Caseous Lymphadenitis Myths Realities in Treatment and Prevention




 �Microscopic pyogranulomas �Coalesce to form larger")

 in 2 main forms �External form �")







 �Bovine �Cutaneous")



test �Measures Ig. G response to exotoxin in pt")

























- Slides: 46
Caseous Lymphadenitis: Myths & Realities in Treatment and Prevention Katie Simpson, DVM, MS, DACVIM Cross Timbers Large Animal Clinic April 30, 2016
Etiologic Agent �Bacteria from family Actinomycetaceae �Corynebacterium pseudotuberculosis �Also contains Mycobacterium, Rhodococcus, Nocardia �Non-motile pleomorphic rods �Gram-positive �Facultative intracellular � Grows under anaerobic OR aerobic conditions at 37°C �Groups show palisade or ‘Chinese letter’ arrangement in smears �Mycolic acids on outside of cell wall
Bacterial Characteristics: Susceptibility to Disinfectants �Common disinfectants kill the bacterium �Hypochlorite �Formalin & cresol �Presence of organic material = ↑ exposure time �Survives > 24 hours in sheep dips
Virulence Factors �Mycolic acid �Waxy coat on cell wall surface �Induces degeneration/death in leukocytes �May allow survival for long periods in environment � Can survive ≥ 6 months �Protection from lysosomal enzymes � Survives phagocytosis (being engulfed by white blood cells) � Allows bacterial migration �Contributes to abscess formation
Pathogenesis �Organism entry & spread �Local lymph node(s) �Microscopic pyogranulomas �Coalesce to form larger abscesses over 2 -6 months �Mineralization laid down in concentric layers w/ time �± Extension of infection via blood/lymphatics �Similar lesions in other organs �Survival/replication in macrophages �Potential for reactivation later on CHRONIC, LIFELONG DISEASE IS THE RULE!
Routes of Inoculation �Experimental �ID, SQ, IV, intratracheal, intravaginal, intralymphatic �Naturally occurring �Sheep: skin � Minor cutaneous wounds from shearing � Also castration, docking, umbilicus in neonates � Respiratory route not as likely �Goats: oral cavity or skin of face/head � Mutual grooming, head butting, ‘inquisitive behavior’ � Breaks in skin/mucosa
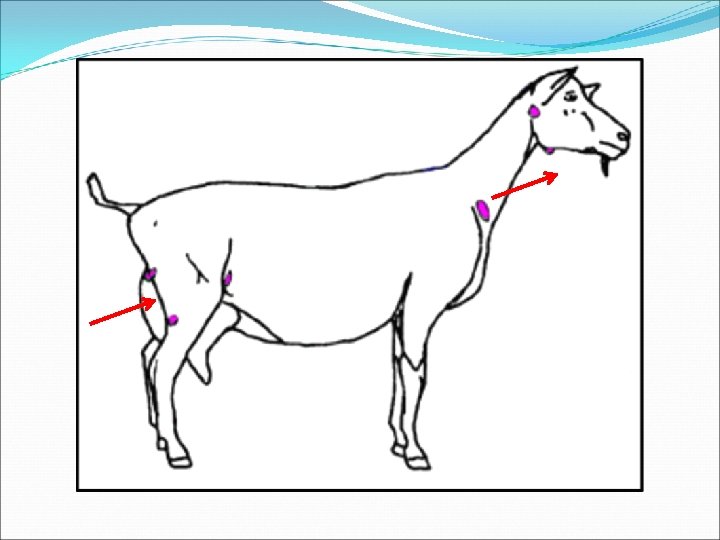
Clinical Features of CLA �Pyogranulomatous lesions (abscesses) in 2 main forms �External form � Aka ‘superficial’ or ‘cutaneous’ � Characterized by abscessation of external lymph nodes �Internal form � Aka ‘visceral’ � Abscesses in internal llnn. & other organs �BOTH forms may coexist in same animal!
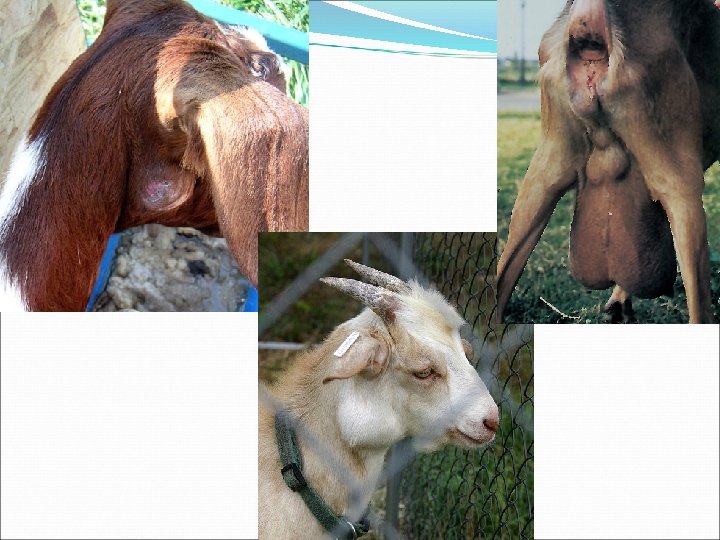
External CLA �Most common form in GOATS �Superficial lymph node abscesses �Diameters of 3 -15 cm �Principal lymph nodes affected �Goats: head & neck � Submandibular, parotid, prescapular �Sheep: torso � #1: Prefemoral, #2: prescapular
Internal CLA �Less common than external form? ? �More frequently see internal form in SHEEP �Chronic weight loss, ill-thrift, ‘thin ewe syndrome’ Photo from Merck Veterinary Manual, courtesy of Dr. J. Glenn Songer �Principal organs involved �Sheep: lung parenchyma & mediastinal llnn. � Lung abscesses, less commonly bronchopneumonia � Mediastinal llnn. can get large enough to compress esophagus �Liver, kidneys, udder � More rarely spleen, heart, testis, scrotum, uterus, joints, brain, SC
Summary of CLA by Species Sheep Goats Most common form Internal External llnn. most affected Torso: Prefemoral Prescapular Head/neck: Submandibular Parotid Prescapular Abscess content Caseated, ‘onion layered’ Uniform, pasty, green
Transmission �Rupture of superficial abscesses �Contaminates environment for extended period �Direct contact OR via fomites �Lung lesions �Discharge into airways �Aerosolize organisms �Exacerbated by close contact & reduced airflow
Transmission: Introduction of Infection �Naïve flock/herd �#1: Clinically or subclinically infected carrier animal �Fomites � Farm workers/shearers � Shearing equipment � Portable handling equipment � Hay? ?
Risk Factors �Minor skin damage from shearing �Increased if plunge/shower dipping done w/in few days �Close confinement �Increasing age �Dusty environment
Other Species Affected �Equine �Ulcerative lymphangitis, contagious folliculitis/furunculosis, abscessation (internal or external) �Bovine �Cutaneous excoriated granulomas �Mastitis, mixed, visceral also possible �Camels & camelids �CLA �Severe lymphadenitis (camels only)
Zoonotic Potential �Most human cases occupational �Shepherds, farmers, shearers, abattoir workers, butchers… �Vets! �Chronic localized suppurative granulomatous lymphadenitis �Axillary, inguinal, or cervical lymph nodes �Occasional pneumonia, no fatalities reported �Most cases require surgical excision �Systemic antibiotics usually unrewarding
CLA Diagnosis: Clinical Pathology �Suggestive w/ clinical signs, NOT definitive �CBC �±Anemia of chronic disease �±Leukocytosis w/ neutrophilia �±Hyperfibrinogenemia �Biochemistry panel �±Hyperglobulinemia �± Suggestive of organ damage
Diagnosis �Culture of organism �Can typically isolate from lesions of all ‘ages’ �Lower number of viable bacteria in chronic abscesses �From transtracheal wash if suspect internal form in lungs �PCR �Multiplex PCR w/ 95% sensitivity � Human test to distinguish from C. ulcerans �More rapid, definitive than culture �Increases likelihood of dx in animals w/ mixed infections
Diagnosis: Serology �Synergistic hemolysis inhibition (SHI)test �Measures Ig. G response to exotoxin in pt serum �CANNOT differentiate exposure/previous dz now cleared/active draining external infection/internal abscess � Vaccinated animals usually have titers � Don’t cull a genetically valuable animal w/ 1 positive titer! �Low/no titer doesn’t rule out disease! � Sensitivity 81%, specificity 40% in recent study � Washburn et al. � Acute onset w/ rapid maturation, thick capsule, ab consumption
Diagnosis: Imaging �Positive titer OR �Evidence of external lymph node abscessation �Current or previous �Plus…
US Pix
Additional Diagnostics… �Radiographs �Intrathoracic disease �Computed tomography?
Treatment Strategies �Antimicrobial therapy �Efficacy poor when used alone �‘Lance & live with it’ �Attempt to minimize spread/contamination �Isolation �Intralesional therapy �Eradicate
Antimicrobial Therapy �Pharmacological treatment VERY difficult �Thick wall of abscess hinders penetration of drug �IC location limits some antimicrobials’ actions �Good in-vitro activity �Penicillin, TMS, tetracyclines, cephalosporins, rifampin �Ampicillin, florfenicol, tylosin, tulathromycin � Washburn, unpublished data �Outcomes… �Best-case scenario: reduced abscess size, nonrecurrence �Worst-case scenario: rupture & drain, exposure
Lance & Live With It �Treat it like any other abscess…. but expect it to return �Allow abscess to mature! �Establish adequate ventral drainage � Collect & dispose of exudate � Attempt over a drain, then clean/disinfect—esp. in your clinic! �Lavage w/ antiseptic solution � Iodinated or chlorhexidine �Consider additional tx if cellulitis �Antibiotics �Anti-inflammatories
Minimize Spread/Contamination �Surgical excision of abscess/lymph node �Primary closure �Difficult in areas with prominent neurovascular supply � Parotid lymph node �Follow up with long-term antibiotics � Minimum of 4 -6 weeks suggested �Does not address recurrence/spread �More expensive option �+ Local or general anesthesia
Minimize Spread/Contamination �Split into ‘infected’ and ‘clean’ groups �No sharing of feeders/waterers �Isolate/confine infected �Can treat abscesses as they occur �OR confine while actively draining �Kids/lambs from infected animals �Remove from dam at birth �Raise on heat-treated colostrum/pasteurized milk �Cull repeat offenders
Minimize Spread/Contamination �Closed-system saline lavage �Large bore needle, remove purulent debris, then…. �Intralesional OR parenteral (SQ) tulathromycin (2. 5 mg/kg) � 83 & 82% resolution of external abscesses � 1 month follow-up � Washburn K. E. ; Bissett W. T. ; Fajt V. R. ; et al. Comparison of three treatment regimens for sheep and goats with caseous lymphadenitis. JAVMA, 2009. 234(9): 1162 -1166.
Minimize Spread/Contamination �Current standard protocol for CL at one institution �Intralesional tulathromycin + SQ in neck � 2. 5 mg/kg once � May increase efficacy if give 3 SQ treatments, 1 week apart � At least as defensible & better biosecurity than ‘lance & live with it’ � In a follow-up study, same group had NO recurrences at same site & only a handful of new lesions elsewhere with this treatment (Washburn, personal communication) � Follow-up of 13 -14 months � Only external lesions evaluated
Tulathromycin: Draxxin® �Macrolide family �Triamilide �Highly lipid soluble �Labeled for RD in cattle & swine �C. pseudotuberculosis has in-vitro susceptibility �Lung tissue concentrations higher than MIC for 7 days � Sustained therapeutic concentrations in infected tissues �Withdrawal times for goats at previous reported dose �Meat 23 days (Young, Smith, & Leavens et al. ‘PK of tulathromycin following SQ administration in meat goats’, Res Vet Sci 90 (2011) 477 -479) �Milk 45 days (Washburn, FARAD)
Eradication �Culling of genetically superior animals �Not ideal �Some owners prefer this! �May not be as efficacious as one would think…. �W. TX goat herds utilizing the ‘cull’ approach w/ endemic CL still had a prevalence rate of 6% �Prevalence rates did not seem to decrease until treatment instituted �Still should advocate culling of repeat offenders following tx. !
Control Measures: Vaccination �Bacterin vaccines � Formalin-killed whole cells �Toxoid vaccines � Recombinant derivative of PLD exotoxin �Combined vaccines � Only commercially available product currently in US �Live vaccines �Autogenous vaccines � Can be used in goats but $$$$$ � Some feel works better than commercial vaccine � Caution: can kill the animal if not properly prepared/tested
Commercial Vaccines �In the US: Colorado Serum Company �Caseous D-T �C. pseudotuberculosis bacterin-toxoid �Clostridium tetani-perfringens type D �Price: $0. 58/dose �Case-Bac �C. pseudotuberculosis bacterin-toxoid �Price: $0. 70/dose
Advantages to Vaccination �Sheep efficacy study by CSC � 90% protected from internal form � 58% protected from external form �Reduction in disease severity � Decreased # of lesions in those that did develop CLA � Vaccinated: 1 lesion/animal � Non-vaccinated: Avg 36 lesions/animal
Disadvantages Labeled in sheep only Vaccinated prior to exposure Doesn’t prevent infection Post-vaccine lameness 24 -48 hours Mild lethargy, depression Injection site reactions Worse if already infected Renders serology useless $$$
Commercial Vaccine Use in Goats? �Off-label use in goats frequent � Currently no efficacy studies in goats � Anecdotal efficacy: not as good as sheep � Dawson, unpublished data: Approx. 50% efficacy w/ external lesions �Goat vaccine expected by CSC within 1 year…for the past several years �Current vaccine safety issues � Injection site reactions up to 14” diameter � Post-vaccine lameness up to 30 days � Fever � Lethargy, depression, ‘antisocial’ behavior � Anorexia, hypodipsia � Decreased milk production
Commercial Vaccine Use in Goats… �Anecdotal �In some herds with an endemic problem…seems beneficial in terms of limiting number of lesions � Still have issues with ‘vaccine safety’ �In some herds, seems to do nothing �In herds without evidence of clinical CLA…stay away from the vaccines!
Goat-Specific Bacterin, Texas Vet Labs
Texas Vet Labs Vaccine… �Conditionally licensed �Dependent on state �Approved in Oklahoma �Must check with state vet
Environmental Control �Quarantine /test new arrivals!! �Feeders �Source of fomite transmission �Bacterial survival weeks-months �Lower risk � Feeder that animals do not put their head through �Shearing equipment �Fresh clothing, wool bags, footwear �Grooming equipment �Bedding
Additional Management Strategies �Sheep �Isolate young/recently shorn from older �Shear young sheep first �Reduce time animals are held together after shearing �Minimize use of dips for ectoparasites � Particularly 2 weeks following shearing �Goats �Control of external parasites � Pruritus = rubbing on posts, nails, etc.
Additional Management Strategies �Both species �Needles, tattooers, surgical instruments sterilized after one use �Wounds treated promptly �Dip umbilicus at birth �Ensure no nails/wires present in housing facility
Questions?