Causal Agent Several protozoan species in the genus









 -Secondary infection Amoeboma Obestraction intusssception -Invasion of blood")















, to invasive intestinal amebiasis")

")


 85 -95 % of cases. •")
 acute non suppurative hepatitis (2) liver abscess b.")



 is the drugs of choice. -For symptomatic")






. • Symptoms")



 • Symptoms usually within a few days after swimming in")











- Slides: 79
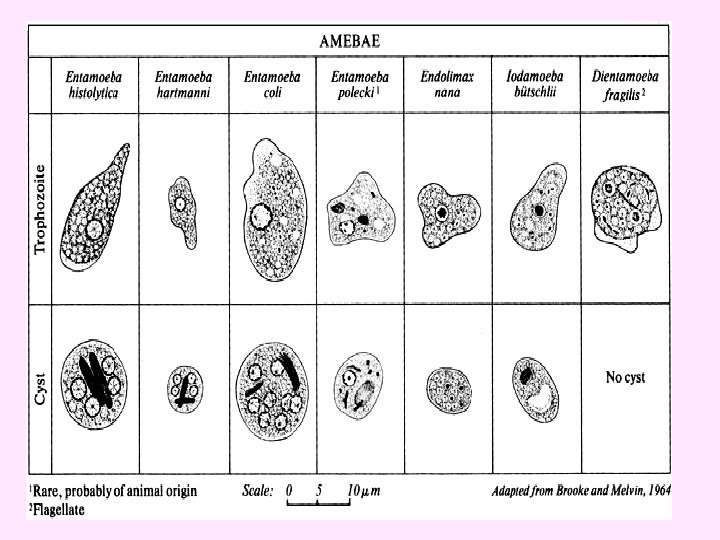
Causal Agent: • Several protozoan species in the genus Entamoeba infect humans, but not all of them are associated with disease. • Entamoeba histolytica is well recognized as a pathogenic ameba, associated with intestinal and extra-intestinal infections. • The other species are important because they may be confused with E. histolytica in diagnostic investigations.
Introduction Entamoeba histolytica 1. The only pathogenic amoeba among all of the intestinal amoebae. 2. Infecting perhaps 10% of the world's population. 3. Lead to invasive amoebiasis.
Entamoeba histolytica • Worldwide, with higher incidence of amoebiasis in developing countries. • risk groups include male homosexuals, travelers and recent immigrants, and institutional populations.
morphology
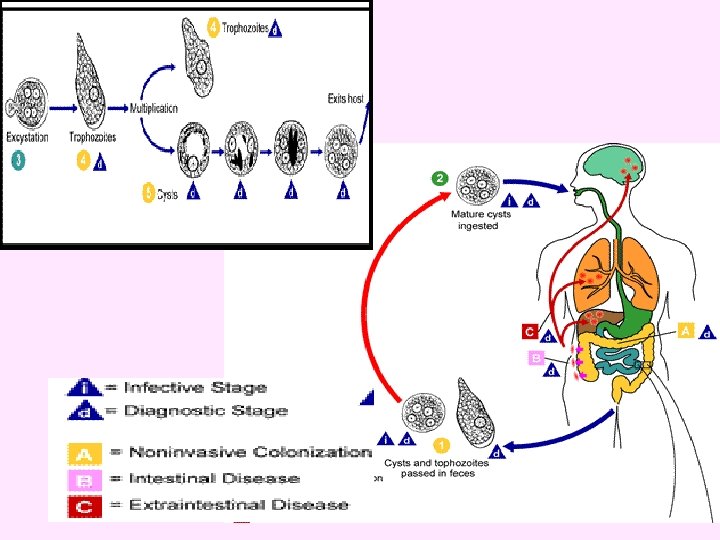
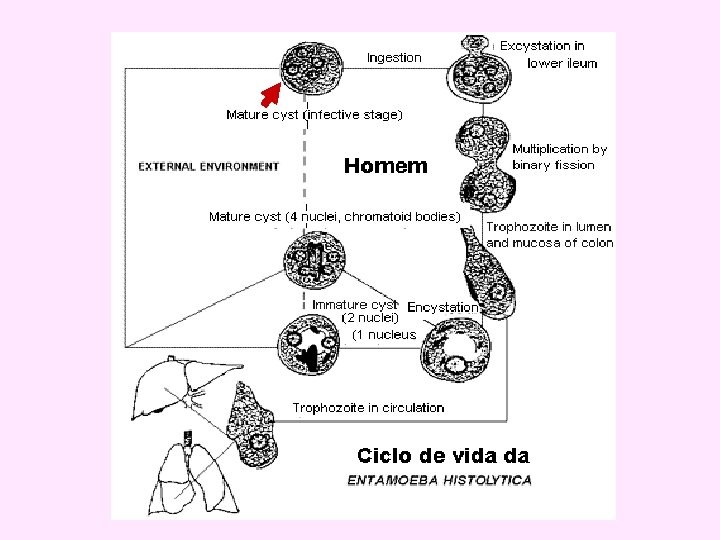
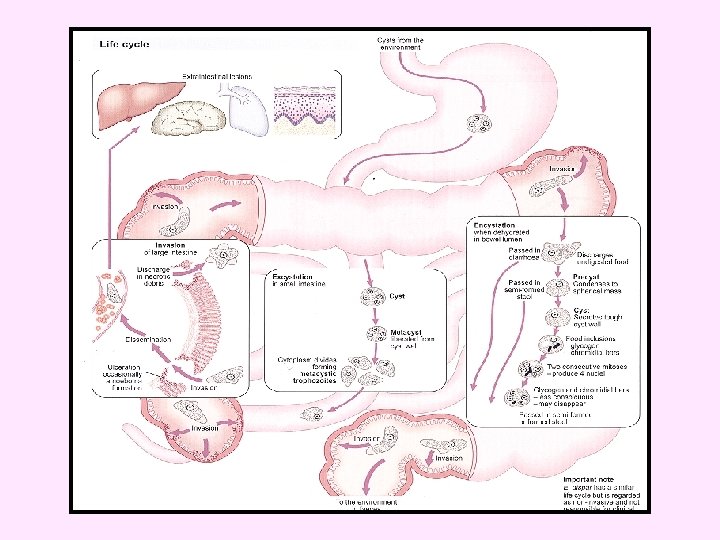
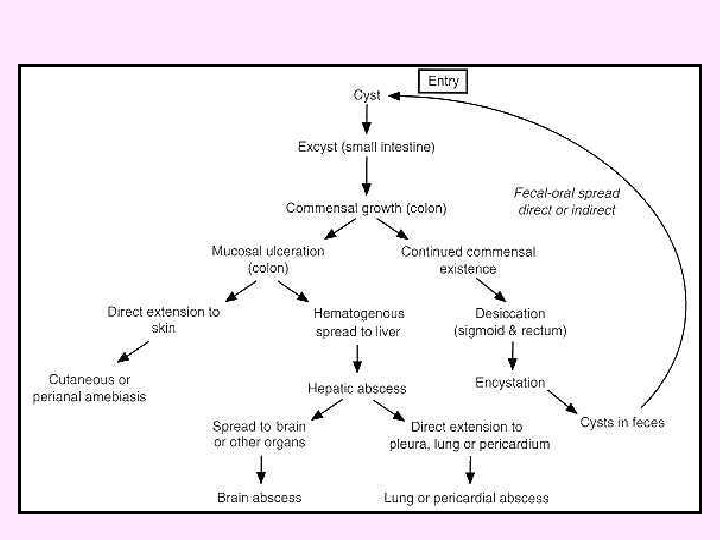
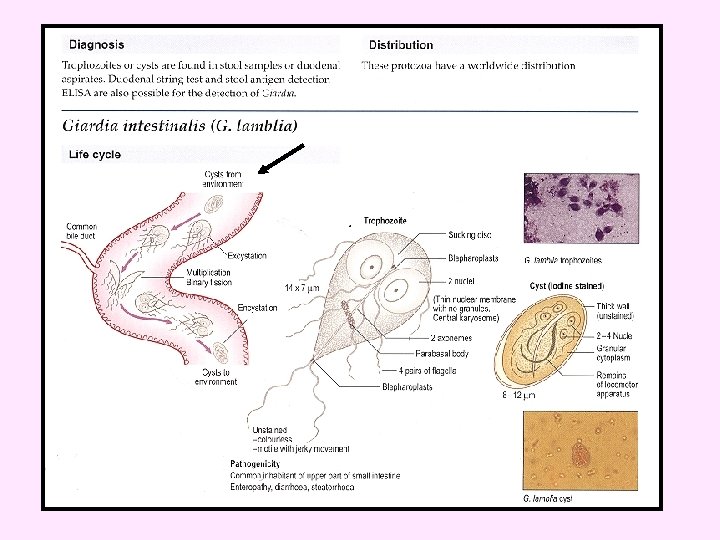
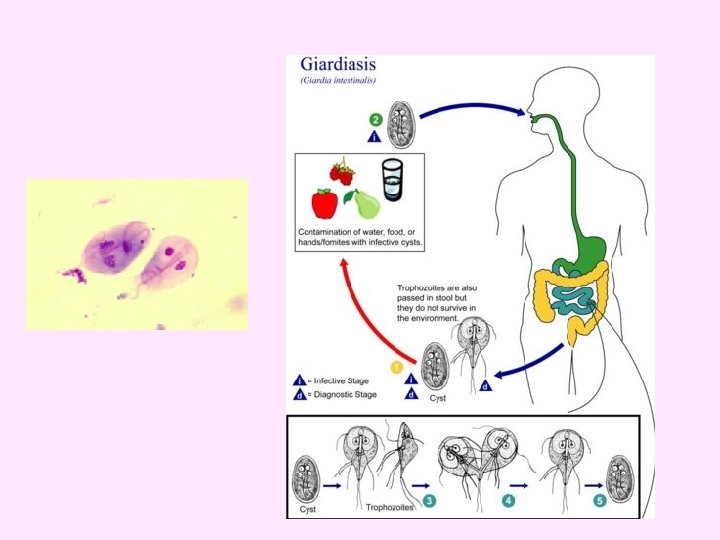
• • Life cycle Infection by Entamoeba histolytica occurs by ingestion of mature cysts in fecally contaminated food, water, or hands. Excystation occurs in the small intestine and trophozoites are released, which migrate to the large intestine. The trophozoites multiply by binary fission and produce cysts. Cysts and trophozoites are passed in feces Cysts are found in formed stool, whereas trophozoites are found in diarrheal stool.
E. dispar has similar live cycle but non invasive , not pathogenic. Viability : -Moist , cool condtion Up to 12 days -In water 9 -30 day Via polluted water; infected food handler, flies contaminating food, soil cultivation, direct contact
transmission. • the cysts can survive days to weeks in the external environment (protection by cyst walls) and are responsible for transmission. • Trophozoites in the stool are rapidly destroyed outside , and if ingested not survive in the gastric juice. • In many cases, the trophozoites remain confined to the intestinal lumen of individuals who are known as (non-invasive infection) cyst passer.
1 2 3 4 1 - the primary ulcer invasion of mucosa via crypts repair may occur. 2 - extension in mucosa muscularis mucosa relatively resistant. 3 -formation of sinus accumulation of amoebae superficial to muscularis mucosa with lateral extension of lytic necrosis; abscesses may coalesce under intact mucosa , mucosa may slough with widespread ulceration 4 -deep extension muscularis mucosa eventually pierced (direct or via blood) deep necrosis of sub-mucosa even muscle and sub-serosa
Complications and squeals -Perforation hemorrhage (rare) -Secondary infection Amoeboma Obestraction intusssception -Invasion of blood vessels. -Direct extension outside bowel -Pretonitis haemorrhag -Surronging inflammatory reaction -A mass under oedemotous mucosa Amoeboma clinically simulates neoplasm -Extraintestinal lesion
-Ulcer with peritonitis - hemorrhage - surrounding inflammatory reaction and fibroplastic proliferation a mass formed under edematous mucosa amoeboma (simulate carcinoma)
Extra intestinal extension
Extra intestinal extension Liver involvement - Secondary to - Concomitant with - Independent of
. A B
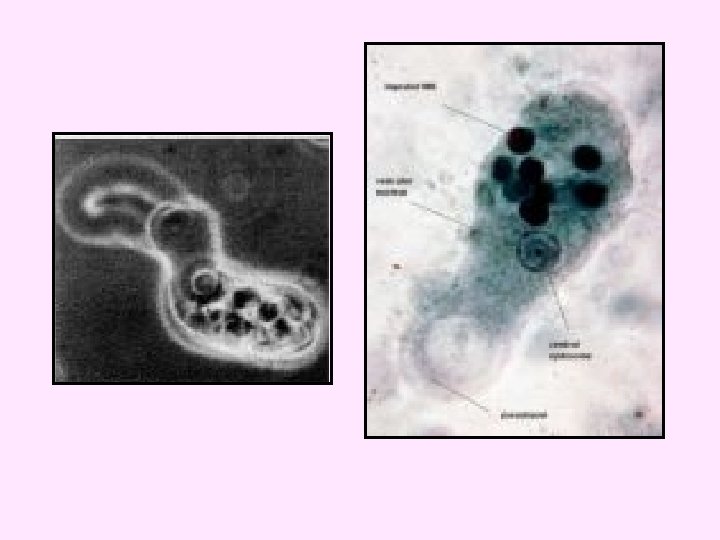
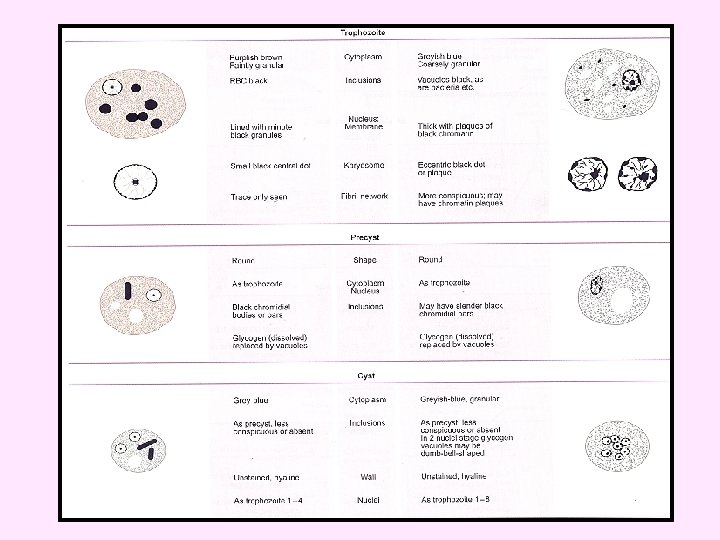
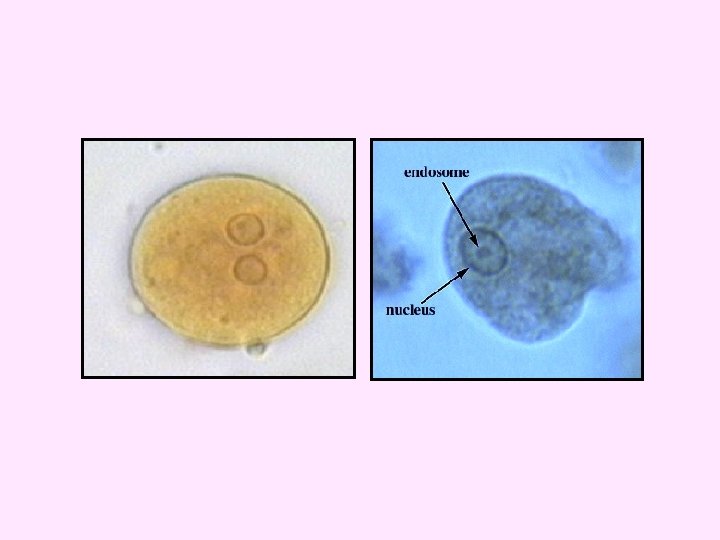
• the pathogenic E. histolytica is not morphologically differs from the nonpathogenic E. dispar! • Each trophozoite has a single nucleus, which has a centrally karyosome and uniformly distributed peripheral chromatin. • The cytoplasm has a granular or "ground-glass" appearance. • Entamoeba histolytica / E. dispar trophozoites measure usually 15 to 20 µm (range 10 to 60 µm), tending to be more elongated in diarrheal stool.
C D
erythro-phagocytosis, e Trophozoites of Entamoeba histolytica f with ingested erythrocytes. The ingested erythrocytes appear as dark inclusions.
• Erythro-phagocytosis is the only morphologic characteristic that can be used to differentiate E. histolytica from the non-pathogenic E. dispar
• The nuclei of Entamoeba histolytica have characteristically centrally located karyosomes, and fine, uniformly distributed peripheral chromatin. • The cysts contain chromatoid bodies , with typically blunted ends. • Entamoeba histolytica cysts usually measure 12 to 15 µm.
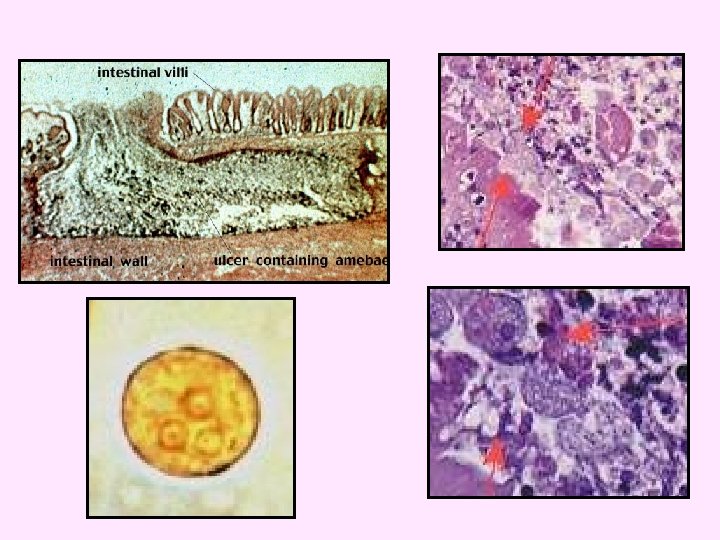
Mature. Entamoeba histolytica cysts usually measure 12 to 15 µm. cysts have 4 nuclei. h I
Entamoeba coli
Trophozoites of Entamoeba coli B A C
• Entamoeba coli -Trophozoites each have one nucleus with a large, eccentric karyosome and coarse, irregular peripheral chromatin. -The cytoplasm is coarse , vacuolated (dirty cytoplasm). - Cytoplasm contains ingested bacteria , yeasts or other materials. - The trophozoites of E. coli measure usually 20 to 25 µm, but it can reach up to 50 µm.
• Mature cysts typically have 8 nuclei, and measure about 20 -25 µm (range 10 to 35 µm). • Chromatoid bodies are seen less frequently than in E. histolytica. they are splinter like with pointed ends. • N. B. chromatoid bodies of E. histolytica have rounded ends.
Entamoeba coli cyst E D F
Clinical Features: A wide spectrum, from asymptomatic infection ("luminal amebiasis"), to invasive intestinal amebiasis (dysentery, colitis, appendicitis, toxic megacolon, amebomas), to invasive extra-intestinal amebiasis (liver abscess, peritonitis, pleuropulmonary abscess, cutaneous and genital amebic lesions).
pinpoint lesion on mucous membrane
flask-shaped (Ulcers)
Amoebic abscess in liver
Pathogenesis: Clinical classification • Intestinal Asymptomatic infection (carrier) 85 -95 % of cases. • Sympomatic cases 5 -15% a. Intestinal amoebiasis - a. dysentery (blood and mucus in stool) - b. non-dysenteric colitis - c. amoeboma
b. Extra-intestinal amoebiasis a. Hepatic (1) acute non suppurative hepatitis (2) liver abscess b. Pulmonary c. Brain, Skin, Other extraintestinal amoebiasis.
Hepatic amoebiasis: sing & symptoms • Local discomfort. • Malaise, fluctuant temperature • Toxemia. • Pain in right shoulder.
Diagnosis : intestinal Direct _ Microscopic identification of cysts and trophozoites in the stool _ trophozoites can also be identified in aspirates or biopsy samples obtained during colonoscopy or surgery. Indirect by immunodiagnosis (elisa)
Diagnosis: of Amoebic liver abscess • X-ray or ct scan show raised diaphragm • Blood picture –leucoytosis. • Serological test (elisa). • Examination of aspirate if indicated as treatment.
• Treatment: -For asymptomatic infections, (furamide) is the drugs of choice. -For symptomatic intestinal disease, or extra intestinal, infections (e. g. hepatic abscess), the drugs of choice are metronidazole or tinidazole, immediately followed by treatment with diloxanide furoate.
Prevention • human feces should not be used as fertilizer • food and drinks must be protected from flies. (mechanical transmission) • personal hygiene. wash hands after defecation and before meals. (autoinfection)
in summary pinpoint lesion on mucous membrane • flask-shaped Ulcers • Amoebic liver abscess • anchovy sauce sputum (lung) • brain , spleen , genito-urinary tract • amoeboma simulate carcinoma. - Cyst carrier is a healthy persons (trophozoite only in intestinal lumen Lumenal form). - Pre-employments Stool analysis was done for food handler.
FREE-LIVING PROTOZOA Ameba Diseases • Naegleria fowleri PAM • Acanthamoeba spp. GAE, skin or lung lesions, amebic keratitis.
Acanthameoba Have only 2 stage cyst And trophozoite. • Trophozoite and cyst are infective form. • portal of entry unknown, possibly respiratory tract, eyes, skin. • presumed hematogenous dissemination to the CNS. •
Acanthamoeba Encephalitis • infection associated with debilitation or immunosuppression. opportunistic parasitic inf. • chronic GAE (granulomatous amebic encephalitis). the organisms cause a granulomatous encephalitis that leads to death. • occurred in wearers of contact lenses.
Amebic Keratitis • Predisposing factors ocular trauma, contact lens (contaminated cleaning solutions). • Symptoms ocular pain, corneal lesions (refractory to usual treatments). • Diagnosis demonstration of amebas in corneal scrapings. • Treatment difficult, limited success corneal grafts often required.
Naegleria fowleri • found in fresh water. • ameba with loblose Pseudopodia. • motile bi-flagellated form. • PAM first recognized by Fowler (1965).
Primary Amebic Meningoencephalitis (PAM) • Symptoms usually within a few days after swimming in warm still waters. • Infection believed to be introduced through nasal cavity and olfactory bulbs. • Symptoms include headache, disorientation, coma.
Clinical picture A-Asymptomatic infection majority , about 80% B-Symptomatic infection: 1* typical picture most of symptomatic cases: incubation period 1 -2 weeks followed by diarrhea for bout 6 weeks. 2* atypical picture - malabsorption in children - fatty diahrrea - Sever diarrhoea.
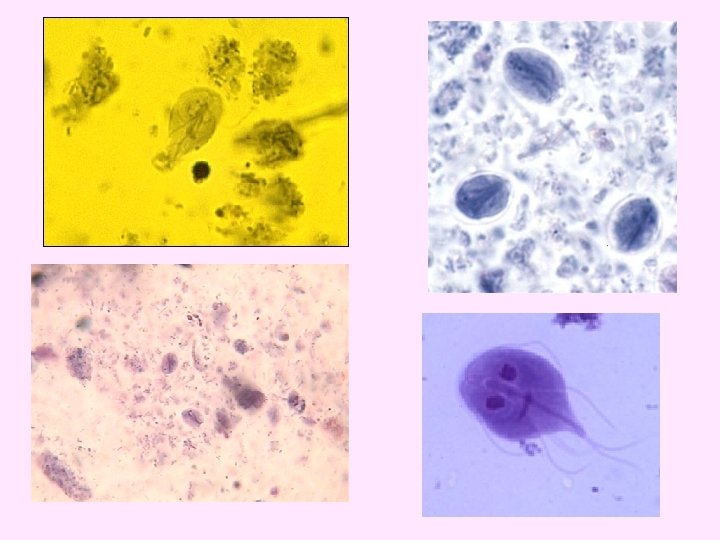
Laboratory diagnosis -Stool examination daily for three days. -Examination of duodenal aspirate, or by string (enterotest)
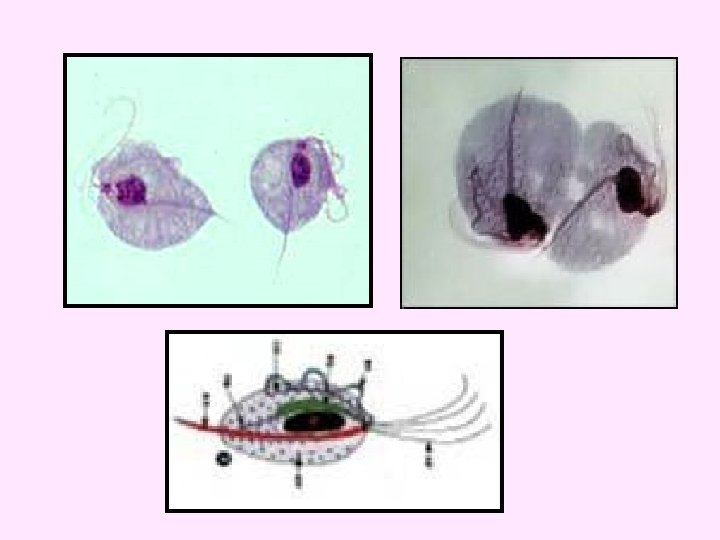
No cyst form
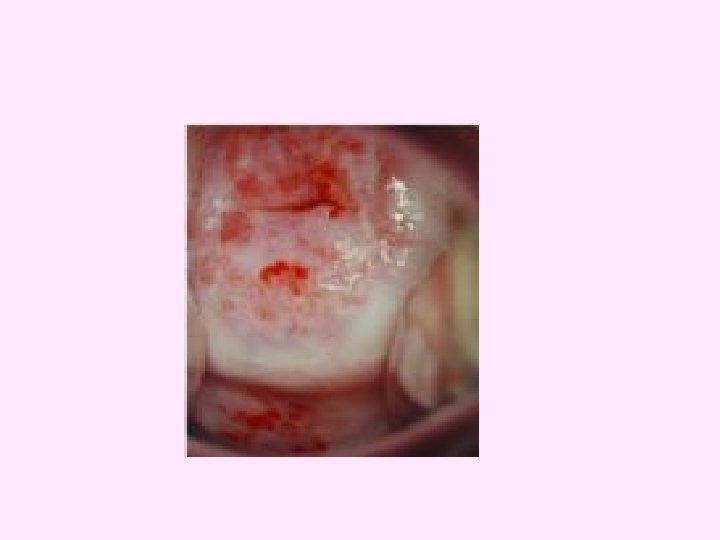
Trichomonas vaginalis • Transmission : sexual intercourse or contact with contaminated objects. • Pathology: • Female: vaginitis , profuse thin yellowish discharge with bad smell. • Male : invasion of urethra , prostate and seminal vesicles , causing urethritis but mostly asymptomatic.
• Diagnosis : identification of parasites by microscopy of discharge. (Examination of vaginal or uretheral discharge for T. vaginalis). • N. B. No cyst stage Imp
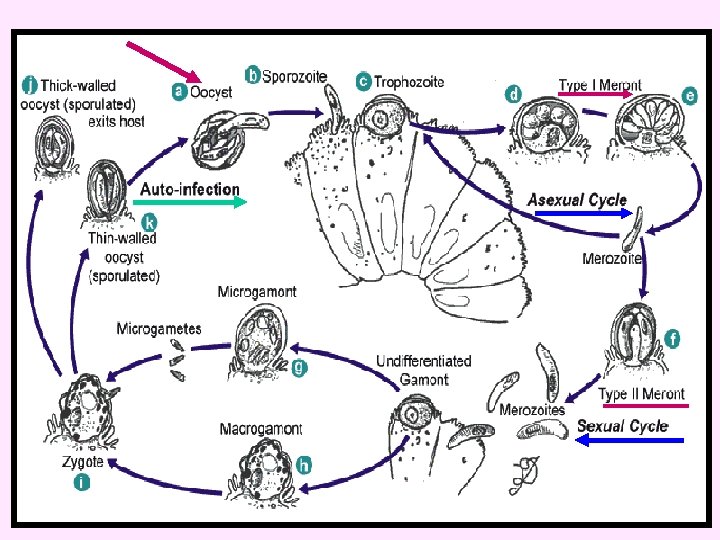
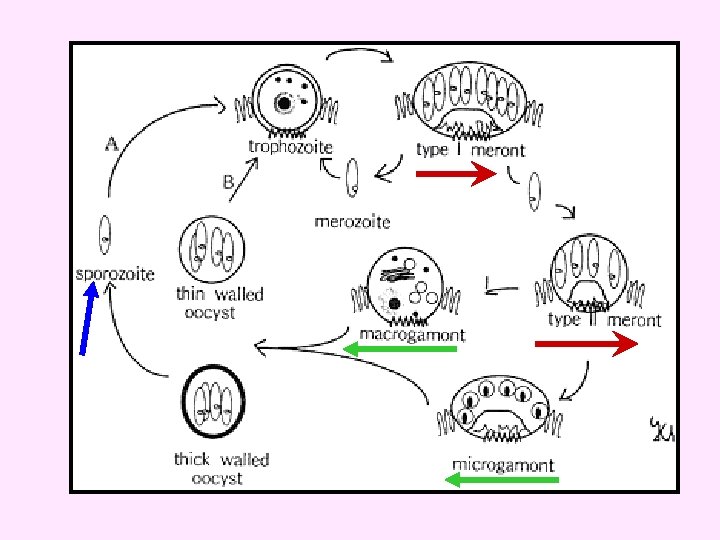
Cryptosporidium parvum
Cryptosporidiosis zoonosis, cosmopolitan, most human and animals infected by Cryptosporidium. Life cycle • Infective stage : oocyst with 4 sporozoites passed in feces. • Upon ingestion sporozoites are released. • Sporozoite penetrate intestinal epithelial cells and undergo two cycle : 1 -schizogony 2 -gametogony. • Sporulated oocyst , 4 -5 M (with 4 sporozoites) are passed in feces.
duodenal biopsy sample from a patient with AIDS and cryptosporidiosis
Pathology & clinical picture: • Immunocopetent persons asymptomatic or mild enterocolitis , last about 2 weeks. • Immunodeficient persons sever diarrhoea with malabsorption. Diagnosis & morphology: • duodinal biopsy : gametes or schizont (4 -8 merozoites) in epithelial cells. • Stools : oocyst 4 -5 m with 4 sporozoites (without sporocyst).
• Treatment - Self limited in immunocomptant persons , no effective drugs in cases of AIDS. - Management of fluid and electrolytes loss. • Prevention and control: -person-to person or animal to person transmission controlled by sanitation. -Identify common sources e. g. contaminated water