Catheter directed therapy for Pulmonary Embolism Saher Sabri

Catheter directed therapy for Pulmonary Embolism Saher Sabri , MD Med. Star Washington Hospital Center Med. Star Georgetown University Hospital

Disclosures • Advisory Board ▫ ▫ Medtronic Boston Scientific BTG Philips

 • Mechanical fragmentation of clot • Removal of clot •")
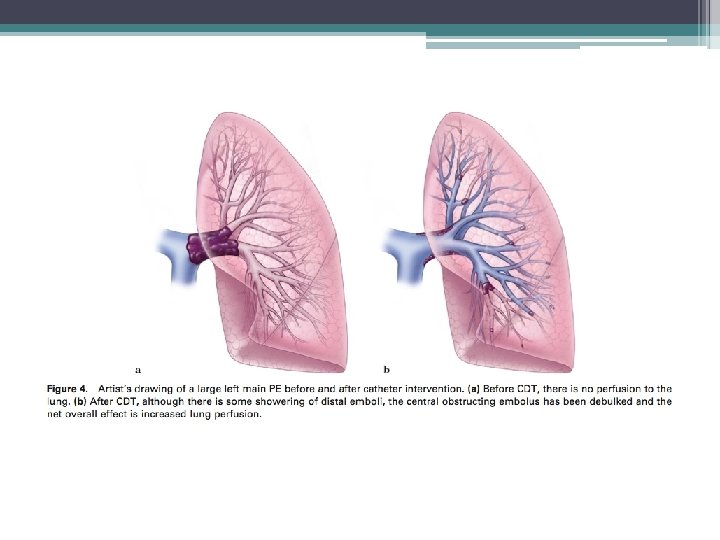
Cather Directed Therapy (CDT) • Mechanical fragmentation of clot • Removal of clot • Direct infusion of thrombolytic agents • Goal is to decrease right heart pressure by relieving central obstruction
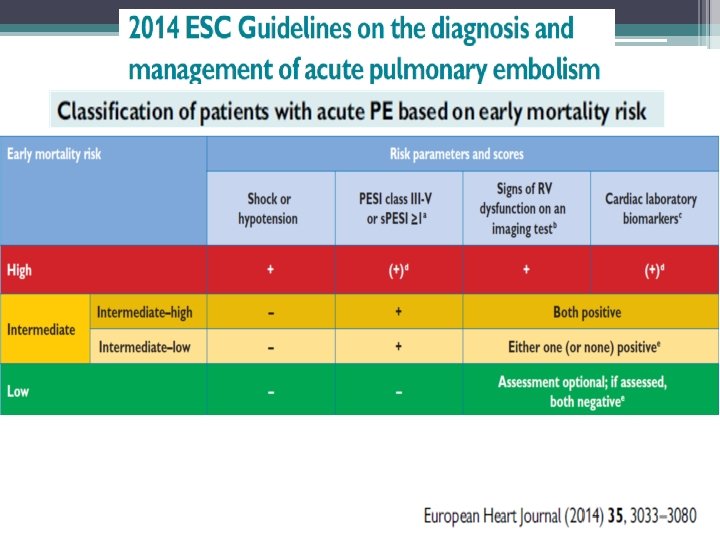
 • Submassive PE ▫ High-Intermediate risk PE (")
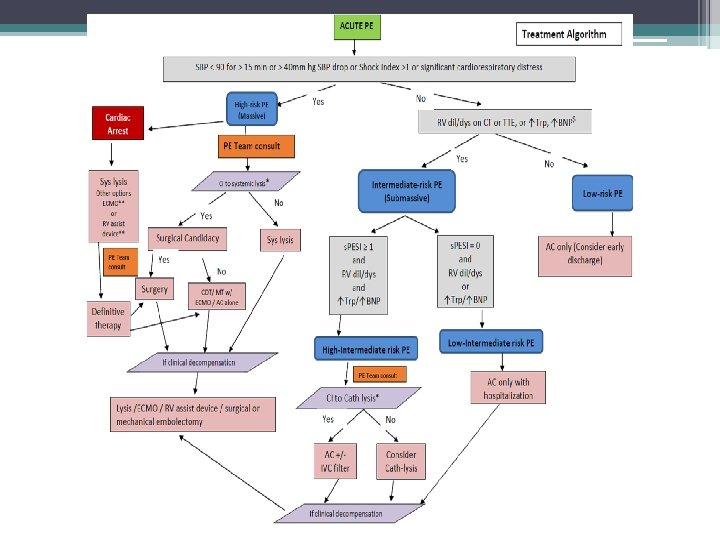
Indications for Catheter Directed Therapy (CDT) • Submassive PE ▫ High-Intermediate risk PE ( PESI >I, RV strain, elevated Troponins & BNP) • Catheter directed thrombolysis only • Mechanical thrombectomy carries a risk of acute worsening of RV dysfunction and should be used with caution • Patients with contraindication to thrombolysis and anticaogulation, may consider mechanical thrombectomy alone
 • Massive PE (Hemodynamic instability, defined as a")
Indications for Catheter Directed Therapy (CDT) • Massive PE (Hemodynamic instability, defined as a SBP of <90 mm Hg, a drop in SBP of >40 mm Hg or ongoing administration of catecholamines for systemic arterial hypotension or persistent hypoxemia despite appropriate anticoagulation and oxygen therapy) • Contraindication to sytemic lytics or lack of response to systemic lytics • Mechanical thrombectomy +/- catheter directed thrombolysis

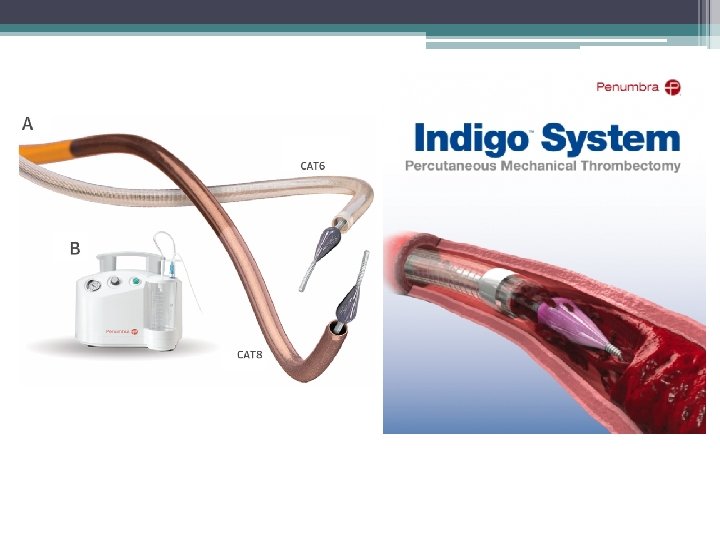
Mechanical Thrombectomy Devices. Use in Massive PE • • • Rotating pigtail catheter Guiding catheters Amplatz device (obsolete) Angiojet system( Black box warning) Angioplasty balloon Trerotola thrombectomy device (Arrow) Cleaner Device ( Argon) Indigo thrombectomy catheter ( Penumbra) Aspirex catheter ( Straub) JETi thrombectomy Inari thrombectomy

Procedural Tips • Femoral vs Jugular. Both work. I find it easier to get to PA from Jugular approach • 8 fr sheath provides a lot of options

Procedural Tips • Femoral vs Jugular. Both work. I find it easier to get to PA from Jugular approach • 8 fr sheath provides a lot of options • Start with a pigtail and obtain PAP • Keep sheath in RA for lysis. May need to advance into PA for thrombectomy ( femoral may work better for that)

Procedural Tips • Femoral vs Jugular. Both work. I find it easier to get to PA from Jugular approach • 8 fr sheath provides a lot of options • Start with a pigtail and obtain PAP • Keep sheath in RA for lysis. May need to advance into PA for thrombectomy ( femoral may work better for that) • Atraumatic 0. 035 stiff wire for exchnage. (Rosen wire)

Procedural Tips • Femoral vs Jugular. Both work. I find it easier to get to PA from Jugular approach • 8 fr sheath provides a lot of options • Start with a pigtail and obtain PAP • Keep sheath in RA for lysis. May need to advance into PA for thrombectomy ( femoral may work better for that) • Atraumatic 0. 035 stiff wire for exchnage. (Rosen wire) • If performing bilateral PA thrombolysis, we prefer two separate right IJ punctures or bilateral femoral puncture. Other option is to place a single sheath with a dual lumen adapter

Case • 62 year old male presenting with 24 hours of chest pain, hypoxia and dyspnea following prostatectomy + colostomy for recto-urethral fistula • Elevated Troponins • PMHx: HTN, hyperlipidemia, prostate cancer

Case • Initially taken to cardiac cath to rule out NSTEMI • Coronary angiogram which was negative for coronary disease • Developed hypoxemic respiratory failure intubated. • Echo showed RA fillig defect and severe RV dysfunction • Sent to CT

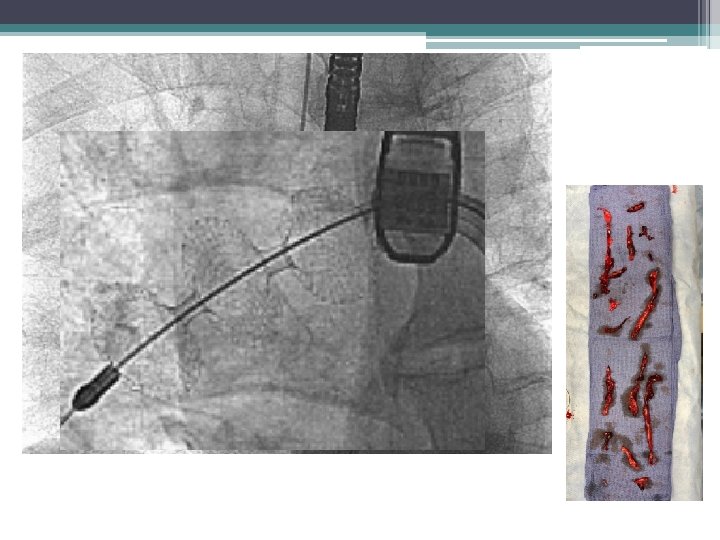
Blood pressure 83/47, pulse 130 Massive PE

12 mg TPA Rotating pigtail Aspiration through 8 fr guide cath

68 year old hypotensive on pressors, intubated
 Flow. Triever Device (“FT”) • Navigates through the")
Triever 20 (formerly Aspiration Guide Catheter) Flow. Triever Device (“FT”) • Navigates through the • Deployed out of right heart and delivers FT device to the pulmonary artery AGC and into thrombus • Disrupts, • Large bore catheter maximizes aspiration and collection of thrombus Disruption, maceration engages and moves large volume of thrombus and retrieval of clot Increased lumen Rapid flow restoration Reduced PA pressure Reduced RV strain 2 CONFIDENTIAL

Courtesy Shawn Sarin, MD

FLARE Study Summary Objective • Evaluate the safety and effectiveness of the Flow. Triever System for use in the treatment of Pulmonary Embolism Study Design • • Prospective, single-arm, multicenter study; 106 patients, 18 sites Follow-up at 48 -hours & 30 -days Results • • Effectiveness • Primary Endpoints • • Effectiveness – reduction in RV/LV ratio at 48 -hours Safety – Composite major adverse event rate Main Inclusion Criteria • • CTA evidence of proximal PE RV/LV ratio of ≥ 0. 9; Systolic BP ≥ 90 mm. Hg; Stable heart rate < 130 bpm Study Administration • • IDE study with all appropriate controls DSMB, CEC, & Independent Core Lab measurement of RV/LV ratio Presented in Late Breaking Clinical Study Session at SCAI on April 27, 2018 Manuscript accepted by JACCi • 0. 38 (25%) reduction in RV/LV ratio from 1. 53 at baseline to 1. 15 (p<0. 0001) • 48 hour post RV/LV measurement cohort (n=101) 2/106 patients given thrombolytics Safety • • 3. 8% MAE (4/106) § 1 bleeding complication (0. 9%) § 3 treatment-related clinical deterioration (2. 8%) No device related adverse events Other • • Median ICU stay 1 day (42% of patients did not go to the ICU) Median length of stay 3 days Conclusions • • • Catheter-directed mechanical thrombectomy using the Flow. Triever System, without the use of thrombolytics met the pre-established safety and effectiveness endpoints by improving RV function in patients with intermediate-risk PE The Flow. Triever System has the potential to reduce bleeding complications, total hospital stay, and ICU stay This study establishes mechanical thrombectomy for acute PE as a viable alternative to thrombolytic-based catheterdirected therapy and warrants further investigation CONFIDENTIAL

Courtesy Bao Bui , MD

JETi Thrombectomy Walk Vascular

Courtesy Bao Bui , MD
 • Submassive PE ▫ High-Intermediate risk PE (")
Indications for Catheter Directed Therapy (CDT) • Submassive PE ▫ High-Intermediate risk PE ( PESI >I, RV strain, elevated Troponins & BNP) • Catheter directed thrombolysis only • Mechanical thrombectomy carries a risk of acute worsening of RV dysfunction and should be used with caution • Patients with contraindication to thrombolysis and anticaogulation, may consider mechanical thrombectomy alone

2018 PERT Data Mortality: 14 -15% intermediate-risk and 11% low-risk PE Multi-center Consortium Registry 475 PERT activations across 8 sites, acute PE in 416 (88%) 3 to 13 (mean 8) activations/mo/1000 beds, 60% from ED 30 -day mortality in 70% anticoagulation alone; advanced therapy patients with PE stratified by risk groups* varied from 16% to 46% 30 day follow-up: Mortality: 16% overall, ranging from 9% to 44% in different centers High-risk: 27% (in discussion 31%) Intermediate-high: 14%, intermediate-low: 15% Low-risk: 11% Major bleeds: 13% overall Advanced therapy: 16% vs. anticoagulation: 12% (no difference) CDT: 19% Recurrent VTE: 7% Higher in advanced therapies: 11% vs. anticoagulation: 5%; higher-risk were more likely to receive advanced therapies * All category captures each site for a total of 338 patients captured Schultz et al. , EXPRESS: A Multidisciplinary Pulmonary Embolism Response Team (PERT) - Experience from a national multicenter consortium. Pulm Circ. 2019 Jan 11: 2045894018824563. doi: 10. 1177/2045894018824563 CONFIDENTIAL 3 Confidenti
 Angiojet system- Pulse")
Catheter-Directed Thrombolysis • • Multi-sidehole infusion catheter Ultrasound enhanced CDT (EKOS) Angiojet system- Pulse spray JETi Thrombectomy

Rationale for Catheter-Directed Thrombolysis • Systemic thrombolysis has 20% risk of major hemorrhage with 2 -5% risk of intracranial bleed • As many as 50% of patients with acute PE have contraindications to IV TPA • Catheter-directed therapy may be used to escalate therapy if systemic thrombolysis fails to result in improvement

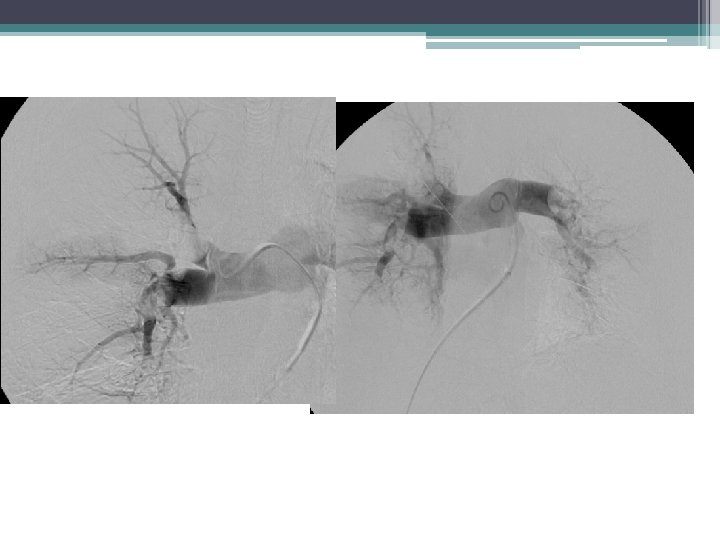
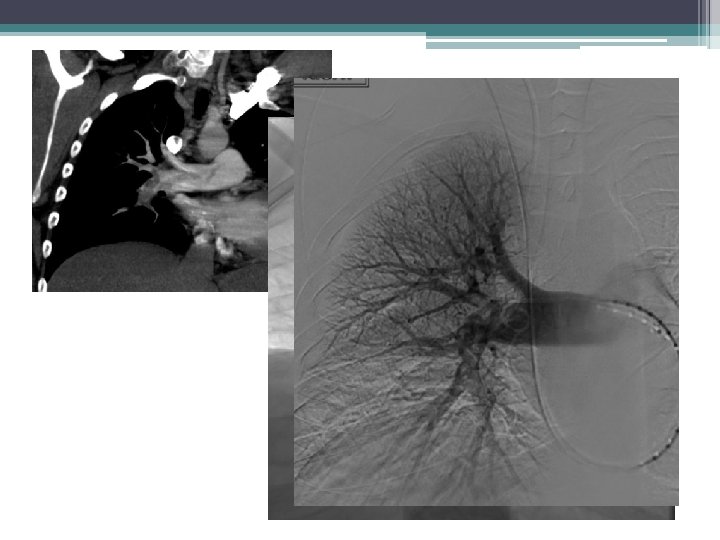
• 72 yr old with acute chest pain. Saddle embolus extending into right main PA. Echocardiogram showed moderate right atrium dilatation and sever right ventricular dysfunction. Tachycardia 110 -120. Normotensive. Elevated Troponins and BNP…High-Intermediate risk PE ( Submassive PE)


Catheter directed thrmbolysis 1 mg/hr TPA

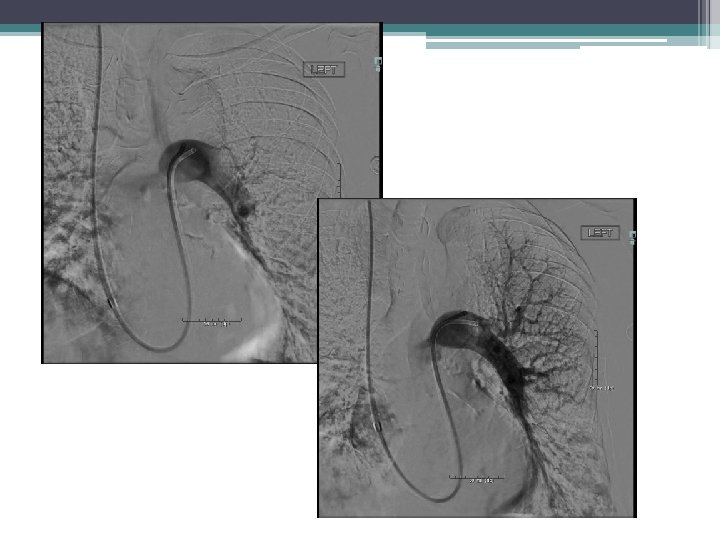
Mean PAP on initial study was 34 mm Hg. Post 12 hours of thrombolysis angiogram shows significant decrease in clot burden. Mean PAP was 15 mm Hg.

Ultrasound enhanced thrombolysis –EKOS 0. 5 mg /hr
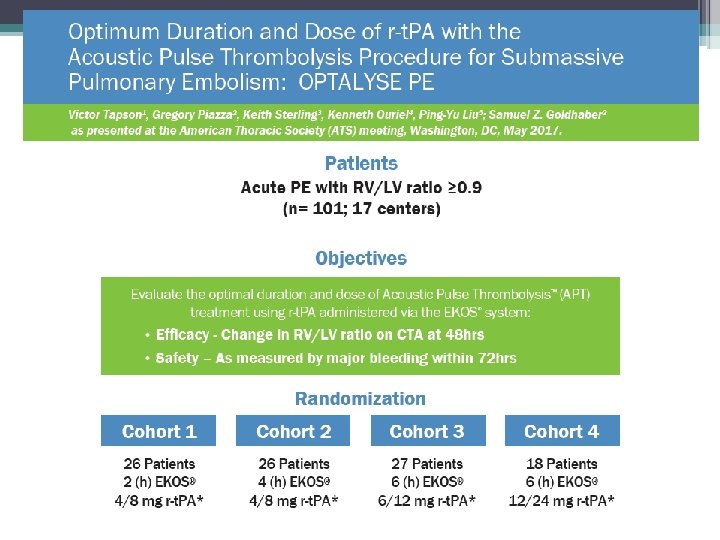
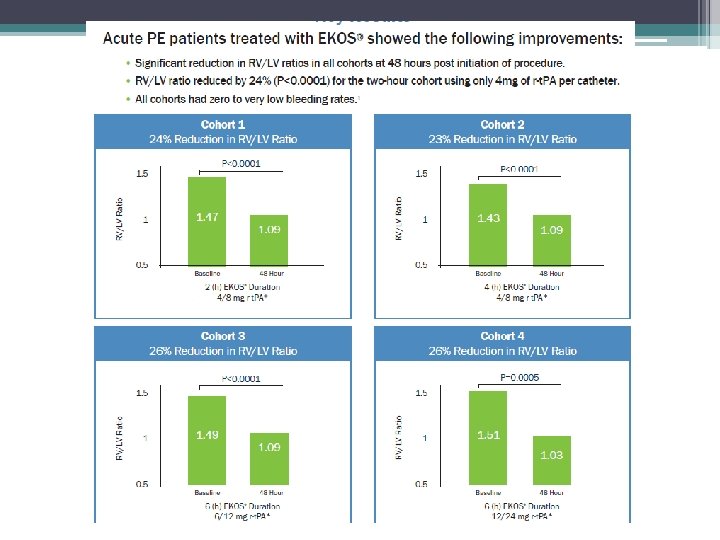
 ULTIMA (2014) Becattini et al (2010) Fasullo et al (2011)")
Study SEATTLE II (2015) ULTIMA (2014) Becattini et al (2010) Fasullo et al (2011) Mi et al (2013) N Treatment t. PA Reduction in RV/LV Ratio at 48 Hours 150 USAT 24 mg 0. 42 / 24% 30 USAT arm 10 -20 mg 0. 29 / 22% 30 -50 mg 0. 31 / 24% 100 mg 0. 40 / 27% 50 mg 0. 11 / 8% 28 35 57 Systemic Thrombolytic Major Bleeding Intracranial Hemorrhage PEITHO (t. PA arm) (Meyer G, et al. 2014) 58/506 (11. 5%) 10/506 (2%) SEATTLE II (Piazza G, et al. 2014) 17/150 (11. 4%) 0/150 (0%) OPTALYSE PE (Tapson V et al. 2018) 4/100 (4%) 2/100 (2%) Study

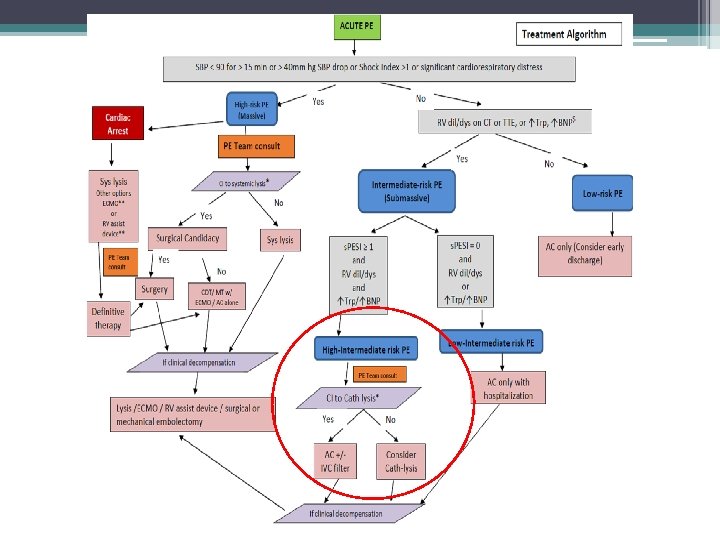
High-Intermediate Risk PE • Decision to CDT or AC alone • PERT Discussion is warranted • Favor CDT in younger patients who are symptomatic • AC alone in asymptomatic and older patients • Awaiting further studies on this patient population

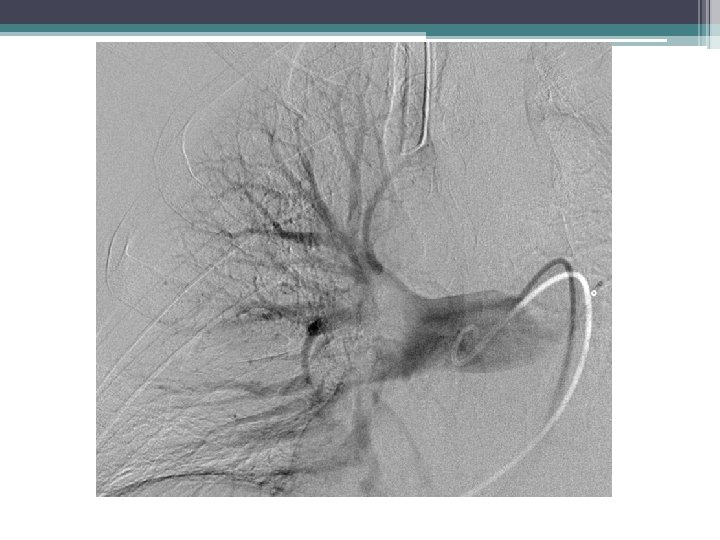
Case • 59 year POD 2. Three level laminectomy and Spinal fusion • Saddle embolus mostly left PA • Normotensive, Tachycardic 120 -130 • Severe RV dysfunction on Echo • Elevated Troponins • Hypoxic. High flow NC • C/I to AC and lytics • High-Intermediate risk PE ( Submassive PE)

Minimal flow to left PA


Catheter Directed Therapy • Massive PE. Nonsurgical candidates. Continued decompensation after IV TPA. ▫ Mechanical thrombectomy +/- catheter directed TPA • Symptomatic Submassive PE ( High. Intermediate Risk) ▫ Catheter directed thrombolysis ▫ Mechanical thrombectomy only if C/I to lytics
- Slides: 49