Case Malnutrition Iron Deficiency Anemia StatusPost Duodenal Switch















 • Blood transfusion • IVF for dehydration • IV iron")








. Retrieved December 29,")
- Slides: 26
Case: Malnutrition & Iron Deficiency Anemia Status/Post Duodenal Switch & Ileostomy Christa Giroux, Dietetic Intern
Overview • Patient’s history • Normal anatomy of GI tract • Present medical status & typical treatments • Lab values • Medications • Present treatment • MNT • Prognosis
Introduction • Patient initials: S. M. • 40 y/o female • 5’ 7”, 89 lbs, BMI= 13. 2 • ED admit 12/11/16 • Several falls, generalized weakness • Observation bed • Discharged on 12/12/16
Past Medical Hx • Iron deficiency anemia • Protein-energy malnutrition • 8% weight loss 2 months • Opioid dependence • S/p duodenal switch surgery (BPD/DS) • IBD • S/p total colectomy with ileostomy • With high output • Lumbar disc degeneration • Bilateral pleural effusion • Spinal stenosis
Reason for Patient Choice • BPD/DS • Ileostomy • Presence of malnutrition in relation to bariatric surgery • Multiple health complications that are related
Social Hx • Unemployed w/ disability status • Divorced, no children • Lives at home w/ mother (breast CA) • Responsibilities: cooking, laundry, other house chores • Adequate standards of living, but not ideal- lack of income • Medicare • Religion not recorded
Normal anatomy & physiology of GI tract • Absorb nutrients, convert food to energy, dispose waste. • Stomach: chemical + mechanical digestion • Gallbladder: bile reservoir; aids with digestion by secreting bile acids into the small intestine • Pancreas: secretes enzymes into small intestine • Small intestine: most digestion & absorption done • Liver: detoxification; processes nutrients from small intestine • Colon: passes stool from digestion to the rectum; can also
Closer Look at Small Intestine • Duodenum: • iron, zinc, magnesium, copper, fat soluble vitamins, calcium, phosphorus, some B-vitamins, folate • Jejunum: • lipids, amino acids, monosaccharides, small peptides, B-complex vitamins, vitamin C, chromium, manganese • Can also absorb same nutrients as duodenum, but less efficient • Ileum: • bile salts, fluids, vitamin K, Vitamin D, vitamin-B 12 intrinsic factor complex
Prior Admissions/Hx • Medication refills, transfusions, lab testing • Several GI endoscopies • Back complications • 2005 - BPD/DS done since the pt was morbidly obese • 2007 - Total colectomy w/ ileostomy for IBD & severe dumping syndrome • 2015 - Episode of TPN d/t inability to eat & absorption issues. Thoracentesis & R chest tube placed for pleural effusion • Several other admissions for back pain, GI bleeds, abdominal pain, weakness. • Sees digestive specialist in Springboro, OH
Present Medical Status & Tx • BPD/DS: combination of gastric bypass + sleeve gastrectomy • https: //www. youtube. com/watch? v=p. WW 2 sw. Ea. Hr. Q • 85% stomach removal & duodenal resection • PROS: Significant weight loss • alters gut hormones, restricts absorption, limits consumption, reduces absorption of fat by 70% • CONS: Adverse side effects • Nutrient deficiencies, higher mortality, malnutrition, nausea, vomiting. • Success requires compliance with dietary restrictions, supplementation, physician visits
Present Medical Status & Tx • Total colectomy w/ileostomy: permanent tx for dumping syndrome • Ileum brought through abdominal wall • Colon, rectum, anus removed • Ostomy bag • High ostomy output: • >8 cups per day indicates malnutrition & dehydration • Treatment: Management w/ medication, soluble fiber, protein, several small meals per day
Present Medical Status & Tx • Iron deficiency anemia: • Common in all bariatric surgery patients • Duodenum primary absorption site • Treatment: Aggressive iron supplementation, include ironrich foods in diet, vitamin C • Hypocalcemia: • • Common with BPD/DS Duodenum primary absorption site Opioid dependence can inhibit calcium absorption Treatment: oral calcium supplementation
Present Medical Status & Tx • Malnutrition: • Common after BPD/DS • Poor absorption, restriction, gut hormones • Treatment: +500 kcal/day for 1 lb weight gain/week • Small, frequent meals • Calorie dense food items • Long term TPN or TF in context of malabsorption
The Literature • Randomized parallel-group trial of 58 participants: • Participants completed gastric bypass or BPD/DS • Malnutrition only seen in BPD/DS patients • Prospective study on all bariatric surgeries: • Iron deficiency anemia in 42. 9% BPD/DS patients within 30 months • 49. 9% with iron deficiency anemia within 60 months • Retrospective review of BPD/DS patients (1999 -2011): • 37% of patients needed further surgery d/t side effects
Medications
Tx (Medical & Surgical) • Blood transfusion • IVF for dehydration • IV iron sucrose • Opioid cessation by physician • Switched to Fergon at discharge, noncompliant w/ previous iron medication • Oral nutrition supplements with coupons • No surgical interventions at this admission
MNT • Patient interview: • • • 5 meals/day N/V Disliked meat Iron pills “hard to crush” Frozen meals & out to eat often Avoids high-fat foods (ostomy) Chicken broth + soups High ostomy output 8% wt loss in 2 months Empties ostomy bag 15 x/day • Diet in hospital: • • Regular Ate 100% of most meals Unjury chicken broth TID Ensure plus BID
24 -hr recall
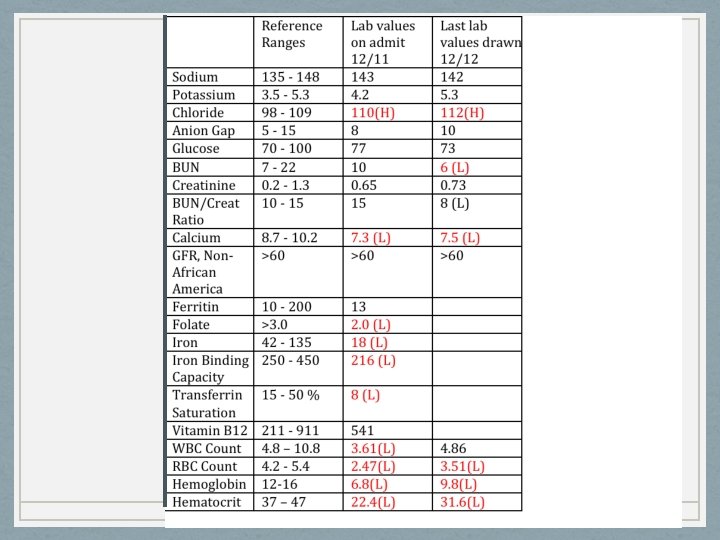
Nutrition-Related Problems & Evidence • Malnutrition • Visible muscle wasting, fat store loss, weight loss, poor intake • Altered nutrition-related lab values: • Iron • Calcium • H&H • Underweight • BMI • Inadequate intake • Weight loss • Per patient • Undesirable food choices • Per 24 -hr recall • Per patient
Nutrient Needs • Malnourished with absorptive issues- increased needs • Kcals: 35 -38 g/kg/day • 1415 -1530 kcal/day • Protein: 1. 4 -1. 5 g/kg/day • 55 -60 g PRO/day
Micronutrient Supplementation • 18 -27 mg elemental iron/day • 1800 -2400 mg calcium citrate (not at same time as iron) • B 12 vitamin supplement 350 -500 mcg • High potency-multivitamin that provides 100% DV of vitamins & minerals each day • Vitamins A, D, K
Nutrition-related recommendations • Increased kcal + protein intake • Calorically dense foodssupplement coupons given • Compliance with iron supplements • Small meals/snacks throughout the day • Hydration • Increased vegetable & fruit intake • Avoiding foods that would affect ileostomy: • • • Sugary foods Carbonation High-fat foods Caffeine Alcohol • Foods high in pectin • To slow down ostomy output
Prognosis • Fair, secondary to hx of noncompliance • Several issues r/t duodenal switch • Adherence to nutrition-related recommendations, compliance with supplements & lower intake of opioids • Patient can improve current state of health
Conclusion • BPD/DS successful for some, but has potential to cause major side effects. • Malnutrition difficult to reverse when normal absorption function is altered • Compliance is important for patients with any GI surgeries or alterations • RD role is vital in patients before & after bariatric surgery, ostomies, or other GI surgeries • Education process important to avoid adverse conditions
References • • • • Digestive System Function & Organs. (2013). Retrieved December 29, 2016, from http: //my. clevelandclinic. org/health/articles/the-structure-and-function-of-the-digestive-system. Stephenson, T. J. , MS, RD, LD. (2015, September). The Digestive System. Lecture presented at Advanced Nutrition Course at University of Kentucky, Lexington, Kentucky. Mahan, K. , Escott-Stump, S. , & Raymond, J. L. (2012). Krause's Food and the Nutrition Care Process (13 th ed. ). St. Louis, MO: Elsevier. Your Digestive System and How It Works. (2013, September). Retrieved December 29, 2016, from https: //www. niddk. nih. gov/health-information/health-topics/Anatomy/your-digestive-system/Pages/anatomy. aspx. Escott-Stump, S. (2012). Nutrition and diagnosis-related care. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. Duodenal Switch (DS). (2014). Retrieved January 09, 2017, from http: //www. cpmc. org/advanced/obesity/ds. html. Nabipour, S. , Said, M. A. , & Habil, M. H. (2014, August). Burden and Nutritional Deficiencies in Opiate Addiction- Systematic Review Article. Retrieved January 09, 2017, from https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC 4411899/. BPD/DS Weight-Loss Surgery - Hopkins Medicine. (n. d. ). Retrieved January 9, 2017, from http: //www. hopkinsmedicine. org/healthlibrary/test_procedures/gastroenterology/bpdds_weight-loss_surgery_135, 64/. Bariatric Surgery Procedures - ASMBS. (2017). Retrieved January 09, 2017, from https: //asmbs. org/patients/bariatric-surgery -procedures#bpd. Long-term outcomes after biliopancreatic diversion with. . . (2016). Retrieved January 9, 2017, from http: //www. soard. org/article/S 1550 -7289(16)00096 -4/abstract. Ostomy Information. (2017). Retrieved January 09, 2017, from http: //www. ostomy. org/Ostomy_Information. html#ileostomy. Ostomy; What to eat and drink when you have a high output. . . (2009, November). Retrieved January 9, 2017, from http: //www. hamiltonhealthsciences. ca/documents/Patient%20 Education/High. Output. Ostomy. What. To. Eat-trh. pdf. Jáuregui-Lobera, I. (2013, May). Iron Deficiency and Bariatric Surgery. Retrieved January 09, 2017, from https: //www. ncbi. nlm. nih. gov/pmc/articles/PMC 3708339/. Post-Gastrectomy Syndrome Symptoms. (2017). Retrieved January 09, 2017, from http: //my. clevelandclinic. org/health/articles/post-gastrectomy-syndrome-overview. Sovik, T. T. (2011, September 6). Weight Loss, Cardiovascular Risk Factors, and Quality of Life After Gastric Bypass and Duodenal Switch: A Randomized Trial. Retrieved January 9, 2017, from http: //annals. org. ezproxy. uky. edu/aim/article/747095/weight-loss-cardiovascular-risk-factors-quality-life-after-gastricbypass.