Case Presentation R 1 20140117 Basic Data NameO

Case Presentation R 1林靜微 2014/01/17

Basic Data Name:高O斌 p Gender:male p Age: 15 y/o p Chart Number: 072749 XX p Date of Admission: 2013 -12 -25 p p Chief Complaints Intermittent fever (38 -40 C) every day for 3 weeks

102. 07 Admitted to 新樓 H. for one day -> Chronic diarrhea with ascites Subsided spontaneously -> Colonoscopy: focal lymphoid aggregate in the colonic mucosa and no evidence of malignancy. 09/24 學校健檢 U/A: protein: +2 BUNL/Cr: 21/1. 0; albumin: 4. 6 10/11 Our pediatric OPD - U/A: normal - Renal echo: Left mild hydronephrosis - 24 hours protein loss: 140 mg/day - 24 hr CCR: 82 ml/min
 for one week -cluster of")
12/13 Rheumatology Dr. 吳 -intermittent fever(BT 38 -39 C) for one week -cluster of painful oral ulcer noted over hard palate at the same time -no URI symptoms, dysuria, diarrhea -no erythematous skin lesions -Management: septic workup, survey for autoimmune dx transfer the patient to PED ID OPD and dermatology OPD (skin change noted at bilateral lower leg(LMD d/dx: ichthyosis )


12/16 PED ID OPD -Still intermittent fever up to 38 -40 C every day, and most episodes of fever occurred in the afternoon and evening -CXR (PA) + R' lateral view: mild increased perihilar infiltration, no pleural effusion, no LAP -PPD test: negative -Body Temperature record Dermatology OPD - Skin biopsy: Pathological Diagnosis: Compatible with X-linked ichthyosis, right forearm

12/20 Rheumatology OPD follow up -Occult maligacny or infection can not be ruled out -Check ds-DNA Ab, SSA/SSB Anti-n. DNA Ab 1: 160

12/24 PED Neurology OPD -Chills or tremor, duration around 1 min amplitude from small to large for 1 -2 months -NE: cranial nerve ok no focal weakness DTR hyporeflexia barely + Babinski sign: no response -Arrange EEG and NCV 上下肢 motor + sensory
 every")
12/25 PED ID OPD follow up - Intermittent fever (BT 38 -39 C) every day for 3 weeks - Fever of unknown origin more likely autoimmune disease - Suggest admission

Past history p p p p Birth History: G 4 P 4, NSD, GA: FT weeks, BBW: unknown, DOIC(-), PROM(-), Apgar score: ? Feeding: On full diet Vaccination: As schedule Growth and Development: BW: 52. 2 Kg(25 -50 th%), BL: 168 cm(50 -75 th%), BMI 18. 49 kg/m 2 Developmental milestones: WNL Hospitalization history: 2013. 07 chronic diarreha with ascites, admitted to 新樓 hospital for one day No major disease before

Personal history p Travel history: denied Occupation: student Contact history: denied Cluster history: denied p Current Medications: Nil p p p

Family history father and brother: ichthyosis Father work in 中國大陸, 主要照護者: 伯母
, Fever (+), Body weight loss(+,")
Systemic review p p p General: poor activity (+), Fever (+), Body weight loss(+, 8 kg within 6 months), Malaise (+) Cardiovascular: Tachycardia (-), Central cyanosis (-) Pulmonary: Cough(-) with sputum(-), Wheezing(-), tachypnea(-) with retraction (-) p p p Alimentary: poor appetite (+), abdominal discomfort (-), nausea (), vomiting (+), bowel habit change (-), diarrhea (+, 2 -3 times/day) Genitourinary: dysuria (), nocturia (-), foamy urine(+) Skeletal: ROM: no limitation

Physical Examination p p p Vital Sign:T: 36. 4度, P: 114/min, R: 24/min, BP: 81/58 mm. Hg Consciousness: drowsy Sclera: not icteric; Mouth: no oral ulcer, dry oral mucosa; Neck: supple, LAP (-) p Chest: Inspection: symmetric expansion Palpation: no crepitus p Percussion: resonance Auscultation: normal BS p Heart: Palpation: no heave, no thrill Percussion: no increase of dullness Auscultation: RHB, no murmur Abdomen: Inspection: globular Palpation: soft, not palpable liver and spleen, pain (-), tenderness (-), rebound (-) Percussion: tympanic, No shifting dullness Auscultation: BS: normoactive Limbs: warm, no edema, cyanosis (-), lateral weakness (-), palmar erythema (-) Peripheral pulse: symmetric and active Skin: no edema, petechiae or ecchymosis, dry skin, ventral finger vasculitis(+), ichthyosiform scaling over the extremities

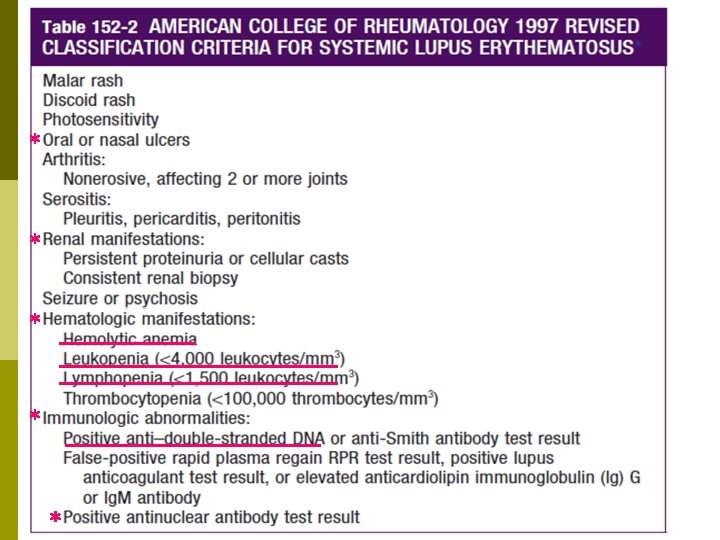
Vasculitis, favor SLE related, ventral fingers Diffuse ichthyosiform scaling over the extremities

Impression p Suspect systemic lupus erythematosus with multiple organ involvement

Plan p p p CBC, DC, Reti, ESR, PT/APTT, HPT, Lactate, Sm/RNP, ACA-Ig. M, ACA-Ig. G, beta 2 -GP I Ab, DAT, IAT, Na/K/P/Ca, CK, BUN/Cr, AST/ALT, LDH, CRP, ALB U/A and 24 hours Cr Cardiac sonography for evaluation pericardial effusion NCV-upper and lower extremities and EEG (awake and sleep) Consult ophthalmologist Record I/O and BW

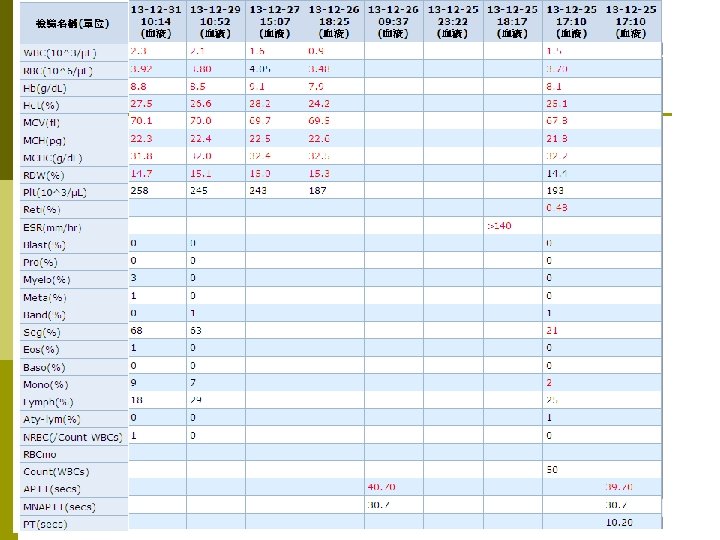
Lab data
 (-) *p-ANCA (+) May increased risk for lupus nephritis")
(-) (-) *p-ANCA (+) May increased risk for lupus nephritis

Antiphospholipid antibody

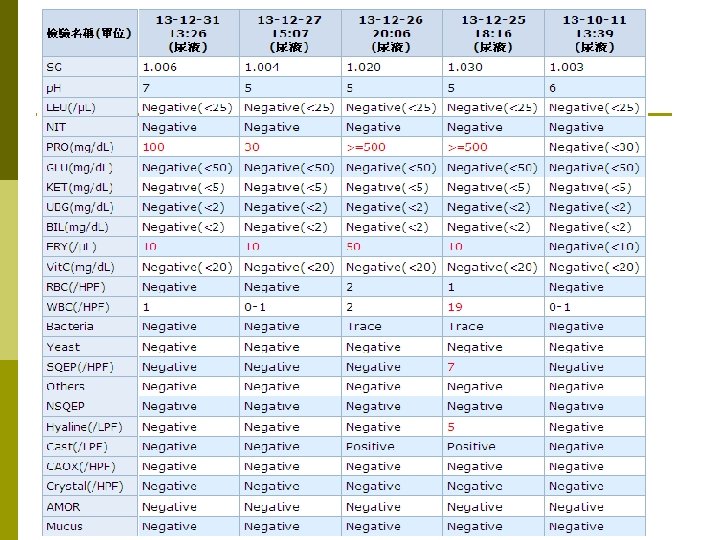
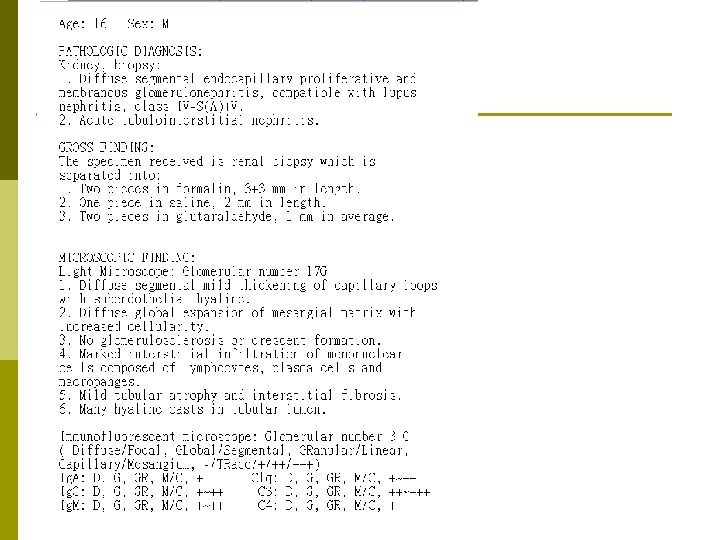
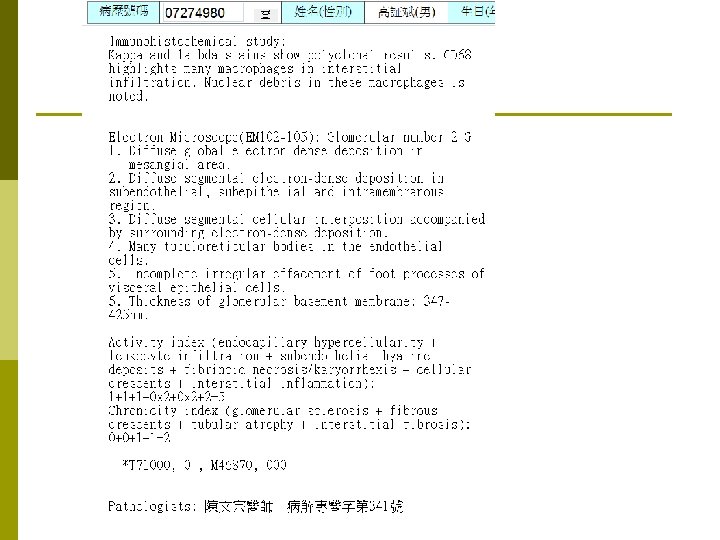
12/25 Urine routine TP: 891 mg/d. L, 24 hrs urine: 1212 ml 24 hrs protein loss: 10. 8 g Renal echo 1. Suspect bilateral renal parenchymal disease 2. Minimal hematoma is noted after renal biopsy, thickness: 0. 33 cm. Renal biopsy 1. Diffuse segmental endocapillary proliferative and membranous glomerulonephritis, compatible with lupus nephritis, class IV-S(A)+V. 2. Acute tubulointerstitial nephritis.

Neurology p p p EEG: Abnormal awake EEG indicates global cortical dysfunction The NCV of four limbs showed: n Sensorimotor polyneuropathy, but bilateral lumbosacral radiculopathy could not be totally ruled out n Right carpal tunnel syndrome. Consult neurologist n Neurological examination: suspect right hearing impairment, general hyporeflexia n Cognition: JOMAC: 29/30

Cardiovascular and Pulmonary p Cardiac echo: n n n p Mild mitral and tricuspid regurgitation Good LV systolic function(LVEF: 62. 4%) No pericardial effusion CXR: no pleural effusion, no cardiomegaly

Gastroenterology p Abdominal echo n Hepatosplenomegaly n Bilateral renal parenchymal disease n Moderate ascites in the Cul-de sac Ocular p Consult Ophamologist n SLE related retinopathy

Bone marrow smear

Bone marrow biopsy

Diagnosis p p p p 1. Systemic lupus erythematosus 2. Macrophage activation syndrome 3. Lupus nephritis 4. SLE related retinopathy 5. Suspected lupus encephalopathy 6. Vasculitis of ventral fingers, favor SLE related 7. Ichthyosis 8. Suspect right hearing impairment

Renal biopsy BMA: MAS Cefazolin Steroid pulse therapy 1 g QD Prednisolone 1 mg/kg/day Endoxan 1# QD MMF 720 mg BID
")
SLE with Macrophage activation syndrome(MAS)
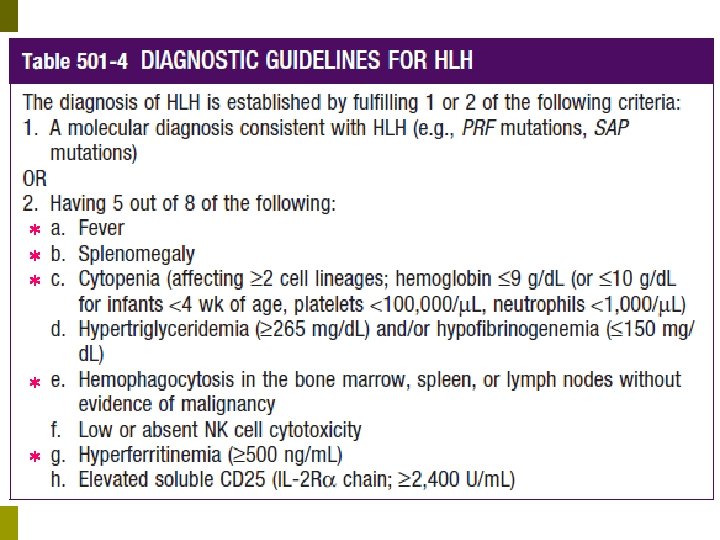
 MAS should be thought of as HLH(Hemophagocytic lymphohistiocytoses) in the setting")
Macrophage activation syndrome(MAS) MAS should be thought of as HLH(Hemophagocytic lymphohistiocytoses) in the setting of a rheumatologic disorder rather than as a separate syndrome. p MAS is used when a hemophagocytic syndrome develops in children with JIA and other rheumatologic conditions. p HLH may develop any time during the course of a rheumatologic disorder (eg, upon presentation, during therapy, in association with a concurrent infection). p

Treatment If a patient with a rheumatologic condition is stable enough to delay HLH-specific therapy, we treat with a course of corticosteroids and/or otherapy for the underlying condition. p For patients with MAS, increased immunosuppression for the underlying rheumatologic disorder is often effective without the need for HLH-specific therapy. p

Thank you for your attentions!
- Slides: 38