CASE of POSTINFARCT VSD History and Physical Exam









 • Epidemiology • • • Pre-Reperfusion Era • Incidence 1")

- Slides: 16
CASE of POST-INFARCT VSD
History and Physical Exam 68 year old male presented to Outside Hospital with stuttering CP x 2 -3 days followed by persistent CP for 5 hours with an “uneasy feeling” – 1 month prior Inferior STEMI with RV involvement No PMHx/PSHx/Medications/Allergies/no smoking Reported VS: BP 97/64 P 118 R 16 Exam loud systolic murmur with S 3 gallop
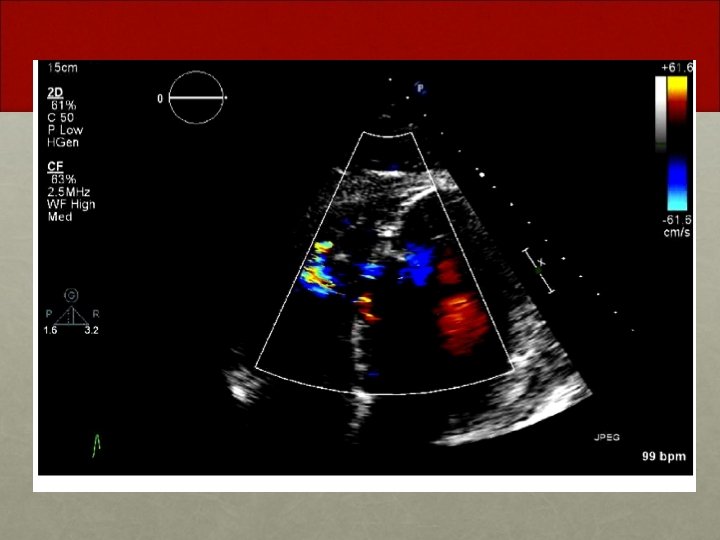
Intervention Outside Hospital one month prior • Bedside TTE with 7 mm VSD + dilated RV • Lesion: 100% occlusion of proximal RCA • Anticoagulation: Heparin • Intervention: PTCA + Aspiration Thrombectomy • BMW wire. 2 x 12 mm Balloon • Coronary Spasm improved with NTG • Residual lesion 70% • Ventriculogram: • Hyperdynamic LV with normal EF • Large RV • Large VSD L-> R shunt • IABP placed • PASP 40 mm Hg, PCWP 14 mm Hg, PA saturations 82 -87%
Follow Up Course over subsequent month • Same day, post-PTCA, taken for emergent CABG (SVG -> PDA) + VSD Patch • Following day returned to OR for washout. Minimal bleeding. Worsening Right Heart Failure • Transferred to tertiary center the following day • RVAD placed Day 5 • Despite RVAD, continued progressive RV Failure, Liver Failure, Renal Failure • CRRT • Trached • IABP • IV Pressor support
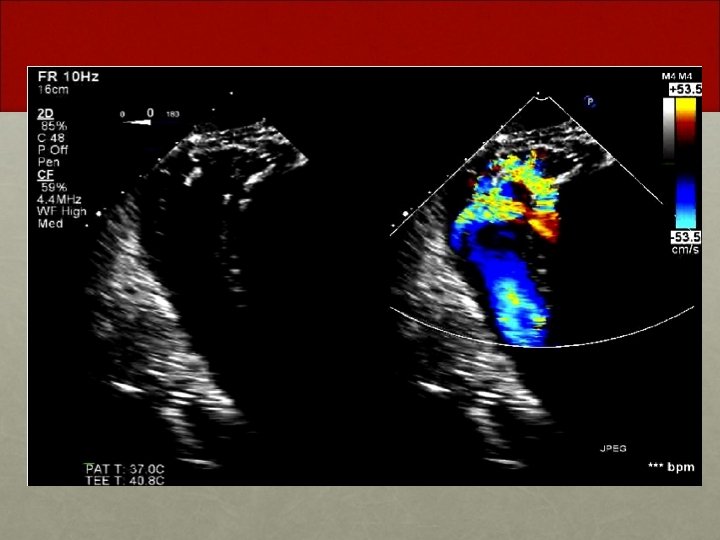
Follow Up One month later • Patient found to have residual VSD despite VSD patch repair post-infarct • Patient brought to the cardiac catheterization suite for possible percutaneous VSD closure
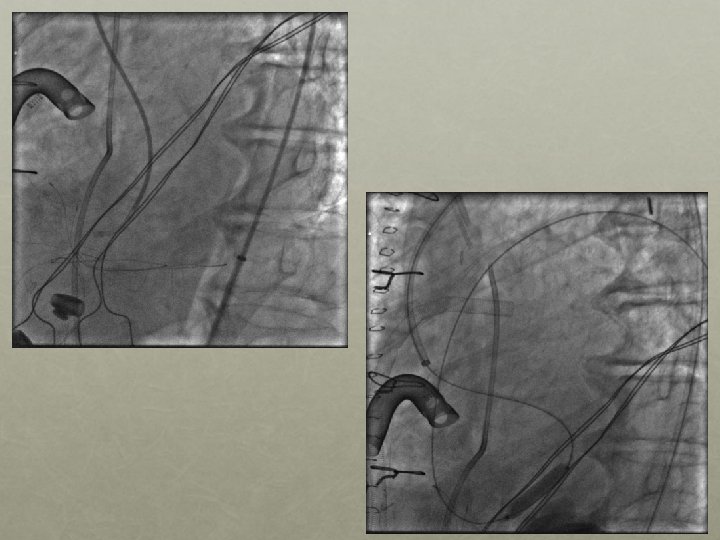
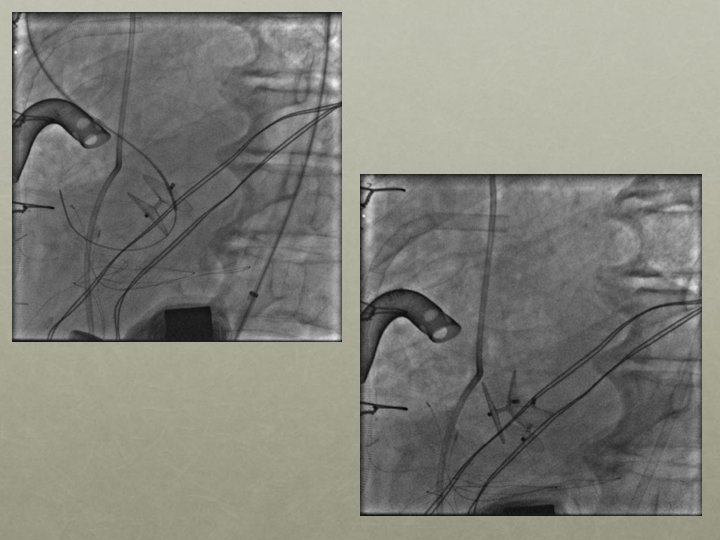
Amplatzer 25 mm Cribiform Septal Occluder
Significant Residual shunt
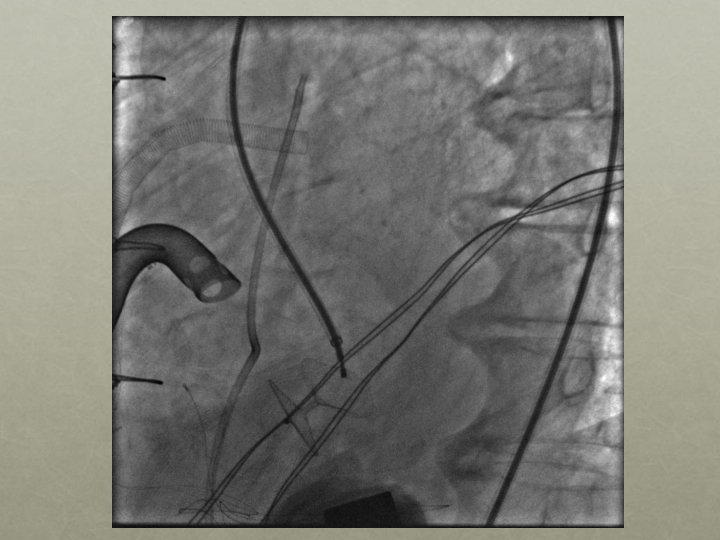
2 nd Septal Occluder Device Deployed
Catheterization Hemodynamics RA 10 RV 44/11 PA 38/13 mean 22 Ao 129/76 Saturations Baseline PA 91% After Occluders PA 83% Following Day PA 76%
Ventricular Septal Rupture (VSR) • Epidemiology • • • Pre-Reperfusion Era • Incidence 1 -3% • In-hospital mortality 45% surgically treated • In-hospital mortality 90% medically treated Thrombolytic Era • Incidence 0. 2 -0. 6% (dependent on study) • 30 d mortality 47% surgically treated • 30 d mortality 94% medically treated Primary PCI Era • Incidence 0. 17%, 0. 23%, 0. 25%, 0. 28% • In-hospital mortality 38. 7% surgically treated • In-hospital mortality 100% medically treated • Incidence has decreased with early revascularization • Extremely high mortality without definitive repair/closure • High mortality despite definitive repair/closure Crenshaw et al. Circ 2000 Moreyra et al. AJC 2010
Percutaneous vs. Surgical Closure • High morbidity & mortality with immediate surgical closure • More complex then congenital VSDs (tissue friable, geometry, multiple holes, expansion of original rupture) • “Bridge” v definitive treatment • Defect <1. 5 cm, subacute stage, poor surgical candidate Percutaneous closure