Case presentation 980505 Presented by Intern Patient profile

小港內科 Case presentation 98/05/05 Presented by Intern : 吳勝騰

小港內科 Patient profile £ Name: 辜O雄 £ Chart number: 00555960 £ Age : 74 -year-old £ Gender: male £ Date of admission: 98/4/23

小港內科 Chief complaint £ Fever up to 39’C with chills was noted in this morning. (4/23)

小港內科 £ Present illness This 74 y/o male is a case of – £ £ Diabetes mellitus was diagnosed 5 years ago, under oral anti-diabetic medication control. Last month, he was admitted for jaundice. Decreased appetite and loss of body weight (2 kg within 2 weeks ) were noted then. The patient also complained of tea colored urine and clay colored stool. Associated symptoms and signs last month included: – – fever (-), chills (-), fatigue(+) mental disturbance or behavior change (-), general weakness (+), insomnia(-) RUQ tenderness(-), hunger pain (-), post prandial pain (+), diarrhea (-), nausea (-), vomiting (-) , tarry stool(-), bloody stool(-) Yellowing of the skin(+), itching of the skin(+)

小港內科 £ During Present illness last admission, a series of examinations were performed, and the laboratory data and image survey indicated the possibility of an obstructive leision involved his biliary tract. £ Under the impression of obstructive jaundice, she received ERBD insertion on 4/9 for symptom relief.
 =7.")
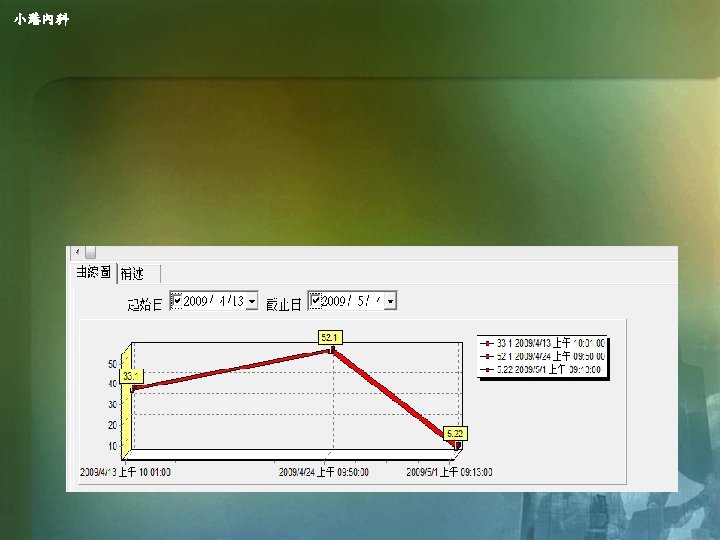
小港內科 Clinical course 4/09 Jaundice. Decreased appetite. Loss of body weight. Bil (T/D) =7. 50/4. 01 WBC= 5290 ALP = 1463 CA 199=180. 65 r-GT = 1504 Arrange ERCP , ERBD was inserted Unasyn 1 vial Q 6 H prophylatic for ascending cholangitis 4/10 4/12 4/14 4/16 Arrange abdominal echo, Lipase=1837. 9 Bil (T/D) =4. 85/2. 47 CRP = 6. 4 Fever up to 39. 1, B/C x 2 , Arrange MRCP Unasyn used day 5 Discharged form our ward.

小港內科 Present illness However, after discharged from our ward, fever up to 39’C attacked him again with chills on 4/23, and his family brought him to our ER for help. £ Associated symptoms and signs included: £ – – fever & chills(+), weakness (+), fatigue(+), rhinorrhea(), sore throat(-), nasal obstruction(-), intermittent cough with mild sputum(-), abdominal pain(-), nausea(-), vomiting(-) , bowel habit change(-), pain, tarry stool(-), bloody stool(-), clay color stool(-) urinary frequecny(-), burnning sensation(-), dysurea(-) Yellowing of the skin(-), itching of the skin(-)

小港內科 Clinical course £ Under the impression of recurrent biliary tract infective episode, he was admitted again, and received antibiotic therapy.

小港內科 • • Diabetic mellitus: mellitus diagnosed 5 years ago, under oral anti -diabetic medication control (Diamicron 1# bid AC). Hypertension with medication control since 民國 94 年 • • Olmetec 0. 5# OM, Capoten 1# PRN Hepatitis non B, non C diagnosed on 民國92年 • • Past history HBV/HCV: HBs. Ag(-), Anti-HCV(-) (92. 09. 12) Alcohol/Smoking(+/+): now quit for 20 yrs Duodenal ulcer history(+) Gouty arthritis: arthritis diagnosed on 民國88年 Hyperlipidemia (+) Operation history: denied Allergy history: pyrine

小港內科 Family history Not contributory
 � 1 * BID AC *")
小港內科 £ £ £ Current medicine Diamicron MR(●) � 1 * BID AC * 28 D� Olmetec � 0. 5 * OM * 28 D� Strocain(息痛佳音錠) � 1 * TID PC * 14 D� Nidolium � 1 * TID PC * 14 D� Suwell � 1 * TID PC * 14 D� Denied of Chinese herb use , medication for gouty atritis, and other drug exposure.
 Vital sign: BP: 100/55 mm. Hg, PR:")
小港內科 • Physical examination on ER (4/23) Vital sign: BP: 100/55 mm. Hg, PR: 94 bpm, RR: 22 cpm, BT: 39. 1 ℃ • • • General Appearance: Consciousness: alert (E 4 V 5 M 6) Conjunctivae: not pale ; Sclera: not icteric Neck:Supple, no palpable mass – – – no jugular vein engorgement no goiter No lymphadenopathy
 Chest:Symmetric expansion – BS: clear, no wheezing")
小港內科 • • • Physical examination (4/23) Chest:Symmetric expansion – BS: clear, no wheezing or crackles • • Inspection : mild distended Palpation Heart:Regular heart beats without audible murmur Abdomen: • • Soft, Tender (+) RUQ, Guarding(-), Rebounding pain (+/-) Liver / Spleen: -/- Percussion : tympanic(-), Shifting dullness(-) Auscultation : Normoactive bowel sound Extremities and skin: – – Pitting edema (-) Freely movable
")
小港內科 Lab data on 4/23 (ER)
")
小港內科 Lab data on 4/23 (ER)

小港內科 Urine routine examination

小港內科 Stool routine examination

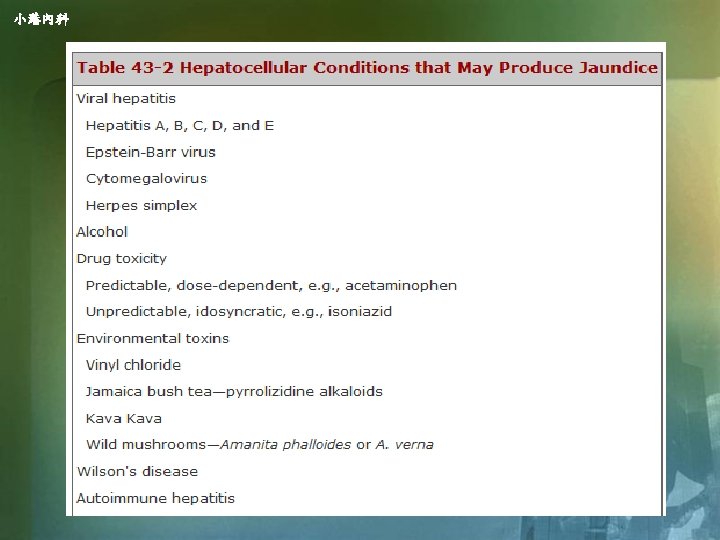
小港內科 Tentative diagnosis on 4/23 £ Suspect recurrent biliary tract infection £ Obstructive Jaundice post endoscopic retrograde biliary drainage (98. 4. 9) , £ Suspect early stage of ampulla vater tumor. £ Diabestes mellitus, type 2 £ Hypertension £ Hepatitis

小港內科 £ Under Clinical course the impression of recurrent biliary tract infective episode, he was admitted again, and received antibiotic therapy. £ We arranged abdominal echo on 4/25 in comparison of prior image on 4/10. £ For his condition is stable, and meet the indication of biliary surgery, he was discharged and went to KHCG for surgical intervention.

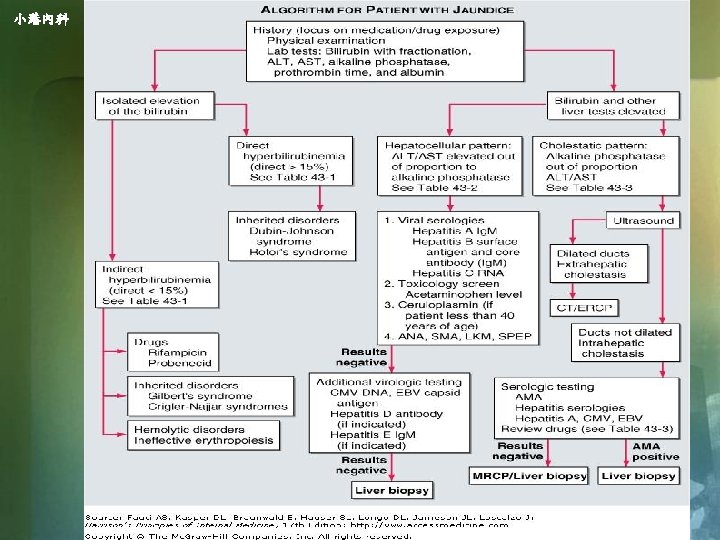
小港內科 Hyperbilirubinemia

小港內科 £ £ Hyperbilirubinemia The presence of scleral icterus indicates a serum bilirubin of at least 51 mol/L (3. 0 mg/d. L). The bilirubin present in serum represents a balance between input from production of bilirubin and hepatic/biliary removal of the pigment. Hyperbilirubinemia may result from – – – (1) overproduction of bilirubin (2) impaired uptake, conjugation, or excretion of bilirubin (3) regurgitation of unconjugated or conjugated bilirubin from damaged hepatocytes or bile ducts.

小港內科 Bilirubin metabolism

小港內科 £ Thank you very much!

小港內科 Lab data on 4/9

小港內科 Lab data on 4/9

小港內科 Blood culture on 4/12



- Slides: 36