CBC Interpretation Exploring the basics of the basic

CBC Interpretation Exploring the basics of the basic test DR IDHATE TUSHAR MD Pediatrics LTMGH, Sion Hospital, Mumbai Fellowship in Pediatric Haemato- Oncology Evelina London Children's Hospital, UK Apollo Hospital, Delhi Registrar in Pediatric Oncology Tata Memorial Hospital, Mumbai

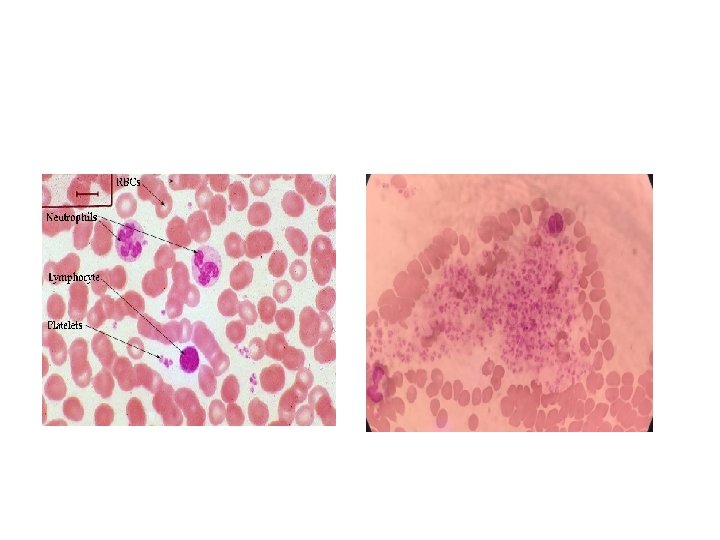
TEST REFERENCE RANGE Hb 9. 5 -13. 5 gm/dl RBC COUNT 3. 2 -4. 8 mill/cu. mm PCV 42 -44% MCV 72 -86 fl MCH 24 -34 pg MCHC 30 -36 % WBC COUNT 4000 -11000/cu. mm DIFFERENTIAL COUNT P/L/M/E/B PLATELET COUNT 150000 -400000 /cu. mm RDW 11. 5 -15% RETIC COUNT 0. 42 -1. 82%
 ----measures variation in red blood cell size")
• RDW (11. 5 -15% ) ----measures variation in red blood cell size • Reticulocyte count (0. 42 -1. 82%) ----window to the bone marrow

TESTS Series 1 CASE-1 Series 1 CASE-2 Series 1 CASE- 3 REFERENCE RANGE Hb 5. 8 5. 5 9. 5 -13. 5 gm/dl RBC COUNT 4. 94 2. 28 3. 31 3. 2 -4. 8 mill/cu. mm PCV 25 14. 7 17. 9 42 -44% MCV 50. 7 68 53. 1 72 -86 fl MCH 11. 8 24 13. 5 24 -34 pg MCHC 23. 39 35 25. 3 30 -36 % WBC COUNT 15910 25587 9500 400011000/cu. mm DIFFERENTIAL COUNT P-42; L-49 P-25; L-70 P-53; L-20 PLATELET COUNT 2, 74, 000 180000 642000 150000 -400000 /cu. mm RDW 20. 4 14. 5 16. 3 11. 5 -15% RETIC COUNT 1. 5 2. 2 1. 5 0. 42 -1. 82%

Clinical details- S 1, Case 1 Two year boy admitted with respiratory infection Examination: • Pallor-present • Liver-2 cm • Spleen – not palpable

S 1, Case 1 TEST OBSERVED VALUE REFERENCE RANGE Hb 5. 8 9. 5 -13. 5 gm/dl RBC COUNT 4. 94 3. 2 -4. 8 mill/cu. mm PCV 25 42 -44% MCV 50. 7 72 -86 fl MCH 11. 8 24 -34 pg MCHC 23. 39 30 -36 % WBC COUNT 15910 4000 -11000/cu. mm DIFFERENTIAL COUNT P-42; L-49 PLATELET COUNT 2, 74, 000 150000 -400000 /cu. mm RDW 20. 4 11. 5 -15% RETIC COUNT 1. 5 0. 42 -1. 82%
")
Differentials… ? Iron Deficiency Anemia ? Thal trait ( less likely )

Peripheral Smear • IDA: -Microcytic Hypochromic -Anisopoikilocytosis • Thal Trait : - Microcytic Hypochromic - Less Anisopoikilocytosis PS not sufficient to differentiate
 • SERUM FERRITIN- 0.")
IRON STUDIES • SERUM IRON- 10 mcg/dl ( 70 -180) • SERUM FERRITIN- 0. 80 ng/ml ( 20 -150) • TIBC- 494 mcg/dl ( 250 -400) Diagnosed as IDA

IDA • Stool exam to rule out occult blood • Elemental Iron 6 meq/kg /day ? OD/BD ? Empty stomach ? Ferrous fumarate/sulphate/ascorbate/gluconate ? Duration ? No response to iron

Series 1, Case 2 TEST OBSERVED VALUE REFERENCE RANGE Hb 5. 5 9. 5 -13. 5 gm/dl RBC COUNT 2. 28 3. 2 -4. 8 mill/cu. mm PCV 14. 7 42 -44% MCV 68 72 -86 fl MCH 24 24 -34 pg MCHC 35 30 -36 % WBC COUNT 25587 4000 -11000/cu. mm DIFFERENTIAL COUNT P-25; L-70 PLATELET COUNT 180000 150000 -400000 /cu. mm RDW 14. 5 11. 5 -15% RETIC COUNT 2 0. 42 -1. 82%

What next? ? Iron studies ? HPLC History…

Clinical Details… 4 ½ months boy presented with increasing pallor Exam: Pallor+ Liver 4 cm Spleen 3 cm No lymphadenopathy

Peripheral smear • • • Microcytic hypochromic Anisopoikilocytois Tear drop cells Polychromasia Nucleated RBCs DIRTY SMEAR : Thal Major

HPLC of baby
 • Hb A")
HPLC of baby • Hb A- 4% ( 94 -98 %) • Hb A 2 - 1. 7 % (1. 5 -3. 7) • Hb F- 94. 3 % ( 0. 0 -2. 0 %) Hb F 1 -30 days 22 -92 % 1 -3 months 7. 6 -89 % 3 -6 months 1. 6 -42. 2 % 6 -9 months 0 -16. 7 % 9 -12 months 0. 0 -10. 5 % 12 -23 months 0 -6. 3 % 24 months 0 -0. 9 %
 93. 3 93. 9 Hb A")
Mother Father Hb A ( 94 -98 %) 93. 3 93. 9 Hb A 2 (1. 5 -3. 7) 5. 9 4. 7 Hb F ( 0. 0 -2. 0 %) <0. 8 1. 4 Thal Trait

DIVISION OF PEDIATRIC HEMATOLOGY/ ONCOLOGY DEPT OF PEDIATRICS , MGM MEDICAL COLLEGE AND MCRI, AURANGABAD Name: _________________________________ Registration No: Gender: M/F D/O/B : DATE OF FOLLOW-UP CLINICAL EXAM AGE HT(cms) WT (kg) Pallor Icterus Pigmentation Liver Spleen SMR/TV Pre-Tx Hb range Mean Pre-Tx Hb last year

INVESTIGATIONS HB TC ENDOCRINE INVG: Serum Ferrition GTT/Hb. Alc MRI DC Platelet count LFT: IRON OVERLOAD S. FSH/S. LH Liver iron overload S. Testosterone/S. Oestriol Cardiac iron overload S. GH DEXA Scan (BMD) Total Protein S. Alb/S. Glob Serum Bilirubin(T) Direct/Indirect S. Cortisol Z-Score Femur Z- Score Spine Ca/p/Alk. Po 4 SGPT/SGOT CHELATION DRUG: RENAL function test Dose BUN/S. Creatinine HIV S. PTH Side-effects if any Audiometry HCV HBs. AG Hepatitis B Vaccine Opthalm Examination OTHER MEDIICATIONS

Series 1, Case 3 9 years boy presented with fatigue and pallor since 2 -3 years Exam: Pallor+ Liver 3 cm Spleen 2 cm

TEST Series 1, Case 3 CASE- 3 REFERENCE RANGE Hb 5. 5 9. 5 -13. 5 gm/dl RBC COUNT 3. 31 3. 2 -4. 8 mill/cu. mm PCV 17. 9 42 -44% MCV 53. 1 72 -86 fl MCH 13. 5 24 -34 pg MCHC 25. 3 30 -36 % WBC COUNT 9500 4000 -11000/cu. mm DIFFERENTIAL COUNT P-53; L-20 PLATELET COUNT 642000 150000 -400000 /cu. mm RDW 16. 3 11. 5 -15% RETIC COUNT 1. 5 0. 42 -1. 82%

Differentials… ? Thalassemia ? IDA ? Any other

Investigations: • HPLC : Normal • Iron studies: Sr Iron , Sr ferritin, transferrin saturation All raised What next?

BMA


• Started on pyridoxine 50 mg/day • Mutational analysis at NIIH, Mumbai to confirm congenital Vs acquired form of sideroblastic anemia

Microcytic Hypochromic Anemias IDA THALASSEMIA Trait ANEMIA OF CHRONIC DISEASE Sideroblastic Anemia RDW Wide Normal Peripheral Smear Microcytosis Hypochromia Anisopoikilocytosis, polychromasia, target cells Hypochromia Micro/ Normocytic Microcytosis Hypochromia Sideroblats (basophilic iron deposits ) Serum Iron Low N / high Sr ferritin Low N / high TIBC High N / high N / Low HPLC Normal Abnormal Normal
 < 13 thal")
Mentzer Index MI= MCV/ RBC count ( and not PCV ) < 13 thal trait >13 IDA

Sitting in busy OPD? Take a look…. LOW MCV RDW NARROW HPLC WIDE IRON STUDIES

TESTS Series 2, CASE-1 Series 2, CASE-2 Series 2, CASE- 3 REFERENCE RANGE Hb 4. 76 2. 7 2. 3 9. 5 -13. 5 gm/dl RBC COUNT 1. 22 1. 2 0. 87 3. 2 -4. 8 mill/cu. mm PCV 19 21 6. 75 42 -44% MCV 97. 8 88 77. 59 72 -86 fl MCH 38. 3 30 25. 29 24 -34 pg MCHC 35 34 32. 59 30 -36 % WBC COUNT 7720 2000 3540 400011000/cu. mm DIFFERENTIAL COUNT P-12; L-86 (ANC: 924 ) P-36; L-61 (ANC-720) P-8; L-89 (ANC 280 ) PLATELET COUNT 80000 10000 55000 150000 -400000 /cu. mm RDW 34. 7 13. 1 21. 9 11. 5 -15% RETIC COUNT 0. 7 0. 5 0. 10 0. 42 -1. 82%

Series 2, Case 1 • 10 months female admitted with increasing pallor • History of developmental delay as well • Exclusively breastfeeding Exam: Pallor + Liver 3 cm spleen 2 cm

Series 2, Case 1 TEST OBSERVED VALUE REFERENCE RANGE Hb 4. 76 9. 5 -13. 5 gm/dl RBC COUNT 1. 22 3. 2 -4. 8 mill/cu. mm PCV 1. 9 42 -44% MCV 97. 8 72 -86 fl MCH 38. 3 24 -34 pg MCHC 35 30 -36 % WBC COUNT 7720 4000 -11000/cu. mm DIFFERENTIAL COUNT P-12; L-86 ( 924 ) PLATELET COUNT 80000 150000 -400000 /cu. mm RDW 34. 7 11. 5 -15% RETIC COUNT 0. 7 0. 42 -1. 82%

What Next… • Vit B 12 and folate levels ? • Bone marrow aspiration and biopsy ?

B 12 protocol 10 mcg s. c for 2 days ( K and reactions monitoring) 1000 mcg i. v / i. m. for 7 days 1000 mcg i. m. weekly for 4 doses 1000 mcg i. m. 3 monthly for 1 year (infants) OR oral B 12 (Ref Nathan Oskis Hematology Of Infancy and childhood )

Do Not Miss In Infants Do CBC Of Mother If affording B 12 levels Tab B 12 500 mcg daily for 6 months at least

Series 2, Case 2 TEST OBSERVED VALUE REFERENCE RANGE Hb 2. 7 9. 5 -13. 5 gm/dl RBC COUNT 1. 2 3. 2 -4. 8 mill/cu. mm PCV 21 42 -44% MCV 88 72 -86 fl MCH 30 24 -34 pg MCHC 34 30 -36 % WBC COUNT 2000 4000 -11000/cu. mm DIFFERENTIAL COUNT P-36; L-61 (ANC-720) PLATELET COUNT 10000 150000 -400000 /cu. mm RDW 13. 1 11. 5 -15% RETIC COUNT 0. 5 0. 42 -1. 82%

Clinical details • 14 years girl admitted with high grade fever since 10 days • No history of bleeding, no previous transfusions • Exam: Febrile , tachypnic Pallor + No H-S megaly/ LN pathy

• Differentials…? • What Next…?



Series 2, Case 3 • 15 years female presented with complaints of generalized weakness, fatigue since 4 -5 days • Did not have fever Exam : Pallor + No bleeding manifestations/ significant lymphadenopathy Liver and spleen not palpable CNS - Normal

Series 2, Case 3 TEST OBSERVED VALUE REFERENCE RANGE Hb 6. 1 9. 5 -13. 5 gm/dl RBC COUNT 2. 19 3. 2 -4. 8 mill/cu. mm PCV 18. 3 42 -44% MCV 83. 56 72 -86 fl MCH 27. 85 24 -34 pg MCHC 33. 33 30 -36 % WBC COUNT 3750 4000 -11000/cu. mm DIFFERENTIAL COUNT P-10 L 80 (ANC 370 ) PLATELET COUNT 14000 150000 -400000 /cu. mm RDW 14. 0 11. 5 -15% RETIC COUNT 0. 10 0. 42 -1. 82%

BM Morpho showing blasts : Acute Leukemia

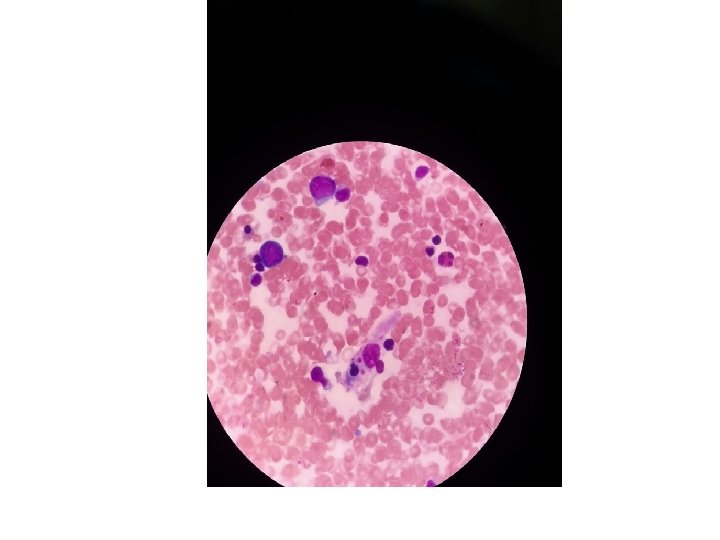
Case 4 : • 2 years girl presented at outside hospital with chief complaints of Fever , abdominal distension & rash over body since 1 month • PER ABDOMEN : Distension ++ Liver : palpable 3 cm Spleen : palpable 4 cm

• Differentials • Investigations
 Peripheral smear normal Dengue/malaria rapid")
CBC : 9. 4 /8170/10000 ( P 20 ) Peripheral smear normal Dengue/malaria rapid test negative Fibrinogen level -147 (Hypofibrinogenaemia ) • Sr Triglycerides- 435 (Hypertiglyceridemia ) • Ferritin >1000 • •
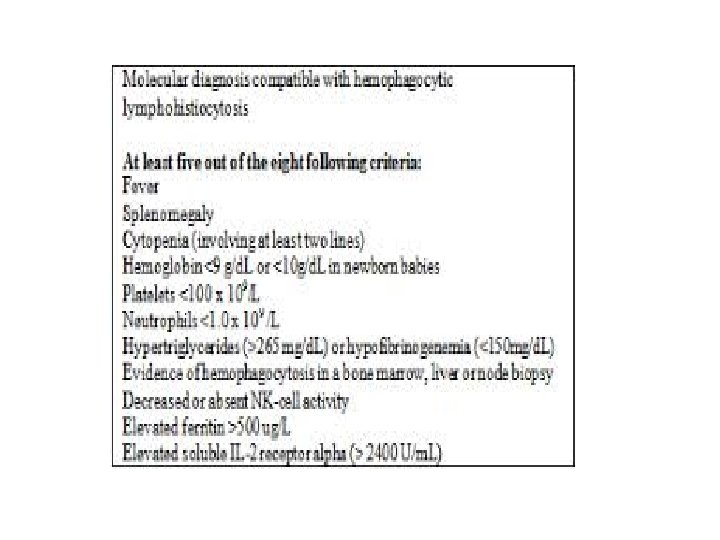
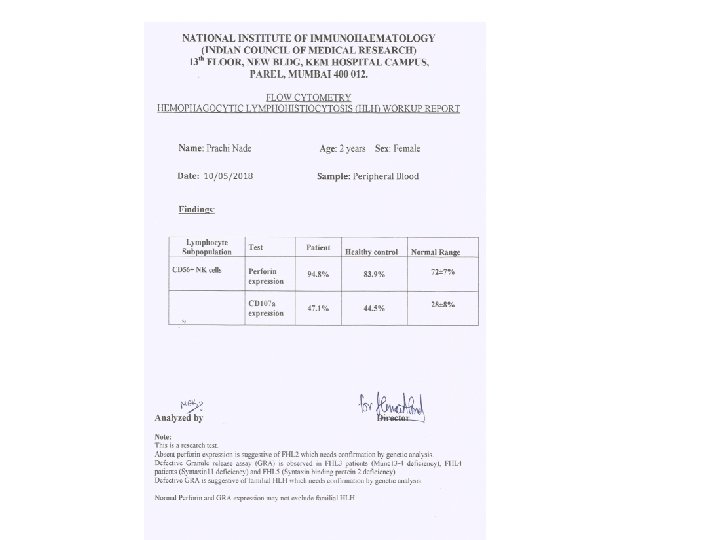

• How common is HLH ? • What is difference between Primary and secondary HLH ? • How will you treat this child ?

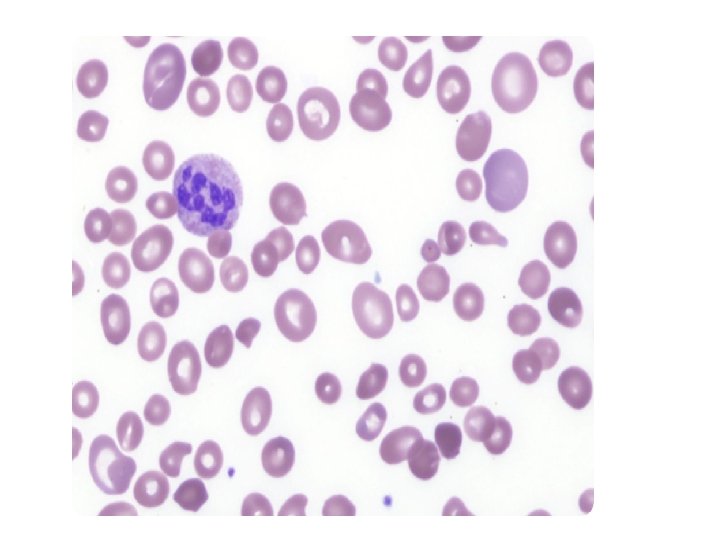
Case 5: • 1 ½ year old boy was referred to our hospital with the complaints of fever, cold and cough since 2 -3 days • CBC and peripheral blood smear showed pancytopenia • Referred for further evaluation

• On general examination, he had silvery hair, hypopigmentation over the skin • Systemic examination Liver 3 cm Spleen 4 cm


• Bone marrow aspirate confirmed ‘giant inclusion bodies’ in cytoplasm of granulocytes which aim towards Chediac Highashi Syndrome

• Skin biopsy showed sparse melanin pigment in keratinocytes in lower half of epidermis and giant melanocytes • Hair shaft microscopy also showed evenly distributed large melanin granules (that were bigger than those seen in normal hair)

• After confirming the diagnosis, the patient and his siblings’ HLA matching has been planned for curative bone marrow transplantation therapy

Pancytopenia • • • Megaloblastic Anemia Acquired Aplastic Anemia Acute leukemia Congenital Marrow failure syndromes HLH PID Peripheral smear some clue Kindly consider BMA and Biopsy

Coming to rainy season … • 16 years old female referred as a suspected case of Dengue fever with thrombocytopenia • Clinically no bleeding manifestations • Serological tests for dengue and malaria : negative

• EDTA blood sample revealed thrombocytopenia. • Peripheral blood smear revealed platelets ADEQUATE and in clumps

EDTA-Peudothrombocytopenia Diagnosis : • Normal platelet count when examining citrated blood • Progressive fall of platelet counts and evident platelet clumping over time in EDTA sample

Take Home Message • Always read CBC Completely ( RBC Count, MCV, MCHC, RDW, ANC, PS) • Microcytic hypochromic anemia: Look RDW • Investigate Iron refractory anemias • Megaloblastic Anemia: Give total doses of B 12 • Pancytopenia : consider BM

• In cases of cytopenias keep possibility of transient marrow suppression due viral infection ( especially in clinically well child ) • EDTA PST is not so rare

Contact: 8554021666
- Slides: 65