Case Discussion Burkitts Lymphoma with Central Nervous System

Case Discussion Burkitt’s Lymphoma with Central Nervous System Relapse 指導醫師: VS 蘇裕傑醫師 實習醫師: Intern 傅斯誠醫師 2005/11/05

Patient Data 盧 先生 19 year-old male ID: I 100150062 Admission date: 2005/10/12 Chief Complaint:

Patient Data 盧 先生 19 year-old male ID: I 100150062 Admission date: 2005/10/12 Chief Complaint: Bilateral leg weakness and numbness For 1 day

Past History 2005/01 Burkitt’s lymphoma Completed 10 courses of chemotherapy

Present Illness 2005/01 Abdominal fullness and poor appetite Hospitalized at 台南市立醫院 Gastric ulcer and ascites

Present Illness 2005/01 Abdominal fullness and poor appetite Hospitalized at 台南市立醫院 Gastric ulcer and ascites Transferred to 嘉義基督教醫院 Abdominal Imaging revealed masses Suspect intra-abdominal lymphoma

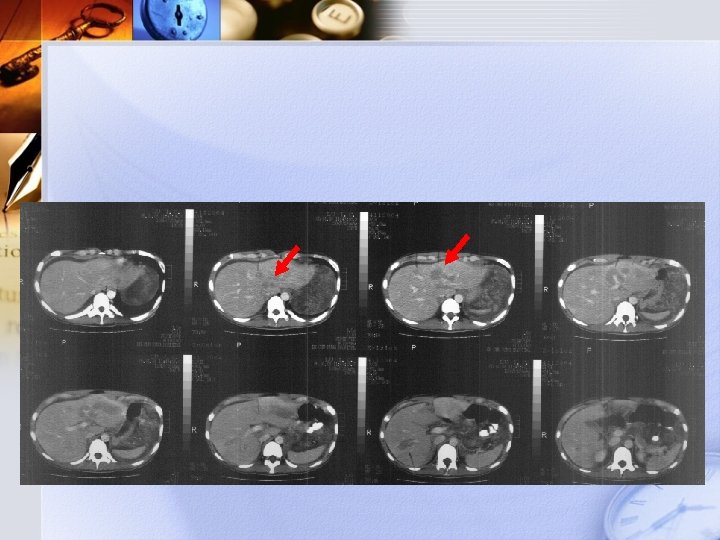
Transferred to 台北恩主公醫院 CT-guide biopsy for diagnosis Burkitt’s lymphoma Liver metastasis

Transferred to 台北恩主公醫院 CT-guide biopsy for diagnosis Burkitt’s lymphoma Liver metastasis Transferred to 台大醫院 Port-A insertion and Chemotherapy

Transferred to 台北恩主公醫院 CT-guide biopsy for diagnosis Burkitt’s lymphoma Liver metastasis Transferred to 台大醫院 Port-A insertion and Chemotherapy Transferred to 大林慈濟醫院 Completed 10 courses of chemotherapy (2005/01/14 ~ 2005/09/23)

2005/01/14 Abdominal CT

2005/01/17 Bone scan No bony lesions

2005/01/18 Gallium scan

Diagnosis Intra-abdominal origin Burkitt’s lymphoma Liver metastases
 High dose")
Diagnosis Intra-abdominal origin Burkitt’s lymphoma Liver metastases Chemotherapy regimen: EPOCH (x 2) High dose MTX + LV + Ara-C Endoxan + Mesna + Oncovin + Epirubicin (x 4) + IT Methotrexate and Ara-C
 High dose")
Diagnosis Intra-abdominal origin Burkitt’s lymphoma Liver metastases Chemotherapy regimen: EPOCH (x 2) High dose MTX + LV + Ara-C Endoxan + Mesna + Oncovin + Epirubicin (x 4) + IT Methotrexate and Ara-C Completed on 2005/09/23

2005/10/11 15: 00 Came to our Emergency Dept. Chief complaint: General weakness Dizziness Dyspnea
 Given K+ supplement Allowed discharge")
At our ER… Lab data revealed hypokalemia (K+2. 8) Given K+ supplement Allowed discharge

2005/10/12 08: 00 Returned to our Emergency Dept. Bilateral lower leg weakness, numbness Drooped right face Diplopia Stool Incontinence

Social History No smoking, betel nut, or alcohol use Lives at home with family

Family History No family member with tumor history. Allergy No known allergies

Physical Examination Weight: 58 kg Vital signs: Height: 178 cm TPR: 37. 3°C / 98 bpm / 20 BP: 127/85 mm. Hg. Skin: normal skin turgor Head & Skull: Bold, no OP scars Eyes: Pupils 3. 0 / 3. 0 Light reflex sluggish Conjunctiva pink

Physical Examination ENT & Mouth: Hearing normal, oral mucosa intact Neck: No jugular vein engorgement, no carotid bruits Neck movement normal, no palpable lymph nodes Thyroid gland impalpable Chest & Lungs: Breathing sounds regular, bilateral expansion symmetric Heart: Heart sounds regular, no murmurs.

Physical Examination Abdomen: Flat, soft, no tenderness Liver and spleen impalpable. Extremities: Movement of upper extremities normal Movement of lower extremities ok, but weak Back & Spine: No kocking pain over C-V angles

Neurological Examination Level of consciousness : clear, alert Mental status normal Judgement Orientation Memory Abstract thinking Calculation Speech Content logical, comprehensible Articulation slightly unclear

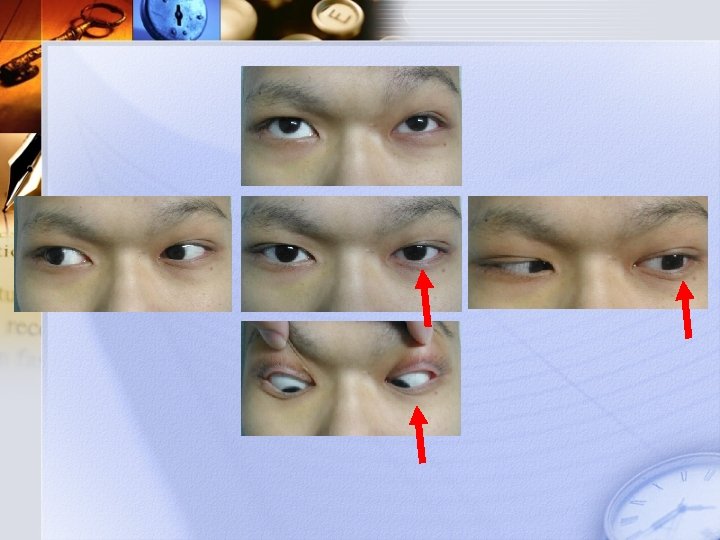
Neurological Examination Cranial nerves : CN I: no loss of smell CN II: Pupils isocoric 3. 0 / 3. 0, light reflex sluggish Visual field normal Visual acuity well CN III, IV, VI: Left eye lateral movement impaired CN V: Normal muscle power of masseter No numbness over face Corneal reflex normal

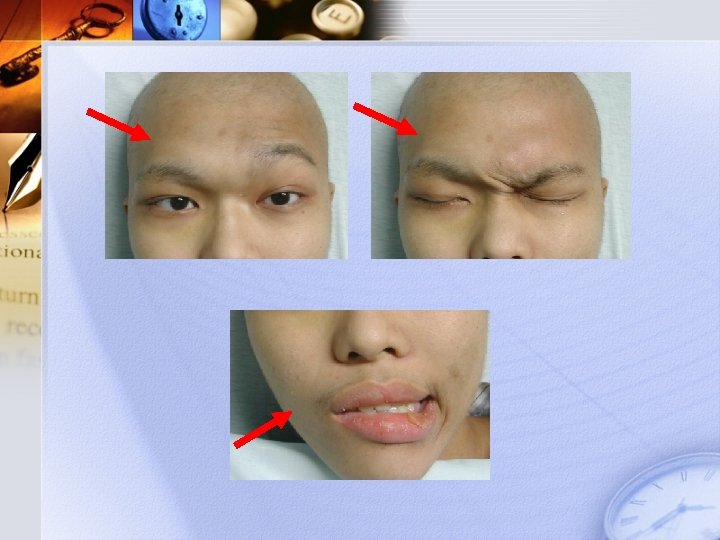
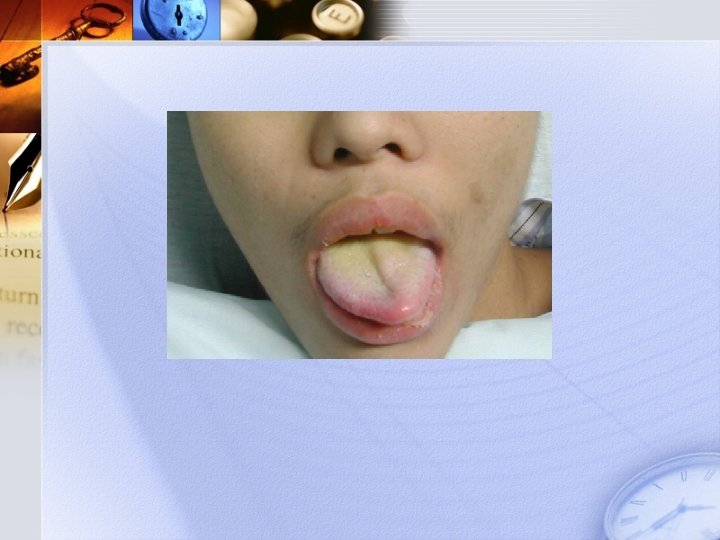
Neurological Examination CN VII: Right facial expression impaired Peripheral type Bell’s facial palsy CN VIII: hearing normal CN IX, X: Phonation normal Swallowing normal No deviation of uvula CN XI: Normal muscle power of S. C. M & trapezious m. CN XII: Leftward deviation of tongue
")
Neurological Examination Motor system: Bilateral lower extremity weakness Stool Incontinence (+)
 Sensory system :")
Neurological Examination Motor system: Bilateral lower extremity weakness Stool Incontinence (+) Sensory system : Decreased sensation over right lateral thigh
 Sensory system :")
Neurological Examination Motor system: Bilateral lower extremity weakness Stool Incontinence (+) Sensory system : Decreased sensation over right lateral thigh Cerebellar function: F-to-N : intact RAM : intact Truncal ataxia : nil
 Sensory system :")
Neurological Examination Motor system: Bilateral lower extremity weakness Stool Incontinence (+) Sensory system : Decreased sensation over right lateral thigh Cerebellar function: F-to-N : intact RAM : intact Truncal ataxia : nil Deep tendon reflex Diffuse decrease of DTR
 2) 3) 4) 5) 6) 7) Left eye deviation")
Summary of Neurological Findings 1) 2) 3) 4) 5) 6) 7) Left eye deviation Right Bell’s palsy Tongue deviation Right thigh numbness Bil. lower extremity weakness Stool incontinence Diffuse decrease of DTR
 2) 3) 4) 5) 6) 7) Left eye deviation")
Summary of Neurological Findings 1) 2) 3) 4) 5) 6) 7) Left eye deviation (CNIII, VI) Right Bell’s palsy (CNVII peripheral) Tongue deviation (CN XII) Right thigh numbness (L 1) Bil. lower extremity weakness (PT) Stool incontinence (Spine) Diffuse decrease of DTR (K+)

Lab Data Upon Admission…

<CBC>

<CBC>

2005/10/11 PA CXR

Problem List Burkitt’s lymphoma with CNS replapse Hypokalemia, Hyponatremia

Treatment Plan Burkitt’s lymphoma with CNS replapse Bone marrow aspiration CSF study Intra-thecal chemotherapy CNS Radiotherapy Hypokalemia, Hyponatremia K+, Na+ supplement

Bone Marrow Aspiration Large lymphocytes >Blue cytoplasm >Vacuoles 10/12

Bone Marrow Aspiration Large lymphocytes >Blue cytoplasm >Vacuoles RELAPSE! 10/12

2005/10/12 Lumbar puncture

2005/10/12 Lumbar puncture Cytology: Burkitt’s lymphoma with CNS involvement Massive tumor cells with large nucleus, scanty cytoplasm Intrathecal methotrexate

2005/10/12 Lumbar puncture

2005/10/12 Lumbar puncture Cytology: Burkitt’s lymphoma with CNS involvement Massive tumor cells Some cell necrosis Intrathecal methotrexate

2005/10/17 Lumbar puncture

2005/10/17 Lumbar puncture Cytology: Burkitt’s lymphoma with CNS involvement Some tumor cells Cell necrosis

Follow-up Conditions 10/16 Spontaneous stool passage Able to stand, walk slowly

Follow-up Conditions 10/16 Spontaneous stool passage Able to stand, walk slowly Questions 10/17 ? Left eye lateral movement (+) Walking improved Swallowing improved DTR (+)

Discussion Burkitt’s Lymphoma with Central Nervous System Relapse

Discussion Burkitt’s Lymphoma with Central Nervous System Relapse IT HAPPENS!

Natural Course Burkitt's Lymphoma CNS involvement: 20~30% Presentation? Risk factors? Benefit? Prognosis? CNS prophylaxis regimen?

Presentation The commonest features Headache Cranial nerve palsies Spinal cord compression Altered mental state and affect Central Nervous System Lymphoma Andrew Lister, Lauren E. Abrey, and John T. Sandlund, Hematology 2002

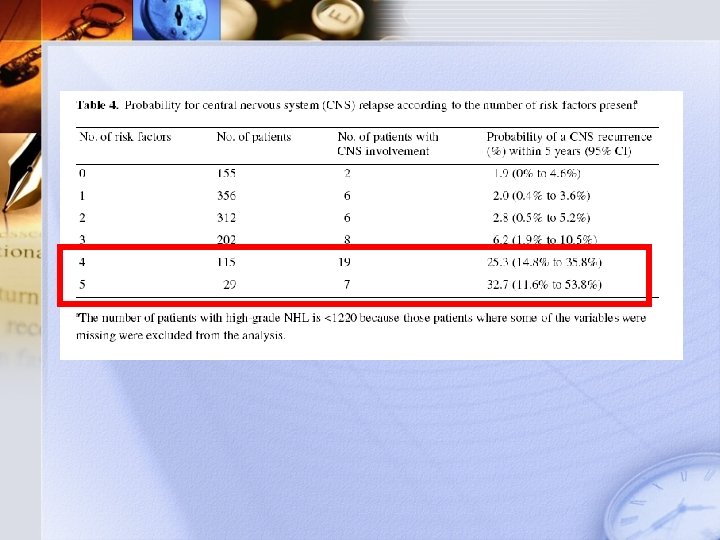
Risk Factors

Risk Factors 1980~1996 Norwegian Radium Hospital 2514 Non-Hodgkin Lymphoma patients Without CNS presentation Retrospective analysis
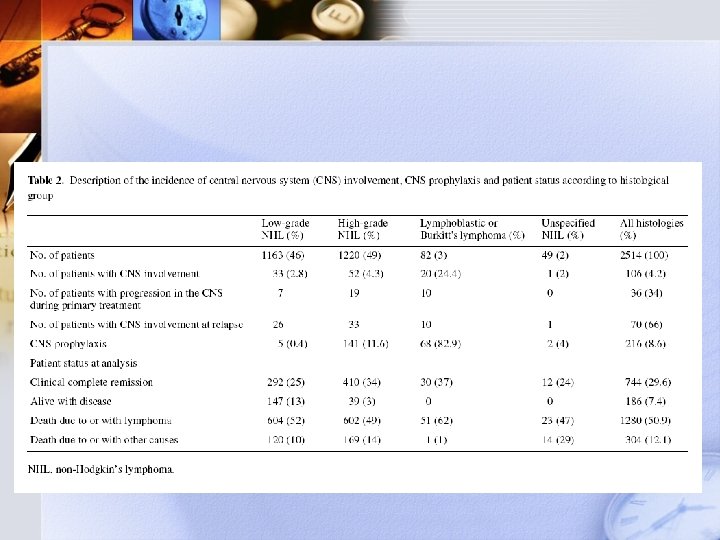
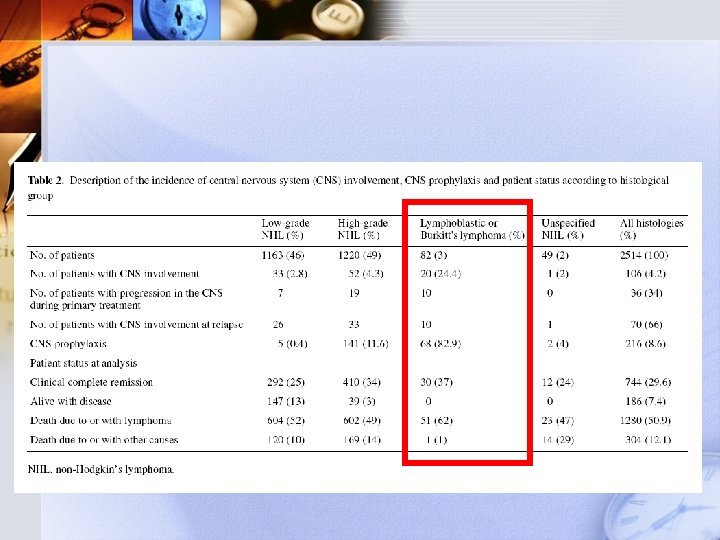

Risk Factors Non-Hodgkin’s Lymphoma Age > 60 years old LDH > 450 U/L Albumin < 35 g/L Retroperitoneal gland involvement Extranodal sites >1
 Useful for High-grade NHL")
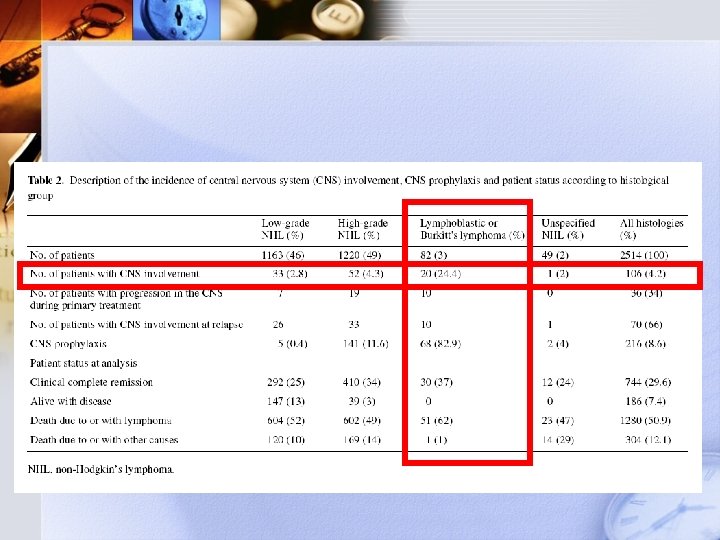
Burkitt’s type is a risk factor! (24%) Useful for High-grade NHL
 Overall 24% Without prophylaxis")
Benefit of Prophylaxis CNS involvement in Burkitt’s (at 5 years) Overall 24% Without prophylaxis 78% With prophylaxis 19% Central Nervous System involvement following diagnosis of non-Hodgkin’s lymphoma: a risk model A. Hollender et al. Annals of Oncology 2002

Prognosis CNS involvement to death Median survival Primary progression 2. 4 Months Relapse 2. 2 Months

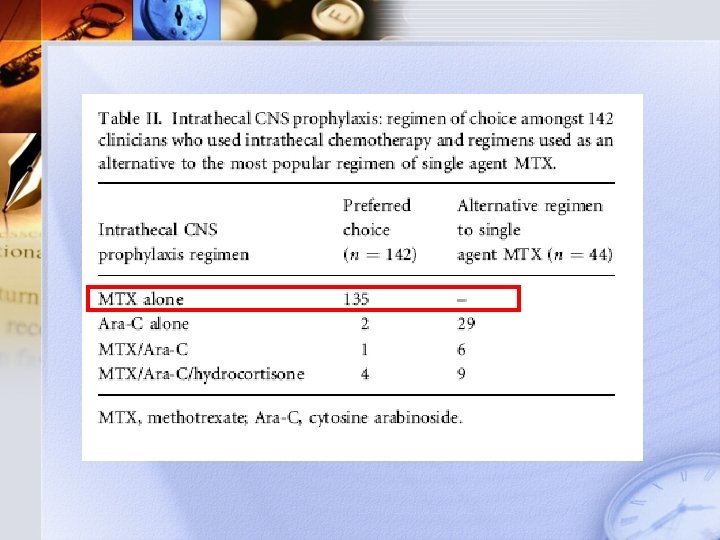
Regimen
 293 questionnaires 158 Received 65 Followed")
Regimen 2004 Feb. ~Apr. (159 UK Medical Centers) 293 questionnaires 158 Received 65 Followed by telephone 70 Did not care for NHL patients

96%

Back to our patient… Presentation Risk Factors Regimen Prognosis

Back to our patient… Presentation Typical relapse Risk Factors Burkitt’s type high risk Regimen MTX based (+Ara-C) Prognosis Poor

Back to our patient… Presentation Comments? Typical relapse Risk Factors Burkitt’s type high risk Regimen MTX based (+Ara-C) Prognosis Poor
 If patient turned out to have normal CSF study, what is")
Discussion comments 1) If patient turned out to have normal CSF study, what is our next step? Cancinomatosis of meninges can also be diagnosed through MRI image studies. 2) The journals involved in this discussion did not help with patient’s future management. What are some other topics of consideration in the benefit of our patient? The discussion included here focused mainly on statistical analysis of the course of Burkitt’s lymphoma. Of course, newer studies on autologous stem cell transplant for cure also being carried out. This topic should also be included here.
- Slides: 74