CBC How to Interpret and Pursue an Abnormal

CBC 이상소견의 해석 및 추적 How to Interpret and Pursue an Abnormal CBC in Adults 혈액종양내과 방수미

Case 1 • A 40 -year-old man presents with a WBC count of 3× 109/L. The WBC differential reveals an ANC of 1. 2× 109/L. The patient is completely asymptomatic, and his family history, medical history, and medication history are all unremarkable. Review of old medical records shows that the patient usually has a mildly low WBC count.

Question 1 • Which one of the following is the next appropriate step? a. Bone marrow (BM) biopsy b. Hematology consultation c. Periodic monitoring of WBC count with no further investigation at this point d. Long-term use of myeloid growth factors to keep the WBC count normal e. Long-term use of prophylactic antibiotics

Neutropenia

Neutrophil Distribution
 AZA for Crohn’s disease G-CSF")
Case 1 (Var) AZA for Crohn’s disease G-CSF
 2 months later")
TPMT deficiency (Thiopurine Methyltransferase) 2 months later

Leukocytosis • The first step: WBC differential to determine which step is in excess • PBS has additional role • Immaure precursors or blasts (leukemia) versus mature leukocyte types (neutrophilia, lymphocytosis, monocytosis etc)

Case 2 • A 57 -year-old man presents with persistent leukocytosis and lymphocytosis (absolute lymphocyte count, 14. 9× 109/L) for 2 years. The patient is asymptomatic, and has neither hepatosplenomegaly nor lymphadenopathy.

Question 2 • Which one of the following tests is the most useful for the diagnosis? a. Serum LDH level b. Chest and abdominal CT c. PB immunophenotyping d. BM histologic examination e. BM karyotype analysis

Diagnosis Monoclonal B-lymphocytosis • • PB lymphocyte < 5, 000/μL Absence of lymphadenopathy or organomegaly Chronic Lymphocytic Leukemia • • • 1~2%/year • PB lymphocytes ≥ 5, 000/μL Larger, stypical, cleaved cells or promyelocytes PB < 55% Monoclonality should be proven using immunophenotyping (CD 5+, CD 19+, CD 20 dim, CD 23+) BM examination, optional Small Lymphocytic Lymphoma • • PB lymphocyte < 5, 000/μL Lymphadenopathy proven by histopathologic examination

Scoring system for CLL Scores in CLL range from 3 to 5 while in the other B-cell disorders are 0– 2.

Scoring system for CLL Scores in CLL range from 3 to 5 while in the other B-cell disorders are 0– 2.

Case 2 with f/u PLT ALC Hb Heavy drinking HBV reactivation

Case 3 • During evaluation for microcytic anemia in a patient with rheumatoid arthritis, the patient’s serum ferritin level was found to have increased and transferrin saturation was 20%.

Question 3 • Which one of the following statements is true regarding this case? a. IDA is unlikely b. IDA cannot be ruled out c. The patient could have both IDA and ACD d. ACD is unlikely e. Thalassemia can be ruled out

Microcytic Anemia 항목 Iron deficiency Inflammation Thalassemia Sideroblastic anemia Smear Micro/hypo Normal micro/hypo Micro/hypo with targeting Variable Serum iron <30 <50 Normal to high TIBC >360 <300 Normal TS(%) <10 10 -20 30 -80 Ferritin <15 30 -200 50 -300 normal Abnormal with β thalassemia normal Hb pattern on normal eletrophoresis
 • During evaluation for the low hemoglobin of 8 g/d. L")
Case 3 (Var) • During evaluation for the low hemoglobin of 8 g/d. L in a patient with Crohn’s disease with melena, the patient’s serum ferritin level was found to have increased and transferrin saturation was 9%. What is the adequate treatment for anemia?
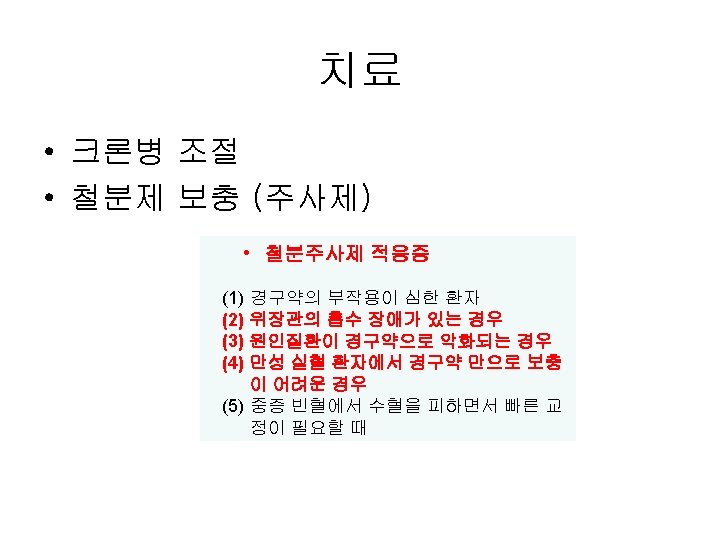
= (15 -Hb)×체중× 2. 3 + 1, 000 (여성은 500) 증례")
치료 용량 용량 (mg)= (15 -Hb)×체중× 2. 3 + 1, 000 (여성은 500) 증례 = (15(M)/14(F)-8) x 체중 x 2. 3 *주의 사항: anaphylaxis (iron dextran제제) Iron carboxymaltose/sucrose/gluconate제제에서는 드뭄 1회 최대 처방용량이 1, 000/500/125 mg로 차이가 있음

Case 4 • During evaluation for military entrance in an 19 -year-old patient, the patient’s hemoglobin was 18. 8 g/d. L. ANC/platelet count were normal. He was not smoker and his past medical history was not remarkable.

Question 4 • Which one of the following tests should be performed at first? a. Serum erythropoietin level b. Arterial O 2 saturation c. JAK 2 V 617 F mutation test d. BM examination e. Abdominal CT

Approach to Polycythemia



Erythromelalgia

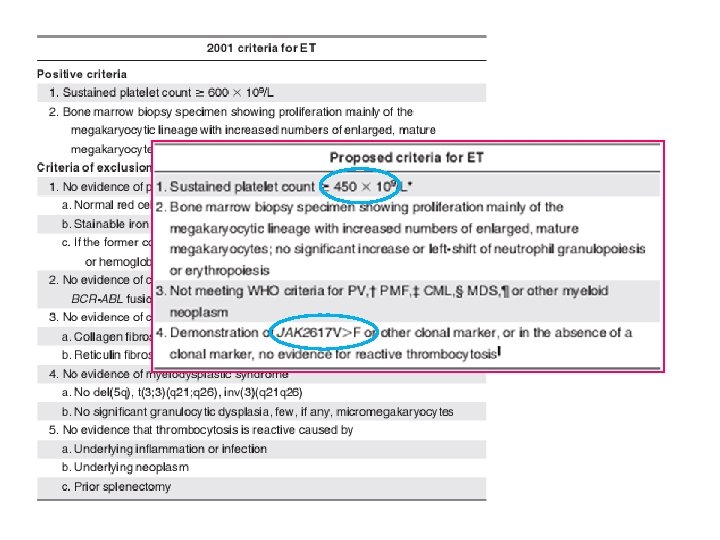
추가 병력 및 검사 • 과거 병력: 6년 전 관절재수술 당시 혈소판이 최고 717 k로 상 승하여 골수검사 등을 시행하고 수술 후 572 k로 감소하여 반 응성 고혈소판증으로 진단 • 신체검진: 간이나 비장 비대는 없음 • CBC: 12, 330 -14. 4 -950 k • LD: 382 (100~225) • BM aspiration and biopsy: normocellular marrow with increased mature megakaryocytes (cellularity 41 -50%) • JAK 2 V 617 F mutation (heterozygote)

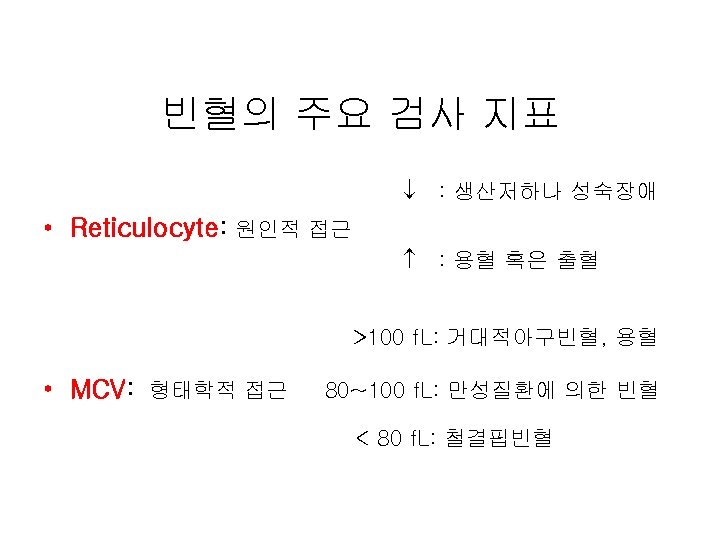
Take Home Messages • • • Leukopenia_감염병력 및 복약력 Leukocytosis_WBC differential counts Anemia_Reticulocyte and MCV Erythrocytosis_EPO Thrombocytopenia_출혈 증상 및 징후 Thrombocytosis_염증, 빈혈, 종양
- Slides: 37