Case Presentation Instructor Presented by Intern June 27

Case Presentation Instructor: 俞芹英醫師、郭雪梨醫師 Presented by Intern 阮昭奎 June. 27 rd, 2006 MRI討論室

Case Presentation • • • Name: 林X杬 Age: 37 y/o Gender: Male Chart number: 03576040 Admission date: 2006. 04. 11 • Chief complaint: Insidious onset and slowly progressive bilateral lower leg weakness for 1. 5 years

Present illness • This 37 y/o male denied any systemic disease before. • One episode of falling down in October, 2004. • Persisted R't flank pain and tightness sensation from then on. • 奇美骨科: X-ray showed no fracture. Treated with analgesics and muscle relaxant, but the symptoms didn't improved. • Besides, bilateral lower leg weakness was noted. • 奇美運動傷害科: R't knee arthroscopy was done but showed negative finding.

Present illness • Our neurology and orthopedic OPD: T-spine MRI showed negative finding. L-spine MRI showed spinal stenosis and compression of bilateral L 4 nerve root. • He ever received physical therapy, but the symptoms didn't improved. In addition, lower leg weakness progressed and he even couldn't walk. • 2006/04: admission.
 •")
Neurological Examination • Left knee Cafe au lait spot (6 x 6 cm) • Right hand intrinsic muscle, forarm, and pectoris major atrophy + weakness 5 5 5 5 5 2+ 0 2 2+ 1 1 3 0 4 3 5 5 ++ ++++ ++++ ↑ • Minipolymyoclnus ++++ ↑ Hoffmann -/+

Upper Limbs
. • Extensor")
Right hand intrinsic muscles: • Extensor pollicis brevis: 4/5 (C 7, 8). • Extensor digitorum: 4 -/5 (C 7, 8). – 以上為radial nerve. • • • Abductor pollicis longus: 4/5 (C 7, 8). Abductor pollicis brevis: 3/5 (C 8, T 1). Opponeus: 4/5 (C 8, T 1). Flexor pollicis brevis: 4/5 (C 8, T 1). Flexor digitorum: 5/5 (C 7, C 8, T 1). – 以上為median nerve

Sensory Function • Pinprick: – Normal, bilaterally symmetric. Except right dorsal hand 9/10. • Joint position sense: – Bilateral big toe decreased (right 1/5; left 1/5 (right/wrong)). • Vibration: Right Left – – Big toe 8 8 Ankle 9 9 Knee 8 8 Wrist 10
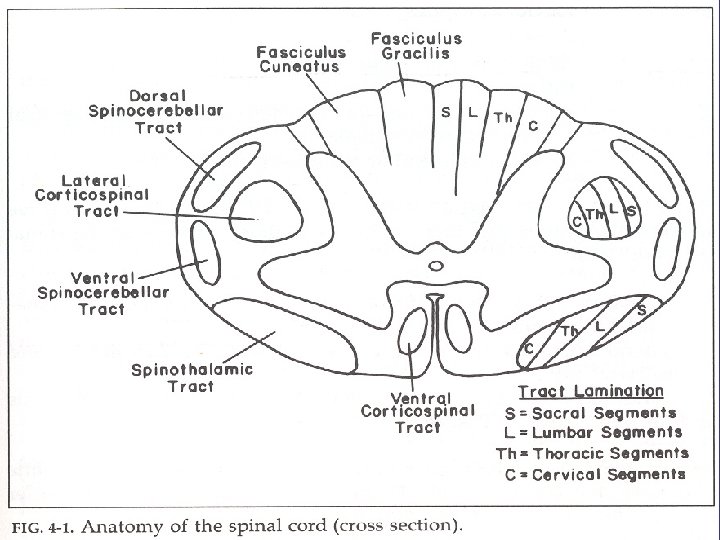

Localization/ Etiology • Intramedullary Lesions • Extramedullary Lesions • Poorly localized burning pain • Radicular pain • A Brown-Séquard hemicord syndrome • Asymmetric lower motor neuron signs in one or two segments • Early corticospinal signs • Marked sacral sensory loss (ascending sensory loss) • Early, prominent CSF abnormalities • Sphincter involvement: relatively late • Sensory dissociation • Sacral sparing • Late and less prominent corticospinal signs • Normal or minimally altered CSF • Sphincter involvement: relatively early
 – Tumor")
Localization/ Etiology • Lower C-cord radiculomyelopathy (C 7, 8 + T 1) – Tumor (extra-medullary) – Traumatic spondylothesis – C-spine HIVD • Survey Result – NCV: severe denervation change of C 8, T 1
 T 2 T 1 F/S+C")
MRI(2006/4/12) T 2 T 1 F/S+C
")
CT(2006/04/27)

• 4/28: C 6 -7 laminectomy + removal of C 6 -7 facet joint + subtotal removal of tumor • Pathology: Neurilemmoma. • Transfer to rehabilitation ward on 5/8.
 T 1 T 1 FSE")
MRI(2006/5/16) T 1 T 1 FSE
 • • • Metastasis 118")
Spinal Tumor • Adults: • Children • Extradural (78%) • • • Metastasis 118 Myeloma 19 Neurofibroma 15 Lymphoma 14 Others 7 • Intraduralextramedullary(18%) • Meningioma 22 • Schwannoma 13 • Others 4 • Metastasis 1 • Lymphoma 1 • Intraduralextramedullary (64%) • Dermoid/Epidermoid 6 • Others 1 • Intramedullary (18%) • Astrocytoma 2 • Intramedullary(4%) In a 2. 7 million population in Glascow • Astrocytoma 8 • Others 1 Adapted from Adams, Graham and Doyle: Brain Biopsy, 1982

Nerve sheath tumors of Spine • 25 percent of intradural extramedullary spinal tumor • 65 percent: schwannomas most of the remainder: neurofibromas • (Schwannoma make up almost one-third of primary spinal neoplasms) • Schwannoma: Schwann cell Neurofibroma: derived from a mixture of Schwann, perineurial, and fibroblastic cells • Schwannomas: sensory components Neurofibroma: motor portions.

Nerve sheath tumors of Spine • Sporadic NSTs: - Most common in the 40 th to 70 th decades - men : women => 1: 1 • NF type 1 - Subcutaneous neurofibromas are characteristic of NF type 1 - 2% of all the NF type 1 patients have neurologic symptoms from a spinal lesion. • NF type 2 - 90% patients with NF-2 had spinal tumors; primarily schwannomas, but including some meningiomas. - 2% spinal schwannomas seen with NF-2; while the rest are sporadic.

Age at diagnosis MATTI T. SEPPÄLÄ. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83: 621– 626, 1995.

Clinical presentation • Slow growing • Fill a significant volume of spinal column before causing symptoms

Diagnosis • Contrast-enhanced MRI is the most sensitive and specific imaging. • Location: - 70 -75% intradural extramedullary - 15% completely extradural - 15% extend through the nerve root sleeve into the epidural space. => “Dumbbell-shaped" tumor - Rare intramedullary - Thoracic> cervical= lumbar • “Dumbbell-shaped" tumor are not pathognomonic for schwannoma and neurofibroma. • The differential diagnosis also includes exophytic meningiomas, lipomas, chordoma, and chondrosarcoma.

“Dumbbell-shaped" tumors By Toyama

Pathology Antoni A Antoni B

Treatment • Surgery is the treatment of choice. • Gross total resection is often curative. However, NSTs are benign and slowgrowing, and function-sparing operations are important. • There is no established role for chemotherapy or for standard radiation therapy in patients with Malignant NSTs.

Surgery • Posterior or postero-lateral approach • Neural monitoring is often used during tumor resection: - Somatosensory evoked potentials - motor evoked potentials - Electromyography - Anal sphincter electrodes - Intraoperative radiographs - Following laminectomy, ultrasound may be used - A biopsy is sent for frozen section • Post-op - Sensory deficits, but well tolerated - Motor deficits are less common - Myelopathy resolves quickly following tumor resection. - Spinal fluid leak is a rare complication. • For patients who are not candidates for surgical resection or in whom only a partial resection is possible, fractionated radiation therapy or stereotactic radiosurgery may be used to treat symptomatic tumors

Prognosis • The goal of treatment - to prevent recurrence or progression - to preserve spinal nerve root function MATTI T. SEPPÄLÄ. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83: 621– 626, 1995.

Prognosis MATTI T. SEPPÄLÄ. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83: 621– 626, 1995.

Prognosis MATTI T. SEPPÄLÄ. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83: 621– 626, 1995.

Reference • Andrew T. Parsa. Spinal cord and intraduralextraparenchymal spinal tumors: current best care practices and strategies. Journal of Neuro-Oncology 69: 291– 318, 2004. • MATTI T. SEPPÄLÄ. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg 83: 621– 626, 1995. • Uptodate: Spinal cord tumors. • Uptodate: Intradural nerve sheath tumors. • Ross and Brant-Zawadzki. Diagnostic imaging: Spine, Part IV, Section I: spinal neoplasms.

Thank you for your listening!
- Slides: 30