Caring for Sick Women Wessex Maternity Academy Early

")













 Approach • Always start at the top and work your way down")




- Slides: 21
Caring for Sick Women Wessex Maternity Academy
Early warning systems- track and trigger • The Modified Early Obstetric Warning Score (MEOWS) has been designed to allow early recognition of physical deterioration in women by monitoring their physiological parameters • Recent enquiries highlighted that failure to identify early signs of illness has resulted in increased levels of maternal morbidity and maternal deaths
ABCDE Approach to care • This is a methodical assessment of physical condition but in exposure you will complete a top to toe review to ensure thorough assessment completed.
What are we monitoring? ? • • • Respiratory Rate O 2 Saturations (also what O 2 support they are receiving) Heart Rate Systolic Blood Pressure Diastolic Blood Pressure Temperature • Additionally: • Fluid Balance (input and output) • Level of consciousness • When to escalate- what is your plan? • What to do if you are concerned
A - Airway • This should be the first thing we assess. . . why? • What could obstruct an airway • How do you assess airway? ▫ Look ▫ Listen ▫ Feel • Do they look as if additional work of breathing (laboured, chest not rising equally)- if yes to the above please expedite review • Can they speak in full sentences? • Are they short of breath? DO YOU NEED HELP?
B-Breathing • Look, Listen and Feel as before Respiratory rate? Oxygen saturations? In air/ on Oxygen • Snoring https: //www. youtube. com/watch? v=xu-b. Bx. A-e. Kc • Stridor https: //www. youtube. com/watch? v=JSd. EK 79 J 4 dw • Wheezing https: //www. youtube. com/watch? v=T 4 q. Ngi 4 Vrvo • Paradoxical breathing https: //www. youtube. com/watch? v=1 wir 6 q. Racrs
COVID update • Baseline Oxygen Saturations? - these need repeating at a minimum hourly (increase as condition indicates) • If subsequent assessment has there been a disproportionate drop in saturations • Respiratory rate baseline? (again minimum hourlymore often if condition indicates) A rare greater than 30 shows decompensation and requires urgent review • Follow normal MEOWS escalation if resp rate raised or Sp. O 2 low on admission even in absence of raised temperature (local case)
• If oxygen requirements or Fi. O 2 of >40% consider or normal saturations with Raised respiratory rate, drowsiness or reduced urine output- escalate care- facilitate higher levels of care until appropriate place of care identified with support from critical care. DO YOU NEED HELP?
C- Circulation • • Look, listen and feel assessment What are we looking for? How do we assess circulation? What may cause changes in circulation? • Capillary Refill ▫ Press and hold for 5 seconds ▫ Peripheral or Central ▫ Normal = < 2 seconds
C – Circulation continued • Cyanosis DO YOU NEED HELP?
Circulation • Should have included not only observations but also: • Fluid balance status- so input/ output- balance • Recent biochemistry/ microbiology • Sepsis markers if applicable
D – Disability • What methods do we use to assess disability? • Level of consciousness • Blood Glucose levels • Pupil dilation DO YOU NEED HELP?
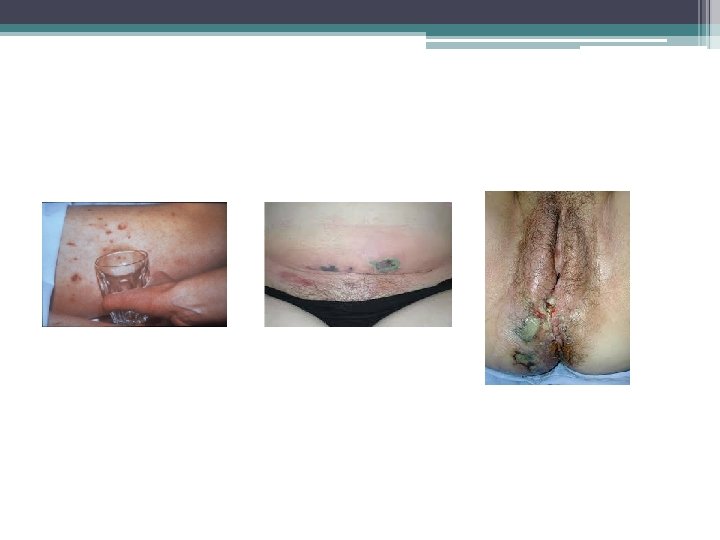
E - Exposure • • • What do we look for? Blood loss Fundal Height Rash/Redness Swelling/Oedema RUQ pain Reflexes Distension unrelated to pregnancy Calf pain/redness/swelling Possible infection sites
DO YOU NEED HELP?
F - Fetus • After 20 weeks the fetus makes the uterus a significant organ, therefore having the capacity to impact on maternal health and wellbeing • Do we need to consider continuous monitoring of the fetus
ABCDE (F) Approach • Always start at the top and work your way down • Write your notes in a systematic way • If you are unhappy/uncertain ALWAYS ask for help. . . I promise NOONE will mind! • Most important: • What is your plan? • When will you reassess?
Who do you need? Neonatal Obstetric theatre staff Obstetric Paediatrics Midwifery Anaesthetic Staff
Example 1 • • • Mrs A G 2 P 2 Day 1 post NVD and 2. 5 L PPH Currently sat up in bed feeding baby A- SV in air Sats 98% B- RR 16 talking in full sentences, normal chest wall movements C- Feels warm peripherally Cap refill <2 seconds , BP 120/70, HR 75, Temp 36. 7 C • D- Alert, no concerns • E- 1 x 16 G cannular R hand patent VIP score 0, Uterus w/c below umbilicus, lochia minimal, AES in situ calf equal and non tender, catheter on free drainage as >150 mls/hr Plan: . . .
Example 2 • • • Mrs B 27/40 admitted to HDU with significant PET Currently lying in be semi recumbent, CTG in progress A- SV in air sats 94% B- RR 18 Normal chest wall movements, talking in full sentences C- BP 180/100 HR 92, Temp 37. 1 C, Cap refill 2 -3 seconds warm peripherally D- Alert E- Pitting oedema to thighs, hands swollen, partner reports facial oedema. C/O RUQ pain. Brisk reflexes and 2++clonus L and R leg. 2 x 16 G cannular 1 x L ACF patent 1 x R forearm both VIP score 0 5 mls/hr Mg. SO 4 75 mls/hr CSL Fluid restricted 80 mls/hr IDC (urometer) draining small amounts concentrated urine approx 15 ml/hr F- CTG in progress fetal movements felt has had 2 x Dexamethasone Plan: . .
• Any Questions? ?