Case 1 A 1 year old boy brought


Case 1 A 1 ½ year old boy brought to emergency department having convulsions. Temperature of patient was 39 o. C, no signs of Meningeal irritation. Patient recover of fit after treatment, and was discharged from ER after 4 hour. What is most likely diagnosis. a. Acute meningitis b. Epilepsy c. d. febrile seizure Encephalitis

Case 2 l A febrile 18 month old boy has a 1 minute generalized tonic-clonic seizure. One hour later he looks reasonably well, but has a croupy cough and new runny nose. What is an appropriate work-up? ¡a) EEG ¡b) Lytes, EEG and CT head scan ¡c) Lytes, EEG and MRI head scan ¡d) none of the above

Case 3 A 2 -year-old boy presents to the emergency department for evaluation following a witnessed Seizure. The seizure was described as generalized, lasting less than 10 minutes with a short Postictal period. His exam currently is normal, except for a red, bulging right Tympanic membrane and a temperature of 39°C. What is the most appropriate management For this patient? a) He should be sent for an urgent CT scan of the head b) He should be given antibiotics and antipyretics and observed at home c) He should be admitted to the hospital and an EEG should be performed d) He should be started on phenobarbital and sent home

Febrile seizure l Convulsion that occurs in association with a febrile illness in children between 6 months and 5 years of age in the absence of an identifiable cause.

Incidence l Febrile seizures are a common cause of convulsions in young children l 2 -4% of children < 5 years of age ¡ Incidence as high as 15% in some populations l Usually 6 mo – 5 years of age ¡ Peak occurrence is in children 18 - 24 months of age l Majority (65 to 90%) of these are simple febrile seizures

Genetics l Strong family history in siblings and parents: increase risk 2~3 times l Febrile seizure gene: Chromosome 19 p and 8 q 13 -21 l Autosomal dominant inheritance in some families

Common Causes l. Viral URI l. Reseola l. Acute otitis media lpost immunization

Simple febrile Complex febrile seizure l Lasts less than 15 minutes l Lasts 15 minutes or longer l Occurs once in a l Occurs more than 24 -hour period once in a-24 -hour period l Generalized l No previous neurologic problems l Focal l Patient has known neurologic problems, such as cerebral palsy

Clinical characteristics of simple and complex febrile seizures

Risk Factors for First febrile seizure ¡Day care center attendance ¡Developmental delay ¡Having a first- or second-degree relative with a history of febrile seizure ¡Neonatal nursery stay of more than 30 days l 2 of 4 risk factors have a 28% chance of experiencing at least one febrile seizure

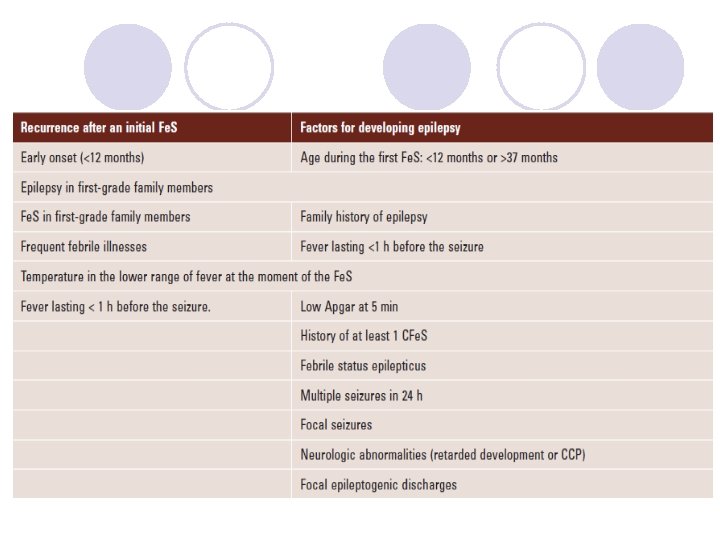
Risk Factors for l Recurrent Febrile Seizures ¡Younger than 18 months ¡Duration of fever (i. e. , shorter duration of fever before seizure equals higher risk of recurrence) ¡Family history of epilepsy (possible, not definitive) ¡Family history of febrile seizures ¡Height of fever (i. e. , the lower the peak fever, the higher the rate of recurrence)
 l Do not necessarily occur with the same degree")
Recurrent Febrile Seizures (cont. ) l Do not necessarily occur with the same degree of fever as the first episode and do not occur every time the child has a fever l Values vary with age from as high as 5065% in children who are < 1 year of age at the time of the first seizure to as low as 20% in older children

Risk factor for epilepsy l Children with febrile seizure have only a 2 % to 4 %lifetime risk l Risk factors for epilepsy ¡ Family history of epilepsy ¡ Complex febrile seizure ¡ Underlying neurologic disorder l If two or more of these risk factors present , the future risk of developing epilepsy is 10. % l General population have. 0/5 % to 1 %lifetime risk of developing epilepsy

Differential diagnosis l CNS infection l Eletrolyte disturbance l Inborn errors of metabolism l Intracranial mass l Diagnosis by history and exclusion
")
Differential diagnosis of febrile seizures (FS)

Red flag signs and symptoms in a child presenting with febrile seizures

Evaluation l The acute component of the evaluation of the febrile child with a seizure is the same as for any child with a fever l Measures include clinical history, presence of chronic illness, recent antibiotic therapy, recent immunizations, and day care attendance
 l 10% of infants < 3 months who appear to be")
Evaluation (cont. ) l 10% of infants < 3 months who appear to be well and have a temperature above 100. 4° F (38° C) have a serious bacterial infection or meningitis l 2% of infants and children > 3 months with a temperature above 102. 2° F (39° C) are found to have bacteremia

Investigation : Blood chemistry ¡Toxicology screening if suspicious ¡CBC, ESR. CRP-UA and UC for detection of fever causes ¡BS, Ca, Na, K, if clinically indicated

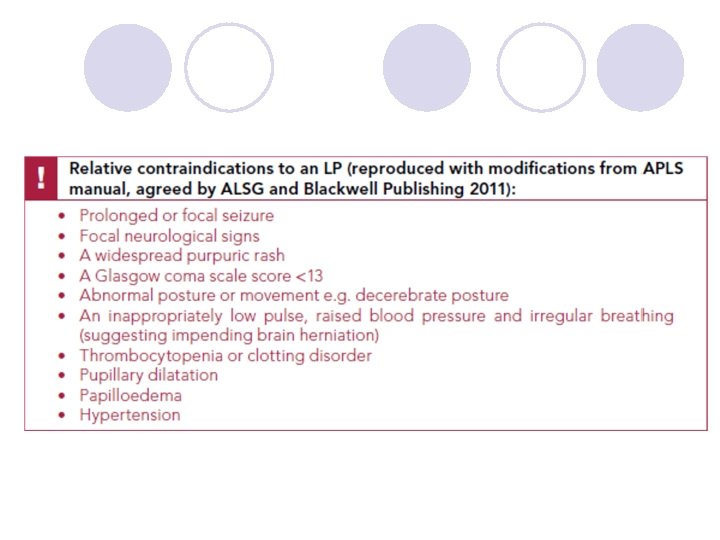
Investigation : LP l When to Do a lumbar puncture? ¡Every child < 1 year of age with a febrile convulsion. ¡Presence of meningeal signs and symptoms. ¡In case of doubt, if LP is not performed , the paediatrician is advised to review the case within a few hours.

Investigation : Imaging l Not necessary in most cases, but exceptions in a child with ¡papilledema ¡cranial nerve palsies (eg. 6 th nerve palsy) ¡other persisting focal neurological signs (eg. hemiparesis ( ¡marked depression in mental status

Investigation : EEG l Rarely indicated in the management of a simple febrile convulsion l Complex febrile seizure

Acute management : general l Same as other type of seizure l Maintain a clear airway (ABC!!!) l Give oxygen if available l Apply suction for nasal or oral secretions if facility available l Place the child in a semi-prone position l Protect the child from injury l Loosen clothing or remove excess clothing l Monitor vital sign

Initial management of Febrile Seizures at home

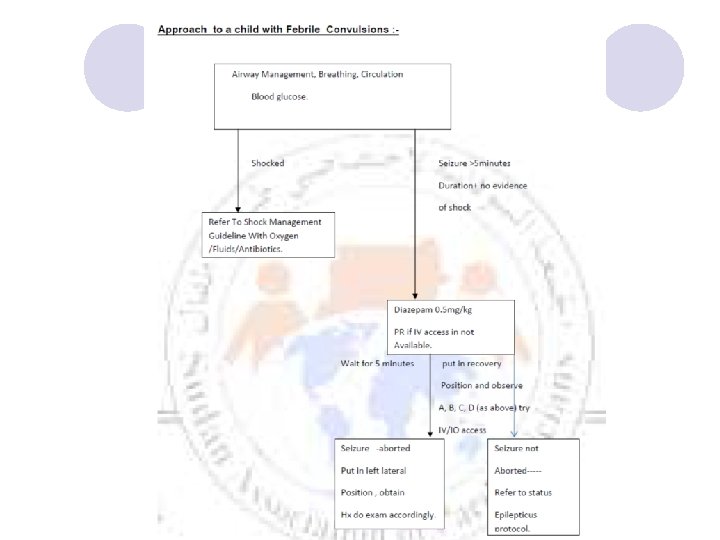
FS treatment in a hospital environment

Acute management : terminate seizure l Benzodiazepines are the first drug of choice for persistent seizure activity. l Diazepam is the most common drug used ¡administer rectal diazepam 0/5 mg/kg/dose ¡IV dose is 0. 3 mg/kg/dose ¡The same dose can be repeated every 10 to 30 minutes to a total of 3 doses, if necessary
 management of Fe. S in children")
Emergent initial therapy for acute (ictal) management of Fe. S in children

Acute management l Observation for several hours after a febrile convulsion l Patients with a simple febrile seizure may be safely discharged to home with parental reassurance and seizure education. l Follow up care

Hospital Admission : indication l Complex febrile seizure l Suspicious of possibility of meningitis and encephalitis l Age < 18 months l Anxious parents or inadequate home care

Management : fever l Identify cause of fever l Sponging with tepid water l Antipyretics ¡Paracetamol 10 -15 mg/kg/dose orally every 4 -6 h ¡Paracetamol 10 -15 mg/kg/dose IM form if oral route cannot be administered

l. Febrile seizure prophylaxy

Recurrent Febrile Convulsions Management l Intermittent prophylaxis l Continuous prophylaxis

Management : intermittent prophylaxis l Antipyretics and tepid sponge. l Diazepam prophylaxis seems to be effective in reducing the recurrence rate. l Suggested doses for prophylaxis ¡ 0. 5 mg/kg administered orally, or rectally every 12 hr whenever the rectal temperature is > 38. 5 C l Side effects of diazepam ¡ ataxia, lethargy and irritability

Management : continuous prophylaxis l Long-term Anticonvulsant Prophylaxis ¡Phenobarbitone or sodium valproate ¡Currently Not advise due to l. No definitive evidence that anticonvulsants can prevent later epilepsy l. Side effects of medications ¡Only use in highly selected case lbased on clinical circumstances and the judgement of the benefit and its side effects
 ¡adverse effects lhyperactivity, lethargy,")
Phenobarbital l effective ¡(25 per 100 to 5 per 100) ¡adverse effects lhyperactivity, lethargy, sleep disturbances, hypersensitivity reactions (SJS)

Primidone l will reduce occurrence l similar problems as with phenobarb

Valproic acid l Only 4% had seizures as opposed to 35% of control l fatal hepatoxicity, thrombocytopenia, pancreatitis, wieght gain or loss

Carbamazepine -phenytoin l not effective

Summarize l Daily doses of an effective anticonvulsant do not seem to give a favorable risk / benefit analysis ¡Can reduce Sz – but are the side effects worth it?

Benzodiazepines l oral diazepam vs placebo ¡ 0. 33 mg/kg q 8 hr for 48 hours ¡did reduce seizures (children had hx of febrile seizures) Sz reduction of 44%

Intellectual Deficit ? l Intellectual outcome is good l Risk of Intellectual Deficit ¡Pre-existing neurological or developmental abnormality ¡Those who developed subsequent afebrile convulsions

1. History taking 2. Physical examination Patient with fever and seizure (age 6 month – 5 years) Assess cause of fever Assess risk factor • Age > 18 months • Age • Normal neurologicl exm • Neurological PE Simple febrile convulsion • Type of seizure If first seizure >>Reassure and follow up If recurrence >> Discuss about oral diazepam prophylaxis • Tepid sponge • Antipyretics • Treat infection • Age<12 month or 12 -18 month with evidence of CNS infection • Abnormal neurologicl exm • Complex febrile convulsion Consider LP CT scan or EEG Normal investigation Abnormal investigation Treat accordingly

What should I do if my child has a convulsion in the future? • Stay calm. • Look at your watch or a clock and time the convulsion. • Do not try to restrain your child and do not put anything in their mouth. • Stay with your child and lay them on their side. • Loosen tight clothing from around that mthe neck and move objects away ay cause injury. • Arrange to see your local doctor/general practitioner after the convulsion has stopped.
- Slides: 49