Case 1 M H Chico State U California

 n n 18 M")




 ICF & (1/3)ECF (Interstitial.")


 Symptoms 135 - 130 Decreased taste 130 - 125")







 until resolved usually")
 n n n It’s July 1 st and the Ortho R")
 n Overaggressive correction of the serum sodium level (usually >12")
 n Hypovolemic hyponatremia n n Correct with NS (0. 9%) Euvolemic")
 n 28 F enters radio station")

- Slides: 29
Case 1 - M. H. (Chico State U. , California) n n 18 M presents after 3 grand-mal seizures after collapsing during fraternity hazing ritual Pledges were forced to do push-ups/exercises for hours in raw sewage that had leaked into basement of fraternity Kept drinking from 5 gallon jug of water which was continuously refilled Vomitted and urinated on themselves
Case 1 n Initial vitals: n n n 120/60 70 20 98% RA T=37. 5 Clinically euvolemic Confused
Case 1 n n Initial labs Na = 110, urine Na <10, serum osmol = 270 How would you treat?
Hyponatremia Matthew Harrington Sultana Qureshi, R 2 Lab Rounds Feb 8, 2007
Hypo. Na Basics n n n Hypo. Na is a symptom of disease Na <135 m. Eq/L Most common lyte abn in hospital pts Incidence 1%, increases with age Acute, symptomatic cases, mortality up to 18%
Quick Physiology Review n 3 fluid compartments n n (2/3) ICF & (1/3)ECF (Interstitial. F + IVF) Na concentration governs movement of water across these spaces Body tightly maintains serum osmolality within 1 -2% of 275 -295 mosmol/kg n Na balance = Renin-angiotensin n Water balance = ADH
Quick Physiology Review n n Hypotension or low ECF renin release from JGA angiotensin II aldosterone production Na reabsorption and K excretion Incr serum osmolality, Decr. BP or volume ADH release from post. Pituitary n More sens to hypovolemia than low osmol.
Clinical Features n Absolute Na level not as important as RATE OF DECLINE
Symptoms Serum Na+ (m. Eq/L) Symptoms 135 - 130 Decreased taste 130 - 125 Thirst Anorexia, N + V Muscle cramps 125 - 120 Weakness Lethargy Restlessness Confusion Delirium Coma Seizures < 120 Thanks to Moritz!
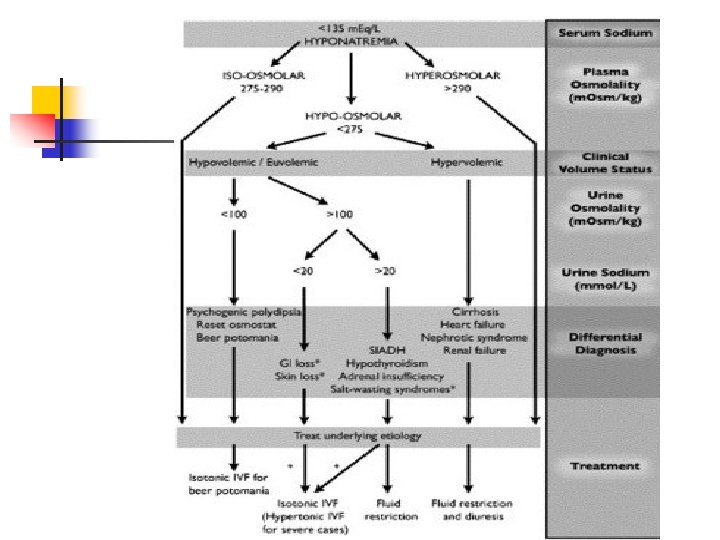
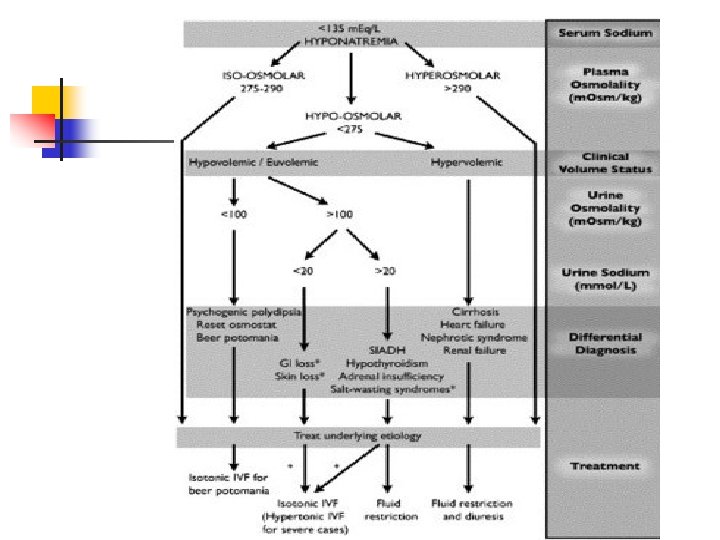
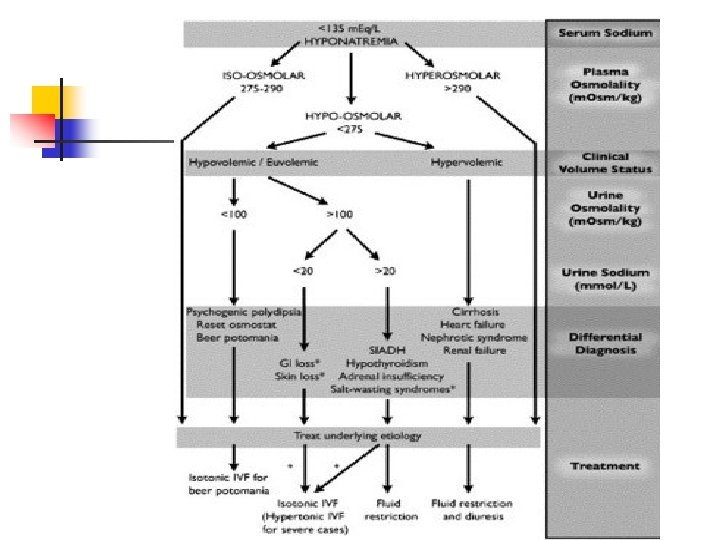
Approach n n Classify Osmolality and Volume status Osmolality n n n Hyperosmolar – excess solutes (ie glucose) draw water into ECF diluting Na Iso-osmolar – psuedohyponatremia Hypo-osmolar (MOST COMMON) – excess water in relation to Na stores (may be incr, decr or n) – categorized by volume status
Hypo-osmolar Hypo. Na n Hypervolemic n n Euvolemic n n CHF, ARF, CRF, cirrhosis/ascites, pregnancy SIADH, adrenal insuff, hypothyroid, psychogenic polydipsia, sports Hypovolemic n Diuretics, diarrhea, sweating, third-spacing, saltwasting nephropathy
Causes of SIADH n CNS disease n n n Brain tumor infarction injury abscess Meningitis/ Encephalitis n Drugs n n Pulmonary disease n n Pneumonia Tuberculosis Lung abscess Pulmonary aspergillosis n n n Exogenous vasopressin (enuresis) Diuretics Chlorpropamide Vincristine Thioridazine Cyclophosphamide
Most common is hypo-osmolar hyponatremia
Case 2 n n 75 F – weak and dizzy x 1 week, falls at home presenting with hip # PMHx – Hyperlipidemia, HTN, chronic diarrhea NYD Meds: HCTZ, lipitor Vitals: 85, 110/70, 14, 95% RA
Case 2 n n n Labs: Na- 112, K-4. 5, Cl- 82, CO 2 -12 Serum osmol – 240 Urine osmol – 300 Urine Na - <10 Cause of Hypo. Na? How would you treat?
Management n n Guided by severity of symptoms and acuity Chronic n n Gradual correction <0. 5 m. Eq/L/hr Acute/Symptomatic n Tolerate faster correction up to 1 -2 m. Eq/l/hr
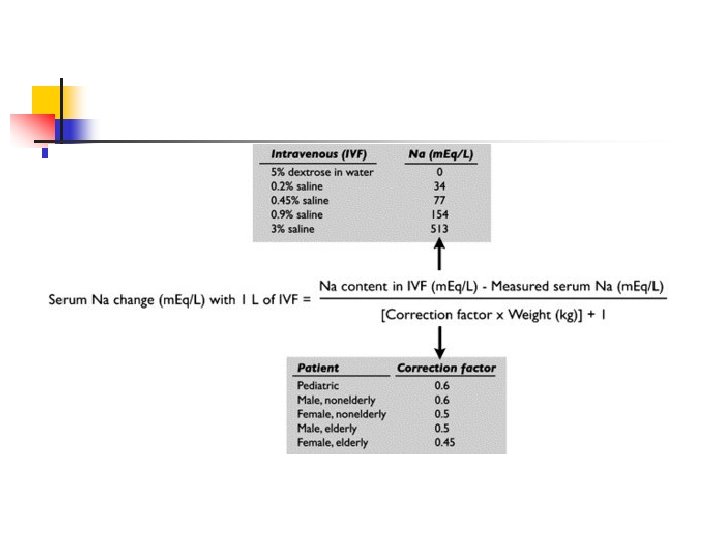
Management n CNS symptoms/seizures n n Correct with hypertonic saline (3%) until resolved usually need to increase Na by 4 -6 m. Eq/L only Then correct 8 -10 m. Eq/L/day Formula n (Desired [Na+] – measured [Na+] ) x 0. 6 Wt(kg) = m. Eq Na+ req’d n Eg (117 -112) X 0. 6(70) = 210 m. Eq
Case 2 (continued) n n n It’s July 1 st and the Ortho R 1 decides to fluid resuscitate her with NS 2 L bolus, then runs it at 200 cc/hr Pt admitted to Ortho Next morning, Na corrected to 136 Later that evening, pt develops confusion, dysarthria, unable to move her arms and legs What’s happening? Call stroke team?
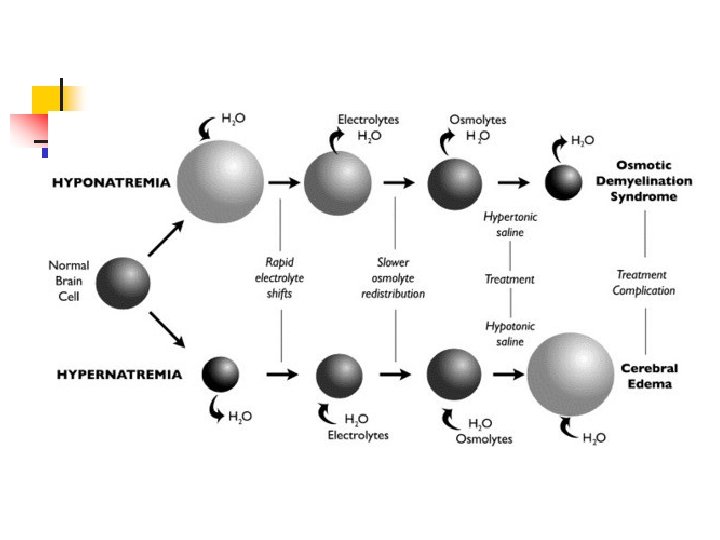
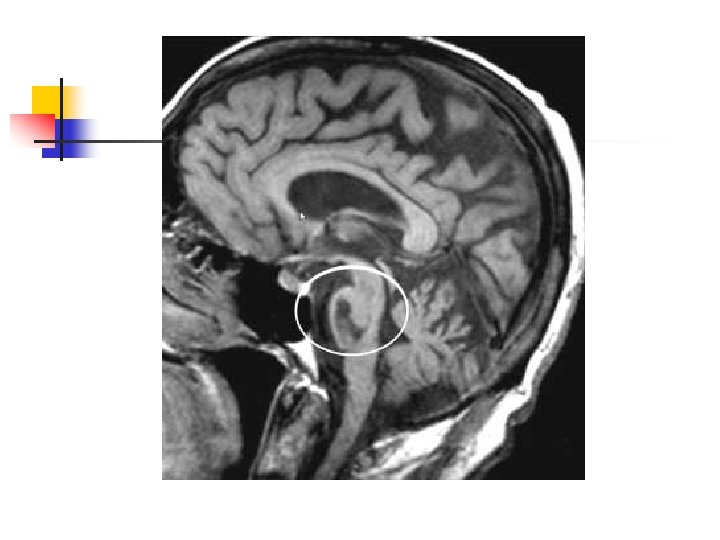
Central Pontine Myelinolysis (CPM) n Overaggressive correction of the serum sodium level (usually >12 m. Eq/L/day) n Destruction of myelin in the pons (due to rapid changes in cell volume? ) n Pts may develop confusion, cranial nerve palsies, spastic quadriplegia, or coma n More likely to occur in patients with chronic hyponatremia n Most cases reported in alcoholic, malnourished, and elderly patients n Can develop 1 -3 days after rapid Na correction n Diagnosed by MRI n Supportive Management
Treatment (mild-mod symptoms) n Hypovolemic hyponatremia n n Correct with NS (0. 9%) Euvolemic hyponatremia: n n n Restrict free water intake Treat underlying cause No NS in SIADH: n n n Worsens due to excessive water retention Lithium and demeclocycline Hypervolemic hyponatremia: n n Restrict free water intake +/- diuretics (may increase Na loss)
Case 3 (Jan 12, 2007 – Sacremento, CA) n 28 F enters radio station competition “Hold your Wee for a Wii” n n n Contestant who could drink the most water without urinating won Possibly drank up to 2 gallons Nurse called into radio station during competition stating danger Last heard from while driving home with severe headache Found dead next morning
Questions?