Case 1 50 year old male with no








































 -0. 5% diltiazem -Nitrates (glyceryl trinitrate")
 anal sphincterotomy.")











 or can")



 • Palpable \"sausage-shaped\"")







- Slides: 76
Case 1 • 50 year old male with no significant medical background presents with one year history of swelling in the left inguinal area.
• Further history ? • What are your DD? ? • Risk factors ? ?
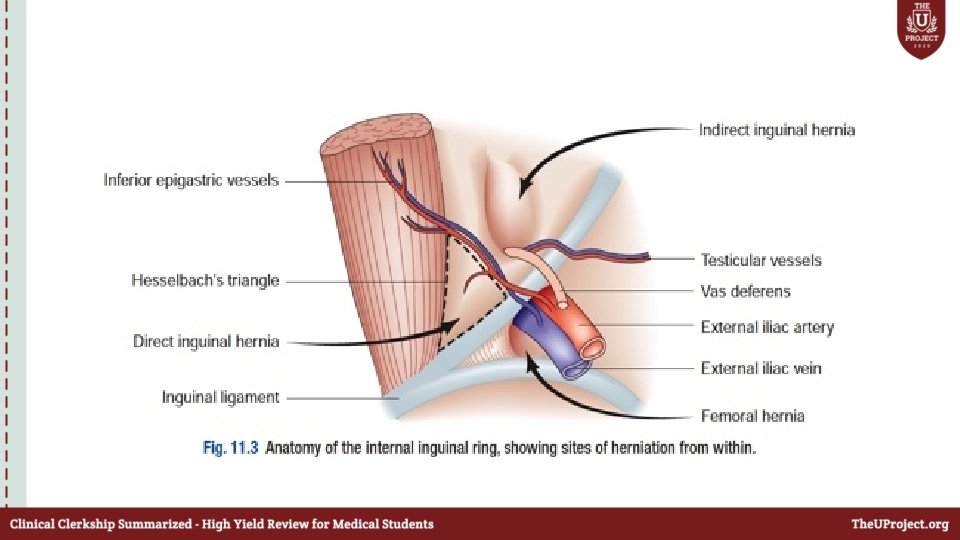
• How will you differentiate between direct and indirect hernia on physical examination ?
• What are the bounderies of hesselbachs triangle ?
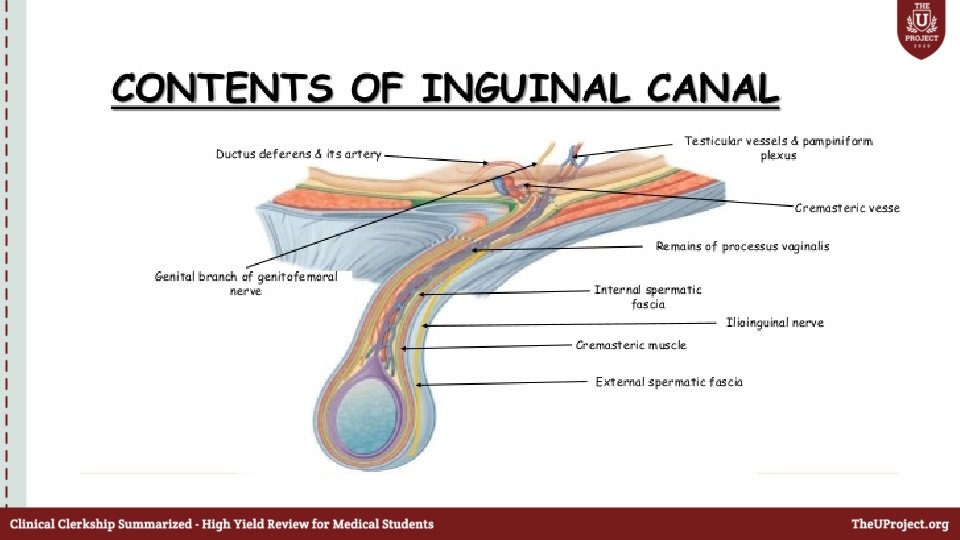
• Boundaries and content of the inguinal canal ?
How will you manage this patient ? ?
• Patient refused surgical intervention and he is asking about the possible complications of inguinal hernia …
• Patient refused surgical intervention , 2 months later he presents to the ED with 3 hours history of fever ; painful irreducible right inguinal swelling ; vomiting and constipation
• What is your diagnosis ? • How will you manage this patient?
• 40 year old patient presents with 2 months history of central abdominal swelling. • Diagnosis? • How will you manage this patient ?
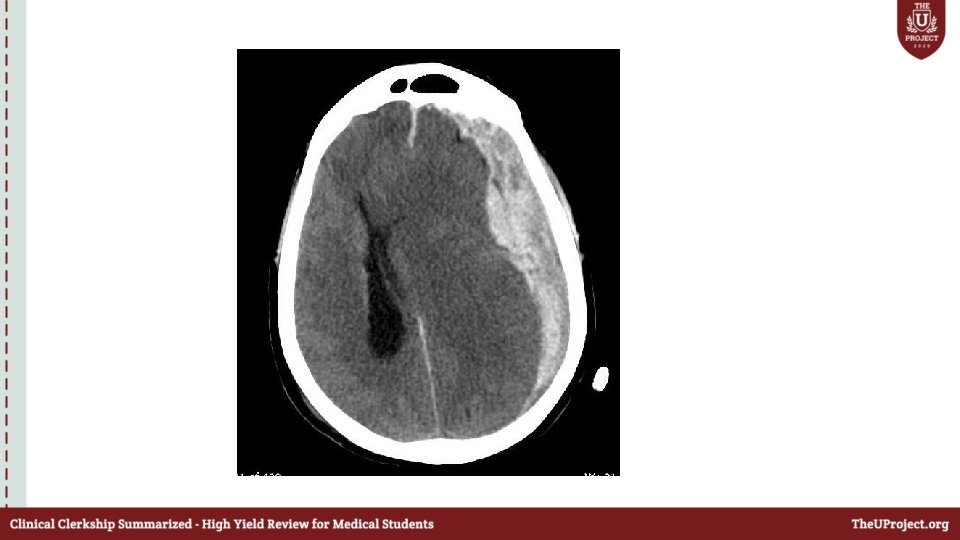
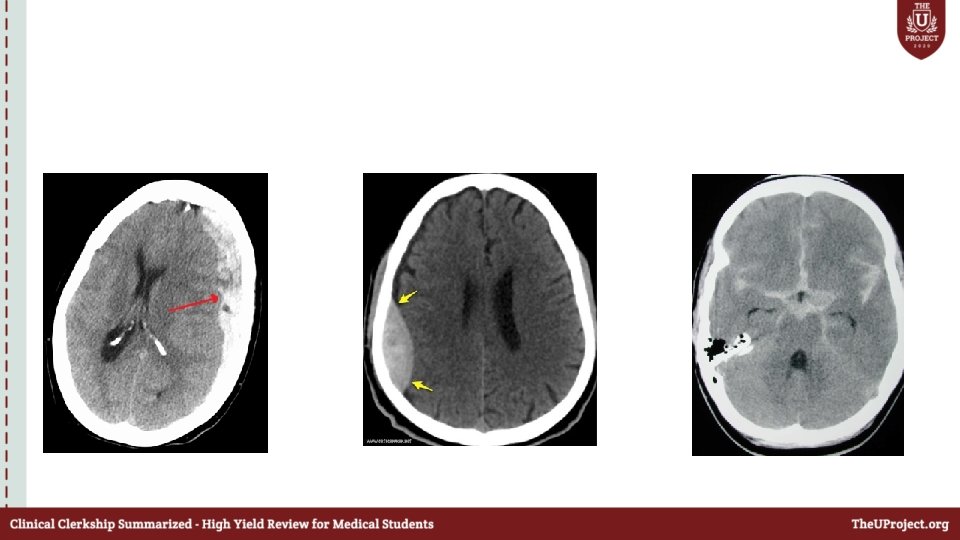
Case 2 • 35 year old male patient was hit by his wife on the head by a metallic pan ; lost consciousness and was brought by EMS to the ED. • As a trauma team leader what will you do before the patient arrives to ED ? • How will you approach this patient ?
Primary survey A: C-spine collar ON Not responding Mouth –full of blood What will you do next ? B: equal air entry bilaterally , SPO 2 100% C: BP 80/60 ; HR 60
• D : GCS: 6 E-1 V-1 M-4 Right pupil was dilated E: No other injuries identified
Secondary survey • Normal • What will you do next ?
• What are the signs of raised ICP?
• How will you mainatain the cerbral perfusion pressure ?
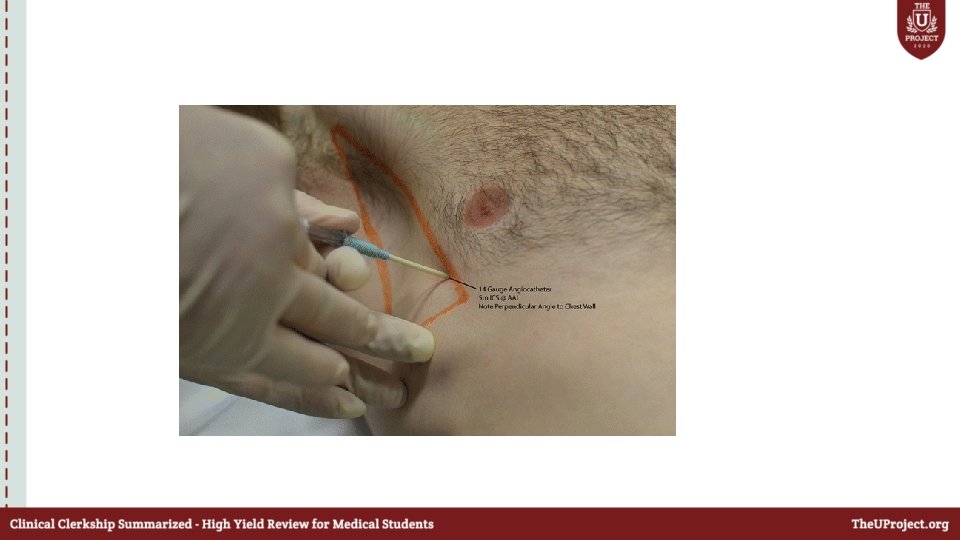
Case 3 • 25 year old man was stabbed in the chest while he was walking in the street. He was brought to ED by EMS. What will you do next ?
• A: Patent Will you keep the C-collar in place ? B: Sp. O 2 : 80% ; reduced air entry on the right side of the chest What will you do next ?
• Where will you place your ICD ? • What will you do next ?
• A: Patient is not responding What will you do ? • BP dropped to 80/40 ; what will you do ? • Type of blood ? • What will you do next ?
• Patient dropped his BP again to 70/40 mm. Hg ; what will you look for ? • What is the definition of massive hemothorax ?
• Chest tube drained 2 L of blood what will you do next ?
Case 4 • 24 year old man involved in a head on collision was brough by EMS to the ED with C collar and backboard in palce. • What will you do next ?
Primary survey • A: Patent ; C-Collar is in palce • B: Sp. O 2 is 80 % ; RR 28 ; absent air entry on the left side of the chest • What will you do next ?
Primary survey • B: Sp. O 2 : 96% ; RR 18 • C: HR 110 bpm , BP 110/90 mm. Hg • D: GCS 15 , reactive pupils
• E: Scalp laceration ; active bleeding What will you do next ?
What will you do next ? ?
• What are the signs of urethral injury ?
Secondary survey • Normal • What do you want to do now ?
What will you do next ?
• Patient was shifted to the ICU ; 3 hours later , • BP : 80/40 mm. Hg • Hb dropped from 12 to 6 ( required 6 units of PRBC). What will you do ?
Case 5 • 30 year old man ; fell from a hight of 3 meters while he was cleaning the roof of his house ; brought by EMS with C collar and backboard in place. • What will you do next ?
Primary survey • A: Patent , C-collar is in place • B: SPO 2 84% ; RR 20 • C: BP 110/80 ; HR 100 • D: GCS : 14 ; pupils are reactive • E: multiple abrassions in the abdomen
What do you want to do next ?
Secondary survey • Normal • What do want to do next ?
Free fluid with no solid organ injury What injuries will u expect & what should you do next ?
Case 6 • 32 year old presents with 3 weeks history of perianal pain. • What further history would you like to obtain ? • DD?
Examination • What is you diagnosis • Will you do PR examination • What are your management options
Mangement • Acute fissures: -Stool softeners (ispaghula ) -0. 5% diltiazem -Nitrates (glyceryl trinitrate 0. 2– 0. 5%) as a cream applied 12 -hourly to the anal canal. -Botulinum toxin injection - temporarily paralyze sphincter -5% lignocaine
Surgical options : • Anal skin advancement flap • Lateral (internal) anal sphincterotomy.
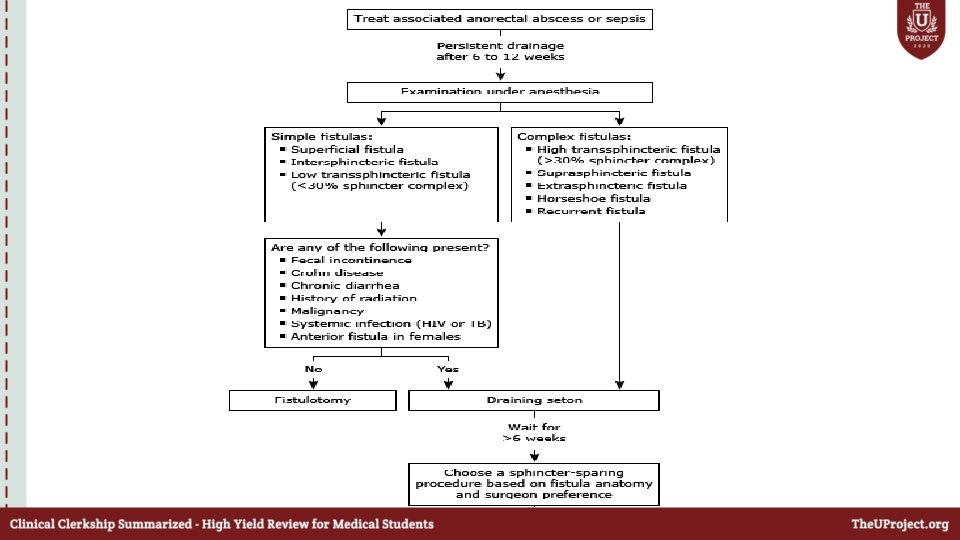
Case 7 • 35 year old man presents with 2 week history of perianal discharge Further history ? DD?
Examination
• What are the different types of perianal fistula ?
• What is goodsall’s rule?
• Gold standard investigation to diagnose perianal fistulas ?
Schematic depiction of a fistulotomy
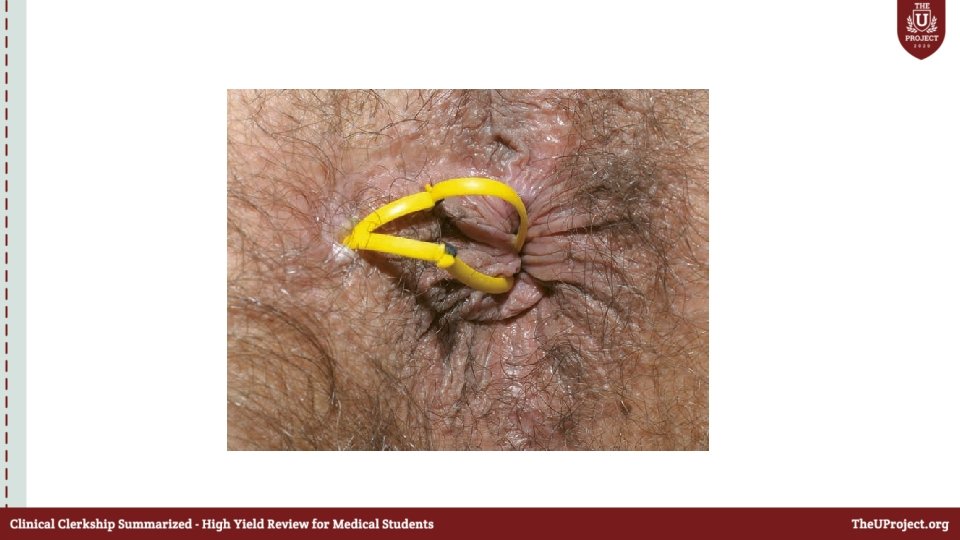
Seton placement
Case 8 • 35 year old man presents with 1 month history of dragging /aching sensation on defication associated with on an off bleeding. • Further history ? • DD?
Diagnosis?
• What are the 3 three anal cushions correspond to 3 terminal branches of the superior rectal artery? • Haemorrhoids classification ? • Haemorrhoids complication ?
Non-operative management • Treat constipation with a high-fiber diet / bulk laxatives / stool softeners. • Barron’s rubber band ligation [most effective] • Submucosal injection of sclerosant • Heat application by infrared photocoagulation.
Operative Management 1. Hemorrhoidectomy: the wound can be left open (Milligan. Morgan) or can be closed. 1. Stapled hemorrhoidopexy: used extensively for symptomatic 2 nd degree, most of 3 rd & 4 th degree.
Choice of treatment: • First degree: avoid constipation and straining • Second degree: conservative, banding, sclerotherapy, hemorrhoidectomy. • Third degree: hemorrhoidectomy if symptomatic • Fourth degree: thrombosed piles treated conservatively ± interval hemorrhoidectomy
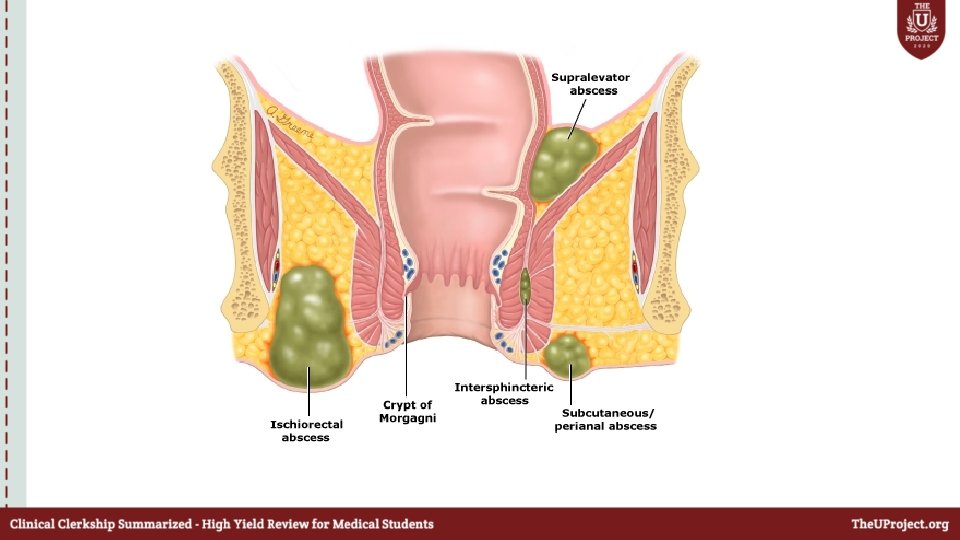
Case 9 • 30 year old patient presents with 5 days history of perianal swelling ; which is very painful and is discharging pus. • What is your diagnosis ?
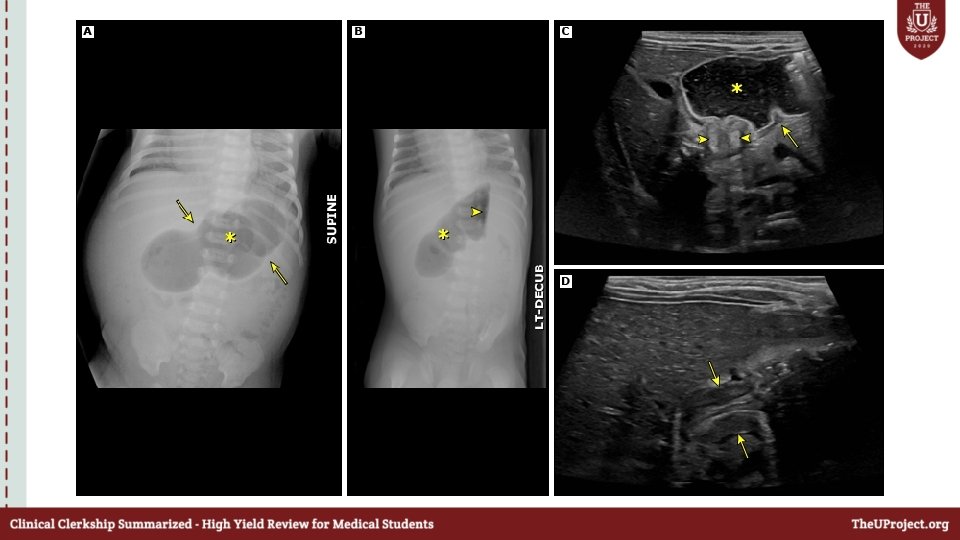
Case 10 • 2 year old girl presents to the ED with 2 hours history of abdominal pain and vomiting Further history ? DD?
Examination • Right lower quadrant that is scaphoid (empty; Dance's sign) • Palpable "sausage-shaped" mass in the right mid or upper abdomen What is your diagnosis?
What do you call this sign
• What are the mangement options for intussusception?
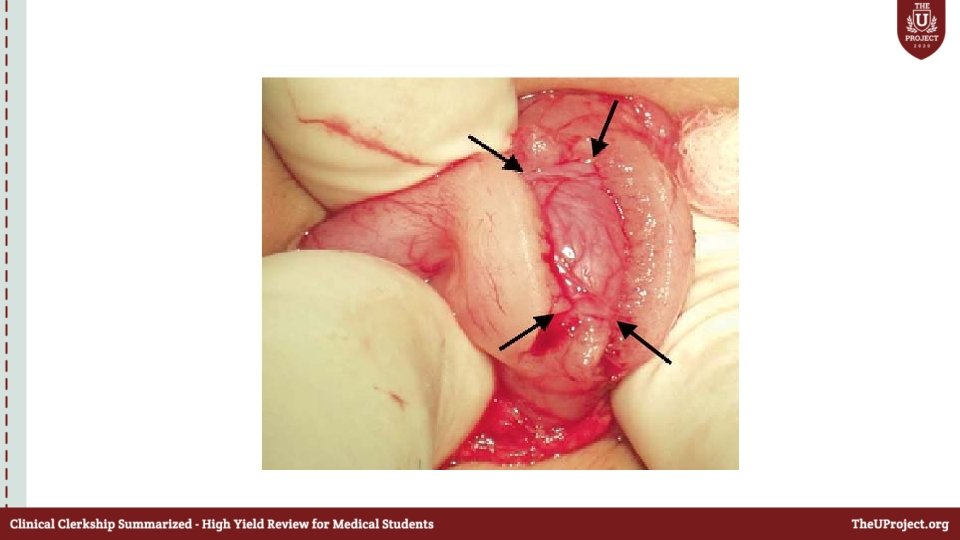
Case 11 • 3 year old boy presents with 3 hours history of painful irreducible left inguinal mass. • What is you diagnosis • How will you manage this patient
Case 12 • 7 weeks old infant presents with 4 hours history of nonbilious projectile vomiting , as per the mother the infant demans to be fed soon afterwards ( hungry vomiter). • What are you DD ?
Examination What is your diagnosis ? Investigations ?
• What is the most common electrolyte abnormality ? • How will you manage this patient ?
• Thank you