Carotid Body Tumor Joint Hospital Surgical Grand Round

Carotid Body Tumor Joint Hospital Surgical Grand Round 24/10/2015

Epidemiology ß Rare tumor ß Parasympathetic paragangliomas: Þ ß prevalence of 1 -2 per 100, 000 population Carotid body tumor constitute 65% of head and neck paragangliomas Þ Sevilla Garcia MA, Llorente Pendas JL, Rodrigo Tapia JP, Garcia Rostan G, Suarez Fente V, Coca Pelaz A. [Head and neck paragangliomas: revision of 89 cases in 73 patients]. Acta Otorrinolaringol Esp. 2007 Mar. 58(3): 94 -100.

Relevant Anatomy ß ß Posteromedial aspect of the carotid artery bifurcation Peri-adventitial tissue layer Blood supply from external carotid artery; typically ascending pharyngeal artery Innervated by Hering Nerve; a branch from glossopharyngeal nerve

Histology ß Type I cells: Þ chief cells ß predominate in carotid body tumors; contain catecholaminebound granules Type II cells: Þ sustentacular cells located at the periphery, are devoid of granules
 ß Familial Þ ß Hyperplastic Þ ß Defective succinate dehydrogenase")
Classification ß Sporadic (85%) ß Familial Þ ß Hyperplastic Þ ß Defective succinate dehydrogenase Chronic hypoxia Syndromic Þ MEN type II, von Hippel-Lindau syndrome, and neurofibromatosis type 1
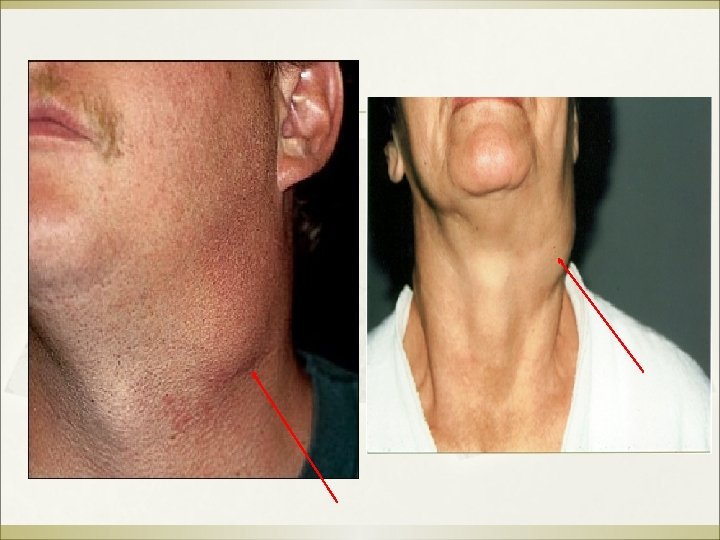

Presentation ß Palpable neck mass Þ Þ Þ Asymptomatic Onset after age 40 slow-growing � Þ Fontaine sign � Þ doubling time of carotid body was 7. 13 years with a median growth rate of 0. 83 mm/year vertically fixed because of its attachment to the bifurcation of the common carotid Jansen JC, van den Berg R, Kuiper A, van der Mey AG, Zwinderman AH, Cornelisse CJ. Estimation of growth rate in patients with head and neck paragangliomas influences the treatment proposal. Cancer. 2000 Jun 15. 88(12): 2811 -6.

Urine catecholamines ß Pick up functional tumors involved in hereditary or syndromic disease

USG neck with Doppler

CT scan Lyre sign

MRI / MRA

MRI / MRA ß ß Well defined mass with salt and pepper appearance on T 1 -weighted image T 2 hyperintense Contrast enhanced Provides better insight into the vascularity of the tumor and its feeder vessels Knight TT Jr, Gonzalez JA, Rary JM, Rush DS. Current concepts for the surgical management of carotid body tumor. Am J Surg. 2006 Jan. 191(1): 104 -10.

Carotid angiogram ß ß ß Better visualization of feeder vessel Invasive Preoperative planning for large tumors

Shamblin Staging - Based on relationship of tumor with carotid vessels and difficulty of surgical resection - Correspond to postoperative side effects

Shamblin Staging by MRI ß ß -Based on measurement of the degree of circumferential contact between Internal carotid artery and the tumor Type 1: < 180 degrees Type 2: 180 - 270 degrees Type 3: > 270 degrees Arya S, Rao V, Juvekar S, Dcruz AK. Carotid body tumors: objective criteria to predict the Shamblin group on MR imaging. AJNR Am J Neuroradiol. 2008 Aug. 29(7): 1349 -54

Young man with carotid body tumor ß ß Presented with right neck mass at age 19 Private USG neck showed right carotid body tumor

CT neck

MRI neck

MRA

Carotid Angiogram ß Right carotid body tumor with blood supply solely from External carotid artery and its branches

Management ß ß ß Surgery Radiotherapy Embolization

Management ß ß ß Surgery vs Radiotherapy Use of preoperative embolization? ? Points to consider: Þ Age and health of patient Þ Bilaterality of lesions, synchronous paragangliomas in other body parts Þ Recurrence - Li-Shan L, Chang-Wei L, Heng G, Yue-Hong Z, Xing-Ming C, Yong-Jun L. Efficacy of surgical therapy for carotid body tumors. Chin Med Sci J. 2011 Dec. 26(4): 241 -5. - Makeieff M, Raingeard I, Alric P, Bonafe A, Guerrier B, Marty-Ane Ch. Surgical management of carotid body tumors. Ann Surg Oncol. 2008 Aug. 15(8): 2180 -6.

Management ß ß Radiotherapy ? ? Some tumors are not radiosensitive and regrowth have been reported after suppression. Tumors that are treated primarily with radiation are also difficult to resect afterwards because of radiation-induced fibrosis. Some reported no cure rates for patients who received radiation for their carotid body Hinerman RW, Amdur RJ, Morris CG, Kirwan J, Mendenhall WM. tumors. Definitive radiotherapy in the management of paragangliomas arising in the head and neck: a 35 -year experience. Head Neck. 2008 Nov. 30(11): 1431 -8.

Management ß ß ß Preoperative embolization ? ? Rationale: decrease size and vascularity of tumor Used to decrease the risk of intraoperative bleeding, particularly in larger tumors Preoperative embolization is still controversial Sahin MA, Jahollari A, Guler A, Doganci S, Bingol H, Karaman B, et al. Results of combined preoperative direct percutaneous embolization and surgical excision in treatment of carotid body tumors. Vasa. 2011 Nov. 40(6): 461 -6.

Management ß Surgery : Þ ß for younger, healthier patients with carotid body tumors Radiotherapy : Þ for patients who are poor surgical candidates, and for selected individuals with multiple paragangliomas in whom resection may be highly morbid - van der Mey AG, Jansen JC, van Baalen JM. Management of carotid body tumors. Otolaryngol Clin North Am. 2001 Oct. 34(5): 907 -24, vi. - Pellitteri PK, Rinaldo A, Myssiorek D, Gary Jackson C, Bradley PJ, Devaney KO. Paragangliomas of the head and neck. Oral Oncol. 2004 Jul. 40(6): 563 -75.

Young man with carotid body tumor ß Carotid body tumor excision performed ß Uneventful recovery ß Early age onset raise suspicion of familial carotid body tumor

Familial Carotid Body tumor ß 9 susceptibility genes: Þ Þ Þ ß ß NF 1, RET, VHL SDHA, SDHAF 2 and TMEM 127 SDHB, SDHC, SDHD Multiple head and neck paragangliomas are common in patients with SDHD mutations Malignant head and neck paraganglioma is mostly seen in patients with SDHB mutations Offergeld et al. Head and neck paragangliomas: clinical and molecular genetic classification. Clinics (Sao Polo). 2012; 67 Suppl 1: 19 -28.
 ß ß two transmembrane subunits (SDHC and SDHD) two matrix subunits (SDHA")
Succinate dehydrogenase(SDH) ß ß two transmembrane subunits (SDHC and SDHD) two matrix subunits (SDHA and SDHB)
 ß Function: Citric acid cycle")
Succinate dehydrogenase(SDH) ß Function: Citric acid cycle

SDHD mutation ß ß ß Most common type of familial paraganglioma Paraganglioma Syndrome Type 1 Pathogenesis: Defective succinate metabolism Þ Accumulation of succinate trigger hypoxia pathway even in normal oxygen condition Þ Tumorigenesis Þ Exact molecular mechanism is still under - Baysal B. research E. , Ferrell R. E. , Willett-Brozick J. E. , et al. Mutations in SDHD, a mitochondrial Þ complex II gene, in hereditary paraganglioma. Science. 2000; 287(5454): 848– 851. doi: 10. 1126/science. 287. 5454. 848. - Yeng F. Her and L. James Maher, III. Succinate Dehydrogenase Loss in Familial Paraganglioma: Biochemistry, Genetics, and Epigenetics; Int J Endocrinol. 2015; 2015: 296167.

SDHD mutation ß ß ß Chromosome gene locus 11 q 23 Autosomal dominant Maternally imprinted Þ ß ß - Inheriting gene from paternal will have phenotypic expression Highly penetrant 75% of carriers will manifest disease by age 40 Neumann H. P. H. , Pawlu C. , Pęczkowska M. , et al. Distinct clinical features of paraganglioma syndromes associated with SDHB and SDHD and gene mutations. Journal of the American Medical Association. 2004; 292(8): 943– 951. Baysal BE et al. Prevalence of SDHB, SDHC, and SDHD germline mutations in clinic patients with head and neck paragangliomas. J Med Genet. 2002 Mar; 39(3): 178 -83.

SDHD mutation ß ß - Multifocal tumor in 56% of cases Frequent development of head and neck paragangliomas Less commonly develop thoracoabdominal paragangliomas or phaeochromocytomas Rarely develop Renal cell carcinoma Neumann H. P. H. , Pawlu C. , Pęczkowska M. , et al. Distinct clinical features of paraganglioma syndromes associated with SDHB and SDHD and gene mutations. Journal of the American Medical Association. 2004; 292(8): 943– 951. Baysal BE et al. Prevalence of SDHB, SDHC, and SDHD germline mutations in clinic patients with head and neck paragangliomas. J Med Genet. 2002 Mar; 39(3): 178 -83.

Genetic counselling If hereditary paraganglioma is known or strongly suspected, then imaging from neck to pelvis should be performed to exclude synchronous lesions ß Genetic testing is performed on DNA extracted from peripheral blood leucocytes and should include validated methods for detecting point mutations, insertions and deletions as well as large deletions in SDHx Lenders JW, Duh genes QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, Naruse ß M, Pacak K, Young WF Jr; Endocrine Society Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014 Jun; 99(6): 1915 -42. doi: 10. 1210/jc. 2014 -1498.

Genetic counselling A positive result from genetic testing should lead to cascade testing of firstdegree relatives after appropriate counseling ß Individuals discovered to carry a pathogenic mutation in SDHx genes should undergo lifelong biochemical, radiological and clinical surveillance for Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad paragangliomas. ß MH, Naruse M, Pacak K, Young WF Jr; Endocrine Society Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014 Jun; 99(6): 1915 -42. doi: 10. 1210/jc. 2014 -1498.

Young man with carotid body tumor ß ß ß Genetic counselling given Genetic test confirmed familial carotid body tumor with SDHD mutation Patient’s father also have SDHD mutation Þ ß Maternal imprinting Other family members will have genetic test in future

The End Thank you
- Slides: 36