Carpal Tunnel Syndrome By Abdullah Radwan Objectives Be

Carpal Tunnel Syndrome By Abdullah Radwan

Objectives • Be familiar with the basic neuroanatomy of the upper limb • Understand factors involved in diagnosing CTS • Recognize the goals and limitations of NCS • Review treatment of CTS

Outline • • Definition Etiology and Risk Factors Neuroanatomy of the Upper Limb Diagnosis: Symptoms and signs Differential diagnosis NCS/EMG and US Treatment

Definition of CTS • Constellation of symptoms and signs secondary to a median neuropathy at the wrist

Outline • • Definition Etiology and Risk Factors Neuroanatomy of the Upper Limb Diagnosis: Symptoms and signs Differential diagnosis NCS/EMG and US Treatment

Etiology • Majority of CTS cases idiopathic

Etiology • Small percentage of CTS due to an identifiable cause, such as: – DM, RA, thyroid disease – Conditions that increase total body fluid (e. g. pregnancy, hemodialysis) – Local wrist lesion (e. g. cyst, fracture, infection, tumor) – Congenital (e. g. small carpal tunnel)

Risk Factors • Gender: F 3 x>M • Age: – Older > younger; very rare in children – Peak prevalence in women >55

Risk Factors • Family history • Certain medical conditions • Workers that use hands and wrists repetitively, especially with high force • Musicians

Risk Factors • Other: Smoking, alcohol, poor nutrition, obesity, high cholesterol
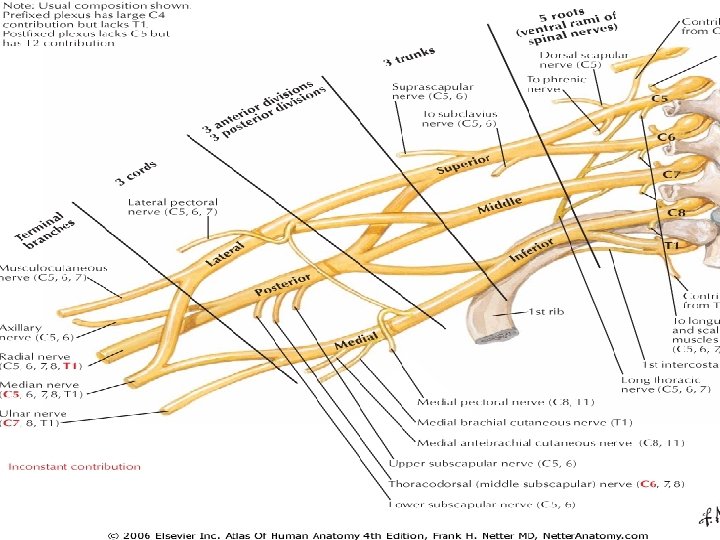
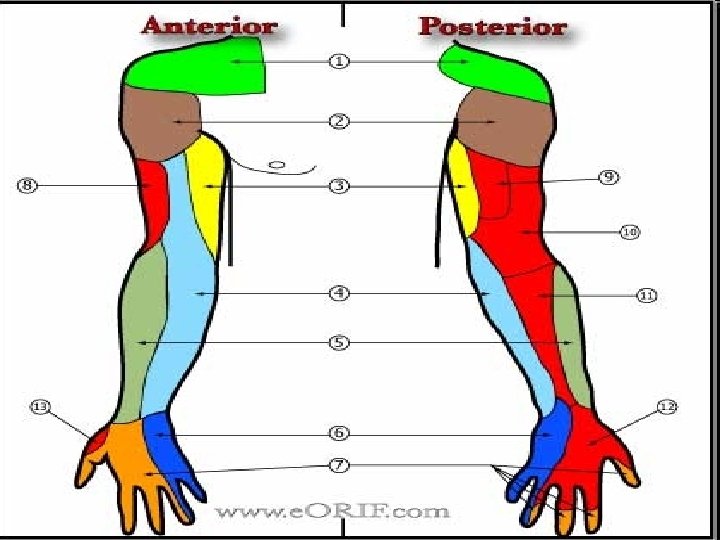


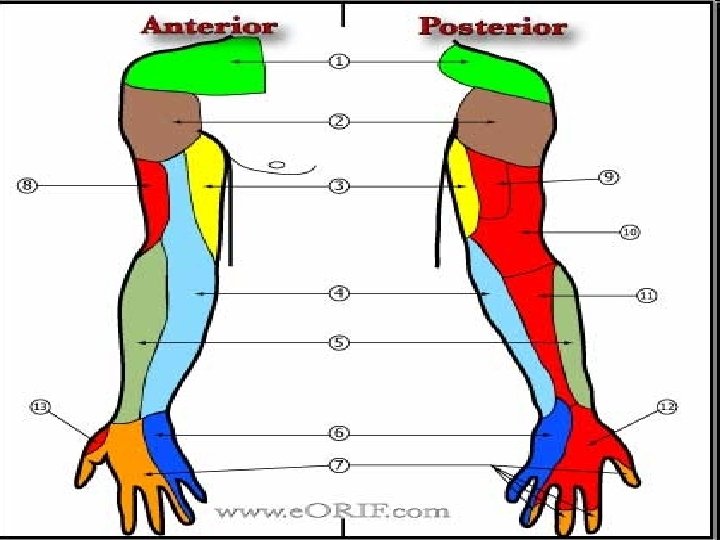
Outline • • Definition Etiology and Risk Factors Neuroanatomy of the Upper Limb Diagnosis: Symptoms and signs Differential diagnosis NCS/EMG and US Treatment

Symptoms • Pattern recognition • Wide variety of symptoms in CTS • Some symptoms are more suggestive of CTS than other symptoms

Symptoms • Classic symptoms in CTS: – Waking up with pain and numbness/paresthesias of the hand – Triggered by driving, holding phone, reading book, typing, writing – Relieving factors • Flick sign • Changes in hand posture

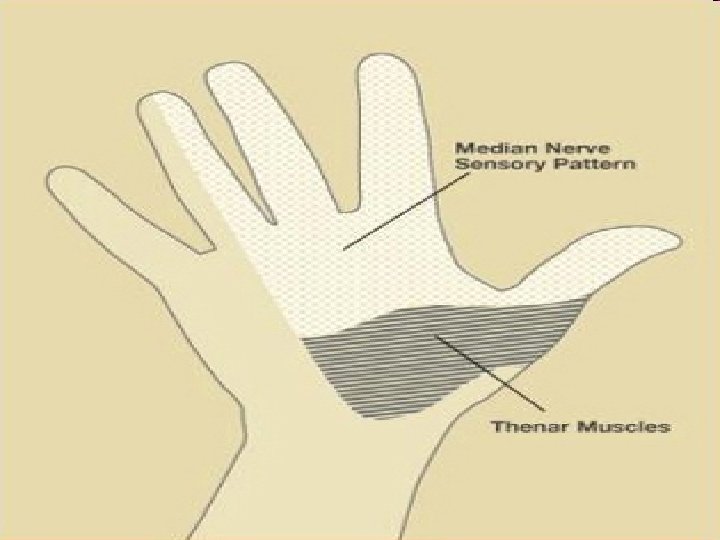
Signs • Key signs suggestive of CTS – Impaired sensation of the lateral 3 -1/2 digits – Weakness of APB and other medianinnervated muscles of thenar eminence – Phalen’s, reverse Phalen’s – Tinel’s – Other: Pressure provocation test, hand elevation test, tourniquet test

")
Signs NOT consistent with CTS – Impaired sensation over the lateral palm (thenar region) – Impaired sensation proximal to wrist – Weakness of hypothenar muscles or other non-median-innervated muscles – Impaired deep tendon reflexes

Outline • • Definition Etiology and Risk Factors Neuroanatomy of the Upper Limb Diagnosis: Symptoms and signs Differential diagnosis NCS/EMG and US Treatment

Differential Diagnosis of CTS – Peripheral NS • Cervical radiculopathy • Brachial plexopathy • Proximal median neuropathy (e. g. in forearm or elbow) • Other mononeuroapthy (e. g. ulnar, radial) • Underlying polyneuropathy – Central NS (e. g. TIA, small lacunar infarct, myelopathy) – Musculoskeletal • Shoulder pain with distal paresthesias • Osteoarthritis • Cumulative trauma disorder

Differential Diagnosis • Peripheral NS: Cervical radiculopathy

DDx: Cervical Radiculopathy • Especially mild cases of cervical radiculopathy • C 6, C 7 • Neck pain, radiation to shoulder, arm, +/distally • Worse with neck movement • Impaired reflexes and strength • Sensory loss beyond distribution of median nerve

Differential Diagnosis • Peripheral NS: Brachial Plexopathy

DDx: Brachial Plexopathy • Uncommon • Etiology: – Trauma – Tumor, Mass – Delayed radiation injury – Plexitis – Postop (e. g. CABG) – Neurogenic TOS

DDx: Brachial Plexopathy • Trauma • Most common cause of brachial plexopathy • Mechanism: – Traction • Car/motorcycle/bike accident, newborn • Upper trunk C 5/6 -Erb’s palsy • Lower trunk C 8/T 1 -Klumpke’s palsy – Penetrating (knife, bullet)
, especially")
DDx: Brachial Plexopathy • Neoplasm, Mass • Metastasis to lymph nodes (most common), especially lymphoma, breast, lung cancer • Local tumor: Pancoast • Other – Direct infilration of nerve: Lymphoma, leukemia – Rare: Primary nerve sheath tumor – Non-neoplastic (unusual): hematoma, vascular anomaly

DDx: Brachial Plexopathy • Delayed Radiation VS • Onset: Progressive, years after radiation • Risk correlated with dose of radiation • Sensory sx prominent (paresthesias, numbness) • (Recurrent) Neoplasm • Onset: Slowly progressive • Prominent pain • Horner’s syndrome

DDx: Brachial Plexopathy • Brachial Plexitis • AKA Neuralgic amyotrophy, Parsonage. Turner • Idiopathic • Often preceded by: viral illness or immunization; also surgery • Long thoracic nerve, anterior interosseous nerve, other • Shoulder pain – Onset: days to weeks after inciting event – Severe pain, awakens from sleep • Weakness and atrophy – Onset: Generally after pain subsides (1 -2 weeks) • +/- Sensory s/sx

DDx: Brachial Plexopathy • Neurogenic TOS • Most cases due to fibrous band between cervical rib and 1 st thoracic rib • Lower trunk, C 8/T 1 • Exam: – Muscles: hand intrinsics, esp thenar T 1; +/- FPL, FDP – Sensory: Ulnar, MABC

Differential Diagnosis • Peripheral NS: Proximal Median Neuropathy

DDx: Proximal Median Neuropathy • • Rare Trauma Ligament of Struthers Anterior Interosseous Syndrome – Pure motor: FPL, PQ, FDP to #2 -3 – “Okay” sign • “Pronator Syndrome” • Possible sites of entrapment – Pronator teres – Lacertus fibrosus (b/t biceps tendon and proximal flexor forearm muscles) – Aponeurotic ridge of FDS (sublimis bridge)

Differential Diagnosis • Peripheral NS: Other Mononeuropathy • Ulnar, Radial

Differential Diagnosis • Peripheral NS: Peripheral Polyneuropathy

Differential Diagnosis • CNS: Cervical Myelopathy

Differential Diagnosis • Musculoskeletal: Shoulder Pathology with Distal Paresthesias

NCS • NCS can be useful in confirming CTS and assessing severity of CTS

NCS • An extension of the clinical examination • Each NCS study must be individualized

NCS • NCS is positive in 91 -98% of patients with clinically diagnosed CTS • (Source: Keles et al, Diagnostic precision of ultrasonography in patients with CTS, Am J Phys Med Rehabil 2005) • Risk of false negatives on NCS generally implies very mild CTS

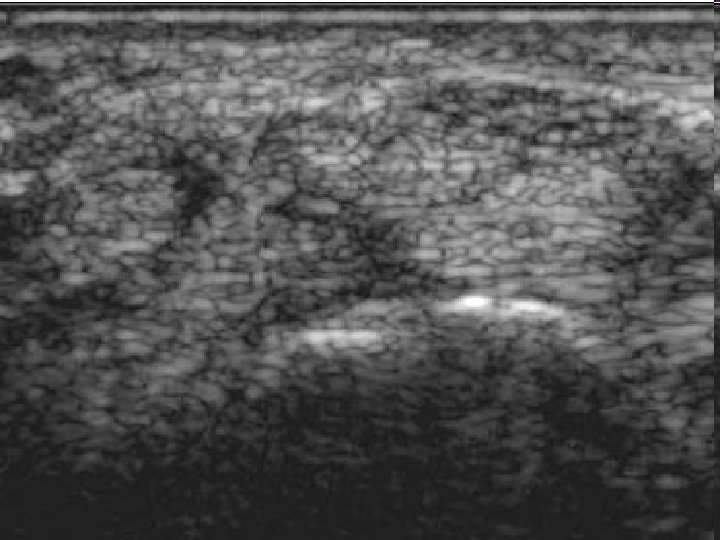
Diagnostic Ultrasound • Real-time imaging of median nerve in carpal tunnel • Qualitative and quantitative • Measurements can include: – Cross-sectional area (CSA) of median nerve – Bowing of flexor retinaculum – Flattening of median nerve in carpal tunnel

Diagnostic Ultrasound • Relatively new development • Aids in diagnosis • Aids in treatment, ultrasound-guided injection of steroid into carpal tunnel

Outline • • Definition Etiology and Risk Factors Neuroanatomy of the Upper Limb Diagnosis: Symptoms and signs Differential diagnosis NCS/EMG and US Treatment

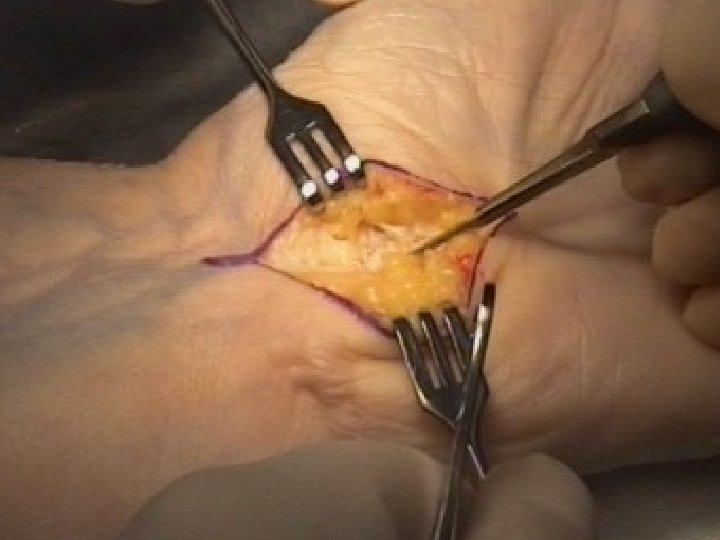
Treatment of CTS



Summary and Conclusion

CTS: Summary and Conclusion • The diagnosis of CTS is made on clinical grounds • Pattern recognition • Be systematic: history, physical, differential diagnosis

Summary and Conclusion • NCS/EMG can be useful in confirming CTS and assessing severity of CTS • Ultrasound can be a helpful adjunct in assessing and treating CTS

Thank You

Questions
- Slides: 56