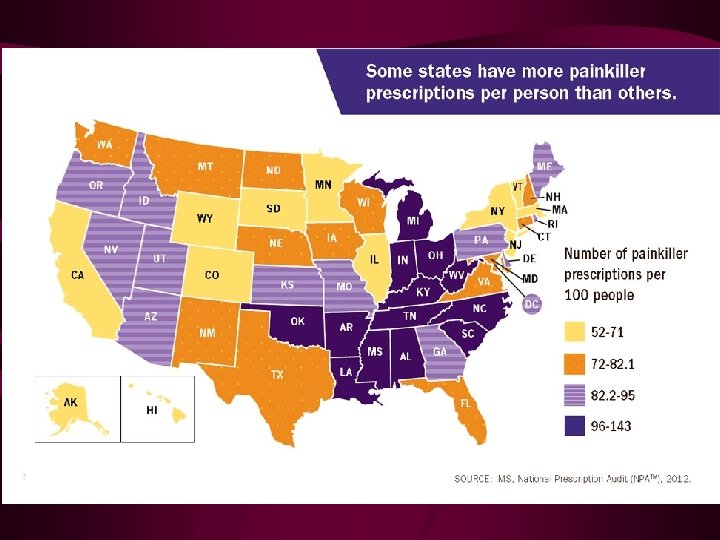
Rationale behind the CDC Guidelines? • • In 2012, >259 million scripts written 2007 -2012 prescribing increased by 7. 3% Prescribing varies greatly across states Significant increase in opioid prescribing in pediatric ages 12 -17 years • PCPs have concerns about abuse and addiction • Lack of consensus on how to use opioids

Goals of the CDC Recommendations • To improve communication between providers and patients • To improve effectiveness of pain treatment • To reduce the risks of long term opioid therapy including opioid use disorder and overdose

Specific Recommendations • Determining when to initiate or continue opioids for chronic pain • Opioid selection, duration, follow up, and discontinuation • Assessing risk and addressing harms of opioid use.

Determining When to initiate or Continue opioids for chronic pain • Opioids are not a first line or routine therapy for chronic pain • Establish and measure goals for pain and function • Discuss the risks and benefits of non-opioid therapies with patients

Pain Management Therapies • Pharmacological Therapies • Psychological Therapies • Physical Therapies • Procedural Therapies

Opioid selection, dosage, duration, follow-up, and discontinuation • • • Use short acting opioids when starting Start low and go slow In acute pain prescribe no more than needed Do not prescribe ER/LA opioids in acute pain Follow up and re evaluate risk of harm; reduce or taper and discontinuation if needed

LA/ER opioids vs. Short acting ***Abuse Deterrent formulations • Ultram ER • MS Contin, Kadian, **Embedda • **Oxycontin • **Nucynta ER • **Opana ER • **Exalgo • Ultram • MSIR • • Oxy. IR, Percocet Nucynta Opana Dilaudid/Hydromorph one

Assessing Risk and addressing Harms of Opioid Use • Evaluate risk factors for opioid related harms • Check PDMP for scripts from other sources • Using UDS to identify all substances • Avoid using benzos and opioids concurrently • Arrange treatment for Opioid Use Disorder (OUD) if needed
 •")
Risk Assessment Tool • Screener and Opioid Assessment for Patients in Pain-Revised, (SOAPP-R) • Current Opioid Misuse Measure, (COMM) • Opioid Risk Tool, (ORT) • Stratify patients on opioids or considering opioids into low, medium and high risk based on predicting risks of aberrant behaviors

Urine Drug Screens • Use risk stratification tool to put patients in high, medium or low risk • Test frequency based on risk category • Examples – High risk test q 1 -3 months – Medium risk test every 3 -6 months – Low risk test every 6 -12 months • Test more frequently if needed
 DSM-V • A problematic pattern of opioid use leading to")
Opioid Use Disorder, (OUD) DSM-V • A problematic pattern of opioid use leading to clinically significant impairment or distress, as manifested by at least two of the following, (criteria) occurring within a 12 -month period:
 • Methadone-outpatient clinic • Schedule II • Need")
Medication-Assisted Treatment for Opioid Addiction (MAT) • Methadone-outpatient clinic • Schedule II • Need special license to prescribe for opioid addiction • Liquid form, daily dosing from clinics • Buprenorphine/Naloxone • Suboxone, Zubsolv, Probuphine • Schedule III • DATA 2000 license ; limit of 275 patients

Abuse-Deterrent forms of Buprenorphine

Opioids and Co-morbidities • • Sleep disturbances Reduced renal or hepatic function Concurrent use of benzodiazepines Pre existing depression or psychiatric dx Concurrent use of psychotropic drugs Age >65 History of OUD or aberrant substance use

Opioid Dose and Risk factors • ASE increase with increasing doses – <50 morphine mg equivalents (MME) – 50 - 90 MME – > 100 MME • MME is a conversion from one opioid to mg of Morphine • For example 20 mg Oxycodone = 30 MME

Opioid Dose and Risk Factors • 80% of overdoses are in the > 100 MME range • Opioid hyperalgesia increased at higher doses • Higher risks of respiratory depression • >50 MME used as a trigger for prescribing Naloxone

Naloxone

What is the problem? • 2013 est. 1. 9 million people abusing prescription opioid medications • H/o getting a script increases the risk for OUD and overdose • Recent study showed 550 died from overdose at 2. 6 years after initial script • 1 in 32 over 200 MME died of overdose

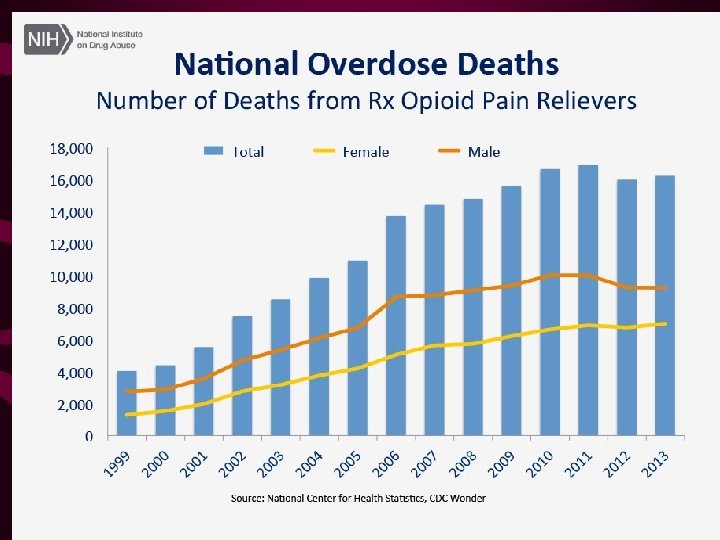
What’s the problem? • Death rates from CAD, and cancer have declined • Opioid associated death rates have increased dramatically • Roughly 20% of physicians prescribe 80% of opioid scripts • Opioid prescribing has increased with opioid sale$ • Each day over 5000 new non-medical users

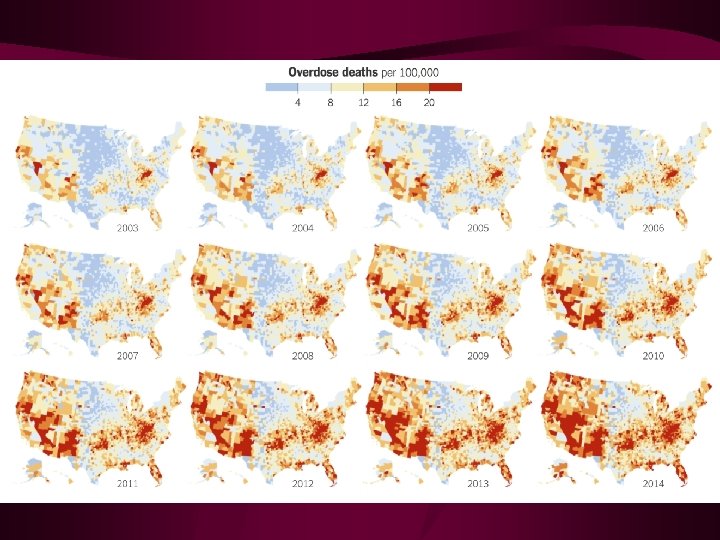
Overdose Statistics

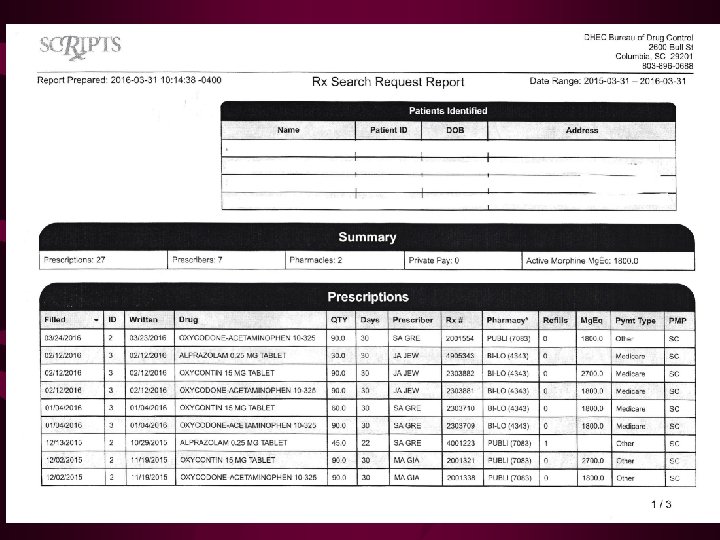
Sources of diverted opioids

How do we turn this around? • Better education for physicians in opioid management • Mandates for physicians to use PDMP • Limit the number/amount/time frame for prescribing opioids? • Limit who can prescribe opioids, DEA? • Pressure on TPP to pay for abuse deterrent drugs

Conclusions • CDC Guidelines are a good start in improving the safety of opioid prescribing • Stricter mandates for physicians who prescribe opioids • Pressure TPP and drug companies to make better opioids financially accessible
- Slides: 31