Case Presentation M Marjani MD MPH Case 1





























 L(23%) M(3%) Hb: 8. 4 Plt: 158000")
 M(97%) E(1%) RBC:")




- Slides: 48
Case Presentation M. Marjani MD, MPH
Case 1
n 62 y/o Afghan women from Varamin n CC: Chronic cough
Symptoms n n n Fever from 14 days Weight loss (5 kg in 3 m) (BW= 48 Kg) Night sweating Cough & Sputum from 5 years ago Hemoptysis Dyspnea
n PMH: no important problem, no diabetic n No history of close contact with TB case n No history of steroid use
Physical exam n PR: 96 RR: 20 BP: 100/70 OT: 38. 3 n ILL; conscious; a little cachectic; mild distress n Head & neck NL; No LAP; Heart NL n Lungs: crackles mostly Rt side n No organomegaly
Lab n n n WBC: 11000 N: 84 L: 10 M: 5 E: 1 Hgb: 13. 5 MCV: 88 PLT: 479000 ESR: 13 CRP: + Serum ADA: 32 Biochemistry: FBS: 111 Cr: 0. 6 Na: 123 K: 3. 8 Uric acid: 2 ALT: 57 AST: 27 ALP: 277 Bili: 1
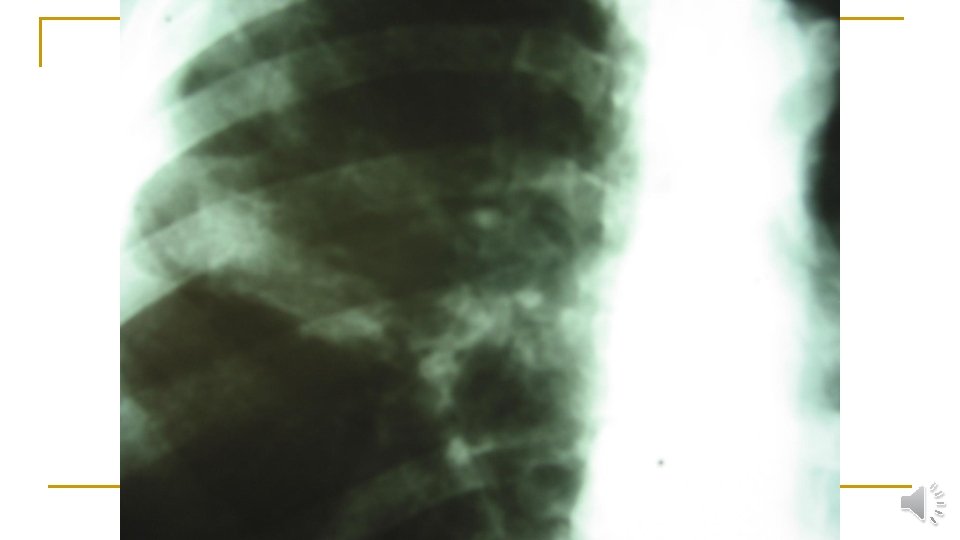
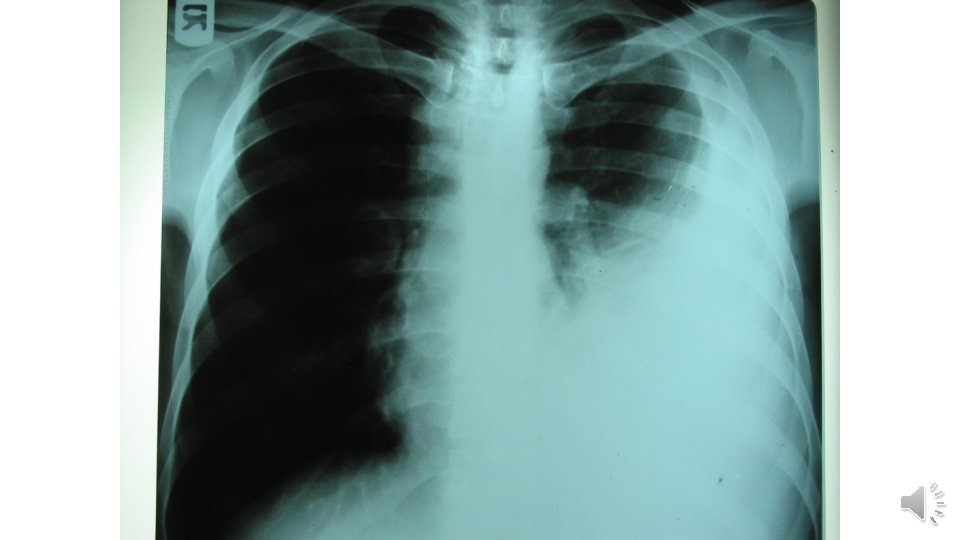
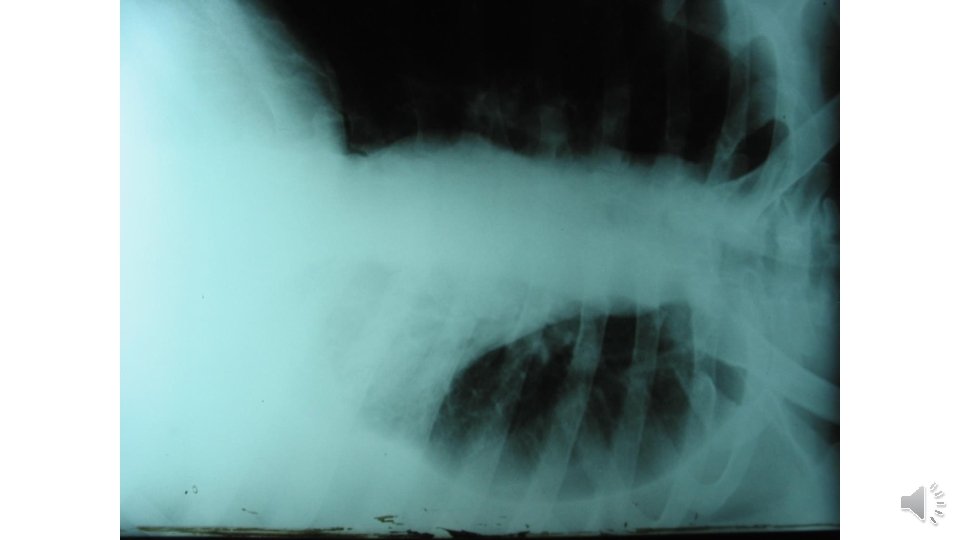
CXR
What your first diagnostic approach
1 st Day n Sputum smear & culture q bacteria & fungi AFB x 3 BK culture q Genxpert q q
Gen-xpert
Differential diagnosis n n n n Mycobacterium Tuberculosis NTMB Nocardiosis Actinomycosis Cryptococcosis Aspergilosis Mucormycosis Histoplasmosis & other endemic fungi
What your next diagnostic approach
Approach to diagnosis • Bronchoscopy and BAL • BAL was sent for • bacteria & fungi • AFB x 3 • BK culture • Cytology • Galactomanan • Genxpert
Quantitation scale recommended by the WHO
Final diagnosis Pulmonary tuberculosis
Patient management • HIV testing • Anti TB initiation • Refer to health clinic • Follow up
Case 2
Case • 33 Y/O man; new case of HIV-HCV co infection • ART naïve • 3 months of cough • PPD: neg
The patient was referred due to: • Fever • Weight loss • Malaise • Sputum For 3 months
Lab tests • ESR: 125 • Hgb: 9. 5 • LFT: Nl • CD 4: 6% = 30 • QFT: indeterminate
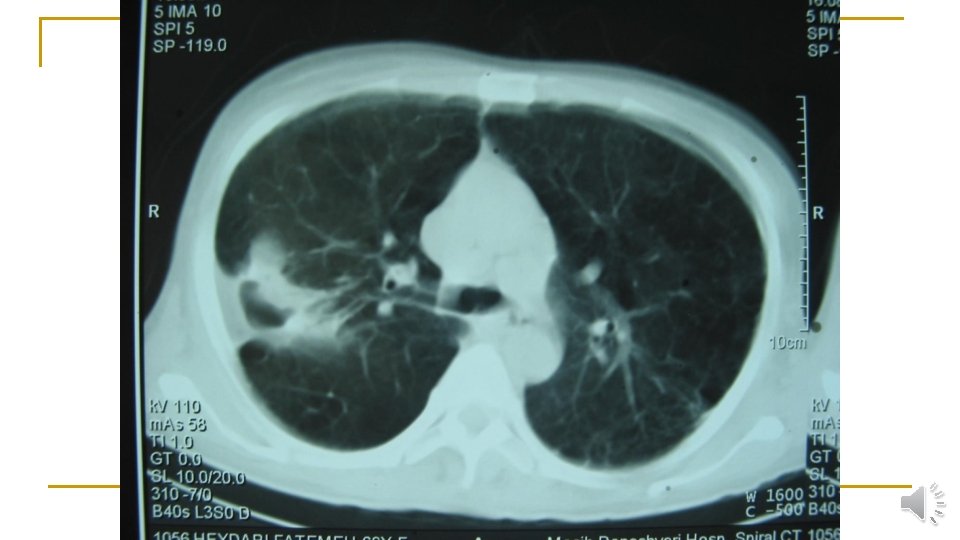
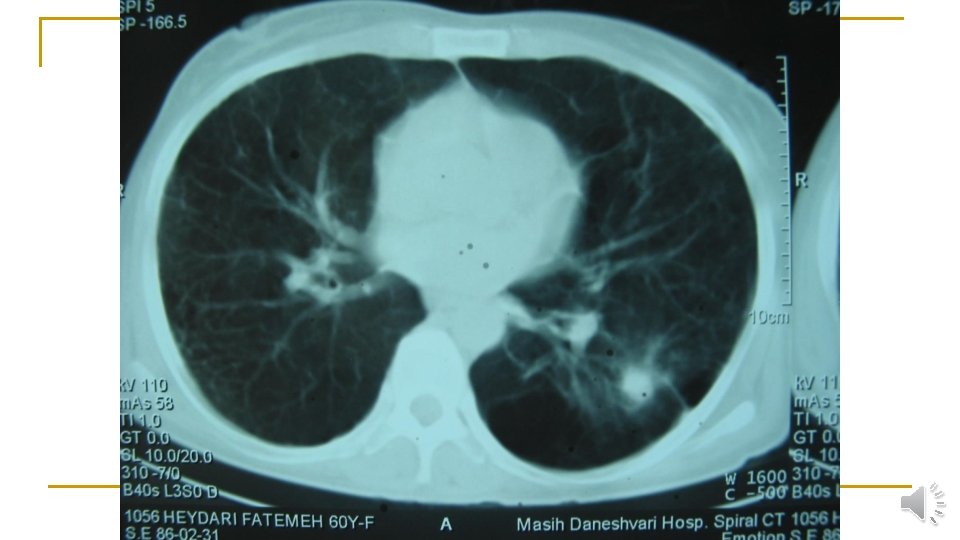
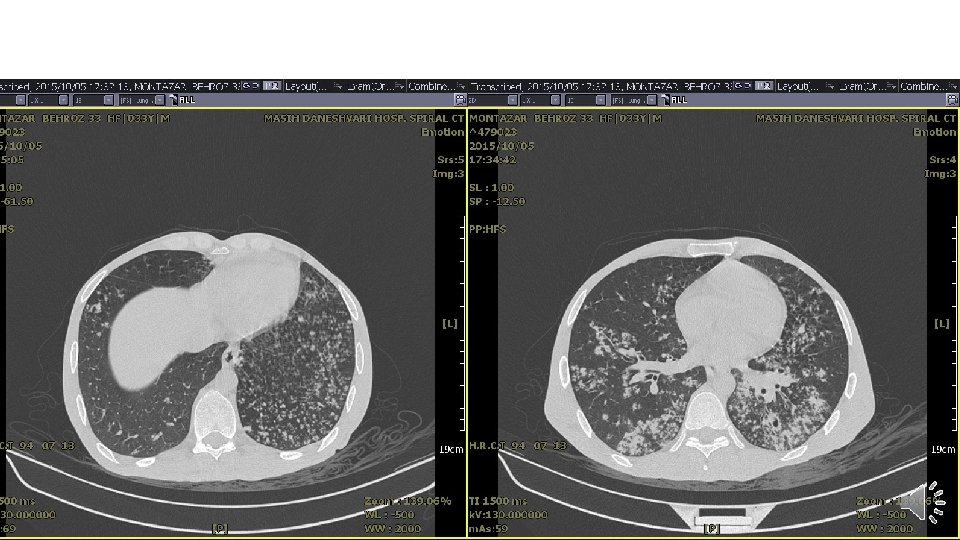
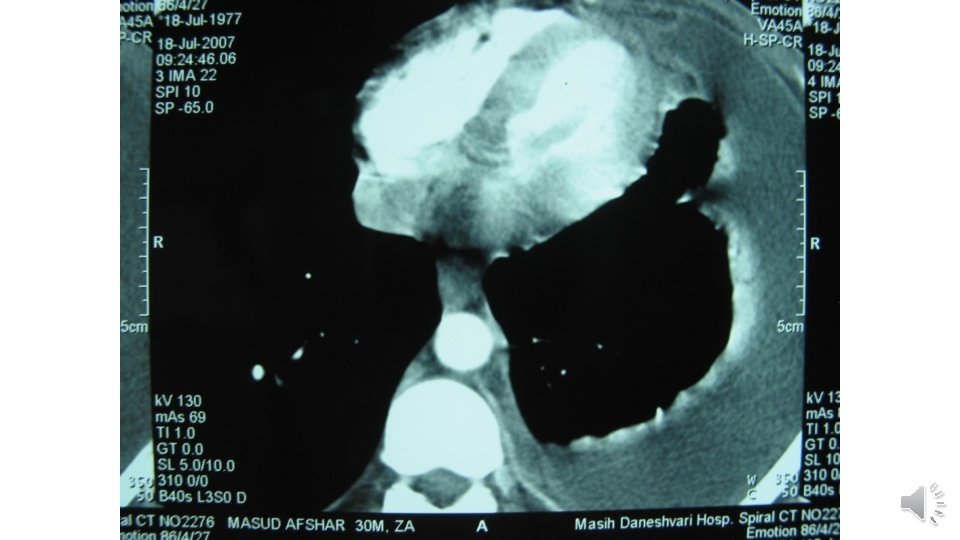
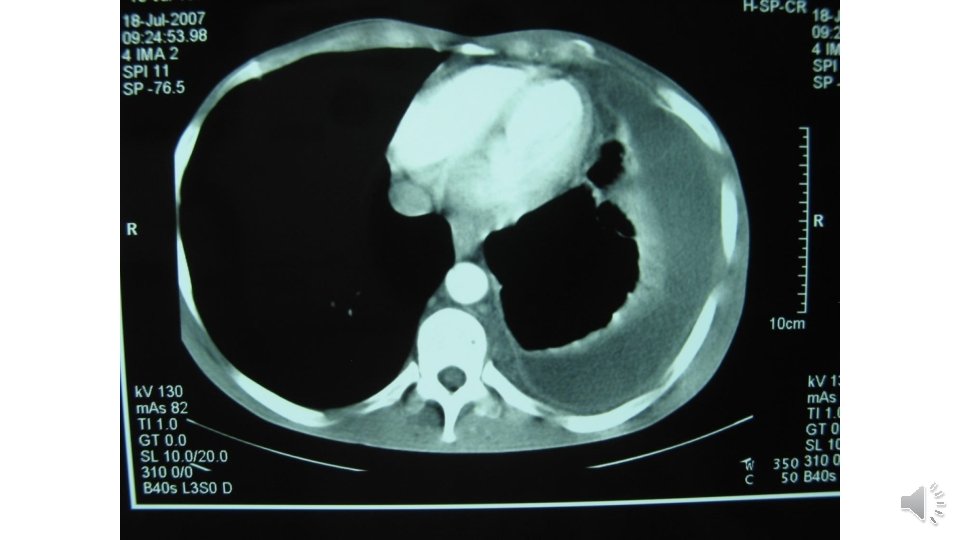
Lung CT scan
Diagnosis and management • Sputum smear for AFB: 3+ • Anti TB was initiated: FDC (HRZE) 3/d • ART (Vonavir) & Cotrimoxazole was continued. Is It enough?
DST
Drug regimen • Anti Tb regimen was changed to: 1. 2. 3. 4. Rifampin Ethambutol Pyrazinamide Levofloxacin 750 mg
Extra pulmonary TB
ﻣﻌﺎیﻨﻪ • • BP: 110/80 PR: 130 OT: 39. 8 RR: 22 Bi temporal Wasting No murmur Decreased left lung sound & dullness No hepatomegaly Splenomegaly O 2 sat: 79%
آﺰﻣﺎیﺸﺎﺕ • • WBC: 1700 P(71%) L(23%) M(3%) Hb: 8. 4 Plt: 158000 LFT: Normal ESR: 60 CRP: neg RF: neg
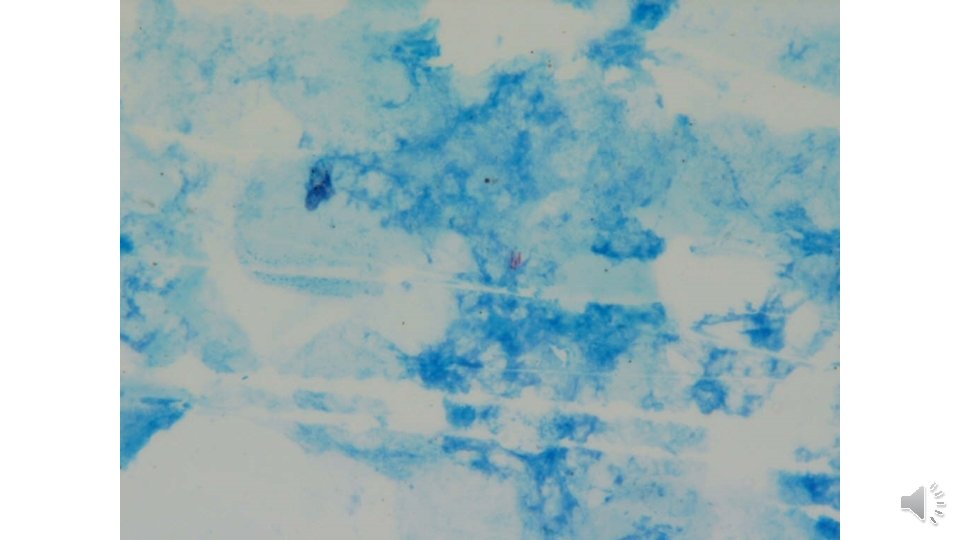
Pleural Fluid • • • PH: 7. 2 WBC: 1400 P(2%) M(97%) E(1%) RBC: 3400 Sugar: 32 Pr: 3. 5 / 5 LDH: 2500 • Smear & culture: neg
TB Spondylitis
Spread of TB spondylitis through the left psoas muscle to the left groin
Psoas abscess tracking down into the left inguinal region