Catheter Based Treatment of DVT J Fritz Angle

Catheter Based Treatment of DVT J. Fritz Angle, MD University of Virginia Health System Charlottesville, VA

John Angle, MD Consultant Proteon disclosure Speaker: Siemens Medical Medtronic
 “symptomatic” proximal DVT randomized to")
ATTRACTive Intent • 692 patients with acute (14 day) “symptomatic” proximal DVT randomized to anticoagulation (control group) or anticoagulation plus pharmacomechanical thrombolysis • The primary outcome was development of the post-thrombotic syndrome between 6 and 24 months of follow-up (Villatta score>5) Vedantham S, et al. Pharmacomechanical Catheter-Directed Thrombolysis for Deep-Vein Thrombosis. N Engl J Med 2017; 377(23): 2240 -2252.

Quantifying PTS: The Villatta • The Villalta PTS Scale is composed of five patient symptoms (pain, cramps, heaviness, paresthesia, pruritus) and six signs (pretibial edema, skin induration, hyperpigmentation, venous ectasia, redness, pain during calf compression) on a 4 -point scale (0=none, 1=mild, 2=moderate, 3=severe) for score range of 0 -33 • This was done at 6, 12 , and 24 months by personnel blinded to treatment group Kahn SR. Measurement properties of the Villalta scale to define and classify the severity of the post-thrombotic syndrome. J Thromb Haemost 2009; 7: 884 -888

Un. ATTRACTive Results • Primary endpoint: No significant difference in the percent of patients with PTS (Villata>5) at 24 months: 47% in the CDT group and 48% in the control group; RR, 0. 96; 95%, CI 0. 82 to 1. 11; P=0. 56 • No significant difference in recurrent VTE at 24 -months (12% in the CDT group and 8% in the control group, P=0. 09) • CDT led to more major bleeding events within 10 days (1. 7% vs. 0. 3%, P=0. 049) • Change in QOL from baseline to 24 months did not differ significantly between the treatment groups. Vedantham S, et al. Pharmacomechanical Catheter-Directed Thrombolysis for Deep-Vein Thrombosis. N Engl J Med 2017; 377(23): 2240 -2252.

Positive Findings • Villatta scores for the post-thrombotic syndrome were lower in the CDT group than in the control group at 6, 12, 18, and 24 months (P<0. 01) (e. g. At 24 months 3. 40 versus 4. 56 (-1. 16) with p=0. 002) • Less leg swelling at 30 days (change, baseline to Day 30, -0. 77 (0. 17) versus 0. 26 (0. 17) (p=0. 034) • Moderate-to-severe post-thrombotic syndrome occurred in 18% of patients in the CDT group versus 24% in the control group (risk ratio, 0. 73; 95% CI, 0. 54 to 0. 98; P=0. 04) Vedantham S, et al. Pharmacomechanical Catheter-Directed Thrombolysis for Deep-Vein Thrombosis. N Engl J Med 2017; 377(23): 2240 -2252.

Femoral Popliteal Sub-Group Analysis Suggests Thrombolysis Not Helpful • No difference in incidence of any signs of Villalta scale ≥ 5, PTS scores, or quality of life score (p > 0. 5 for all comparisons) • No difference in leg swelling or pain at 10 or 30 days. • However, at 10 days, major bleeding occurred in three versus none (p = 0. 06) and any bleeding occurred in eight versus two (p = 0. 032) • Over 24 months, recurrent venous thromboembolism occurred in 16 PCDT and 12 no PCDT patients (p = 0. 24) Kearon C, et al. Pharmacomechanical Catheter-Directed Thrombolysis in Acute Femoral-Popliteal Deep Vein Thrombosis: Analysis from a Stratified Randomized Trial. Thromb Haemost. 2019 (in press)

Iliac Sub-Group Analysis Suggests Thrombolysis Is Helpful • Analysis still pending • Likely to show early and late benefit to CDT • Will not answer the question of Acute DVT in setting of anatomic abnormality, malignancy, hypercoagulability, or prior DVT

42 y/o Female presents with SOB History of DVT 3 years ago while on Gn. RH agonist therapy for menorrhagia. Treatment complicated by HIT

Screening Ultrasound Common femoral compressible

Thrombosis of large left GSV Discharged on coumadin

Returns one month later with new left leg swelling Now has extensive left leg DVT, despite maintaining INR 2. 2 -3. 2 (2. 8 on admission)

IVC Filter Placed for Extensive Iliac Thrombus Use of IVC filtration in LE CDT remains controversial

Mechanical Thrombectomy Filter allows us to be more aggressive Use rotating basket device when rheolytic devices is not sufficient.

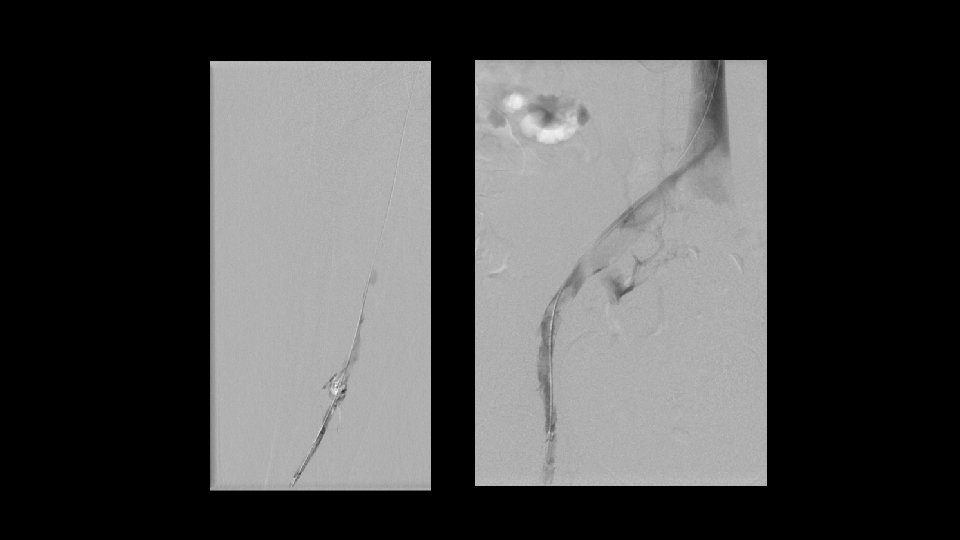
Insure Any Underlying Webs Gone Prior to Stent Placement


Left Iliac vein widely patent. Filter Removed. Note stent extends into IVC Discharged on Arixtra

Presents 2 Weeks Later With New SOB And Bilateral Leg Swelling F/U CTPA: Acute on chronic thrombus on right

Jugular approach venogram Left common iliac stent patent. New right thrombosis.

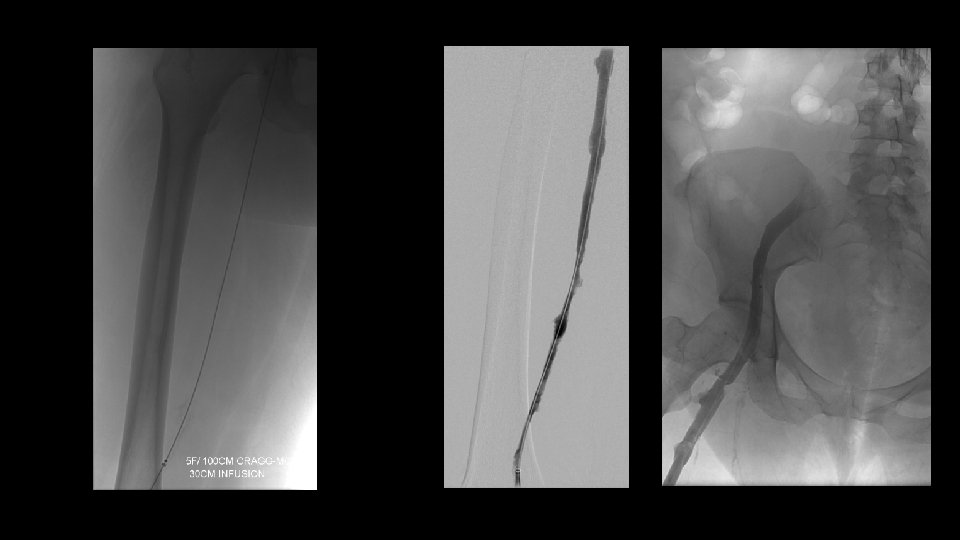
Filter placed. Thrombolysis of right leg initiated

Post thrombolysis Bilateral external iliac vein compression noted

External iliac vein compression did not respond to balloon dilatation

Bilateral EIV stents. Filter left in place. No further treatment of Left CIV stent

CT Performed to Assess the EIV Compression Found to have fluid filled pelvic mass compressing EIVs despite stents

S/P Pelvic Mass Resection Stents no long compressed New diagnosis of clear cell carcinoma

Why Get A Pre-Procedure CTV • Anticipate the proximal extent of thrombus (planning approach, determine need for filter, decide if unilateral versus bilateral lysis) • Differentiate intrinsic from extrinsic stenoses that we often encounter after lysis • Anatomy on venography often confusing in IVC stenosis or atresia • Treatment planning and patient consent

Beyond ATTRACT • Highly symptomatic Ilio-femoral DVT should be treated • Consider abdominal imaging before you treat • Procedure end point should not be duration of lysis but multi -modality confirmation of complete restoration of flow • There is new interest into whether acute or chronic phase iliac intervention is preferable for preventing severe PTS • There are high risk patients that were excluded from ATTRTACT that we must assess and possibly treat (oncology, hypercoaguable, recurrent DVT, and IVC interruption)
- Slides: 29