Case Presentation and the band played on to

Case Presentation “and the band played on” to the tune of MDR-TB November 24 2006 Marie Turner, M. D. Jo-Ann Keegan, R. N. , M. S. N.

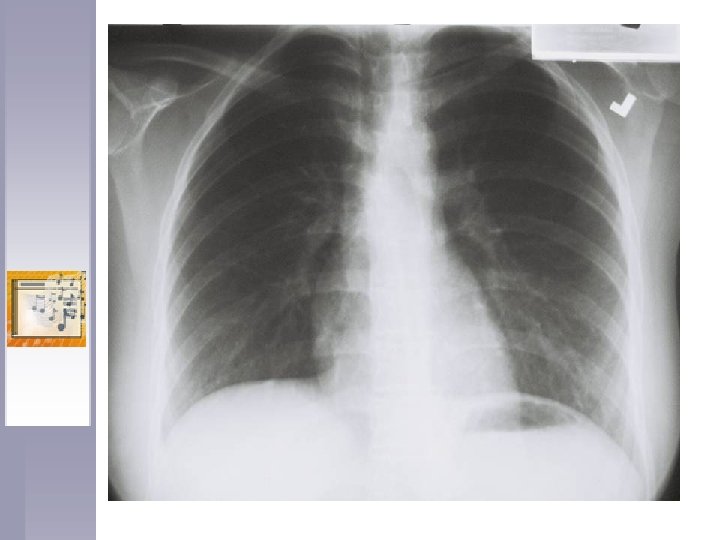
Case Details ♫ 16 y. o. U. S. A. born student in a suburban high school ♫ Played a wind instrument in one of the largest high school bands in the state ♫ Presented with cough, fever, chest pain for more than 1 month duration ♫ CXR: RUL pneumonia TX with Quinolone x 10 days with improvement. CXR 2 weeks later: resolving pneumonia

Case Details ♫ Several weeks later symptoms returned, hospitalized – pneumonia treated with Azithromycin, transferred to a medical center for IV anti-biotics. ♫ DX at Medical CTR. : SM (+), cavitary TB ♫ D/C on 5 drugs INH, RIF, PZA, EMB and Levo. INH resistance suspected


History ♫ Student visited endemic country from age 2 – 11 months ♫ TST positive, CXR negative at age 2 ♫ Treated with INH for 1 year ♫ Sensitivities after 8 weeks treatment: Resistant to INH RIF EMB STREP

History ♫ Treatment guidelines what would you do here? ♫ Treatment § INH changed to 900 mg briefly, then discontinued § EMB and RIF discontinued, PZA continued § LEVO changed to CIPRO then GATI due to joint symptoms § CYCLO and CAPREO added
 8")
Table 1: Treatment Summary for Case Medication Duration Reason to Discontinue Isoniazid (INH) 8 weeks Organism resistant to INH 2 weeks of 900 MG dosages Rifampin (RIF) 6 weeks Organism resistant to RIF Pyrazinamide (PZA) 9 months Elevated liver function tests Asymptomatic with severe hepatitis Ethambutol (EMB) 6 weeks Organism resistant to EMB Levofloxacin (Levo) 1 month Joint symptoms Ciprofloxacin (Cipro) 3 weeks Physician preference – changed to Tequin Gatifloxacin (Tequin) 12 months Treatment completed – (Drug well tolerated) Cycloserine 12 months Treatment completed – (Drug well tolerated) Capreomycin IM 2 months Intensive induction phase completed – Maximum dose PASER 10 months Treatment completed – Drug well tolerated

Identifying and Treating Contacts ♫ Period of infectiousness prior to diagnosis and treatment determined from symptom history ♫ School staff, parents and health care providers interviewed to determine possible school, home, social and work contacts ♫ Contacts classified into risk groups for recent exposure and previous infection ♫ Contacts interviewed to determine previous skin test status

Identifying and Treating Contacts ♫ Band members stratified by instrument type and room position. ♫ Contacts likely infected with MDR TB started on at least 2 drugs based on known susceptibility of the source case isolate. ♫ Medical consultation was from a physician with expertise in MDR TB. ♫ Contacts’ treatment and complication history tracked.

Identifying and Treating Contacts ♫ Patient remained in school while symptomatic for 2 months prior to diagnosis. ♫ Household: 2 of 3 household contacts had positive TST’s, with time of infection undetermined. Dad previous positive TST current CXR WNL, not treated. Mom current TST 25 MM baseline 0 MM TX with INH 900 mg twice weekly. TX options Boosting ? Conversion ? Sibling 13 y. o. (-) TST, (-) CXR (no window prophylaxis) ♫ School: 264 students and teacher contacts identified 250 (95%) completed TST’s and CXR’s.
 were TST positive. §")
Identifying and Treating Contacts ♫ School: 7 of 250 (3%) were TST positive. § § § All 7 were in close physical proximity to the case 5/7 played a wind instrument in the band 2/7 were in close proximity in the classroom 4/7 had documented TST conversions All 7 had no known risk factors for previous exposure and were presumed to be newly infected with MDR TB. Drug treatment for school contacts: • Treatment with 2 drugs to which organism sensitive (PZA, LEVO) • Joint symptoms in 1 adult and 3 students were resolved after TEQUIN substituted for LEVO
 § One student")
Identify and Treating Contacts ♫ Drug treatment for school contacts: (continued) § One student developed drug induced hepatitis toxicity § Directly observed therapy was refused by parents but parents agreed to supervise meds § Adolescents under reported adverse reactions to avoid serologic testing ♫ Table 2 summarizes drugs and treatment of MDR Latent Infection.

Table 2: School Converters – Treatment Summary for MDR Latent Infection Patient Exposure Type PPD Size Drugs Complications Drug Change Disposition #1 Teacher 25 mm PZA, Levo Uric acid elevated (11. 1) PZA, Tequin Completed Rx #2 Band 10 mm PZA, Levo Uric acid elevated PZA, Tequin Completed Rx #3 Band 15 mm PZA, Levo Uric acid elevated (8. 2) PZA, Tequin Completed Rx #4 Band 10 mm PZA, Levo None Completed Rx #5 Classroo m 15 mm PZA, Levo None Completed Rx #6 Band 12 mm PZA, Levo Foot and joint pain with no elevation of Uric acid PZA, Tequin Completed Rx #7 Band 18 mm PZA, Levo Admitted with acute liver failure and listed for a liver transplant until liver functions improved All TB drugs discontinued Unable to complete Rx

OTHER ISSUES ♫ Student did not return to school until nearly 2 months after diagnosis ♫ Culture conversion occurred over nine weeks after initial treatment started ♫ Student was not allowed to return to the same high school she was attending (with 6 weeks left to the school year) ♫ Fear and stigma of the disease extended to the school administration ♫ School nurse was threatened, to induce her to reveal the students identity, she refused caller

Conclusions - Discussion ¯Contacts treated with second line drugs for MDR latent TB infection had clinically significant variations in adverse reactions to quinolones ¯Source case transmission of MDR TB was extended by missed diagnosis and subsequent treatment with a quinolone for suspected community acquired pneumonia

Conclusions - Discussion ¯Patient and family education regarding the importance of stopping medications, if adverse reactions suspected, is vital to health and treatment outcome ¯Contacts treated with second line drugs for MDR TB require close monitoring, including serologic testing and DOT.

Conclusions - Discussion ¯Directly Observed Therapy of MDR TB contacts would likely enhance clinical followup. Although parents refused this option, more education and a comprehensive effort on the part of all providers would most likely be needed to reverse this decision. Another benefit of DOT is the possible prevention of further drug resistance. ¯Further research is necessary to address the complexities and duration of treatment for MDR latent TB infection.
- Slides: 18