Caries Activity Test Caries Susceptibility And Caries Risk

Caries Activity Test, Caries Susceptibility And Caries Risk

Introduction � Caries Activity refers to the increment of active lesions ( new or recurrent) over a slated period of time. Caries activity is a measure of the speed of progression of a carious lesion. � Caries Susceptibility refers to the inherent propensity of the host and the target tissue, the tooth to be afflicted by the caries process. � Clinical examination of carious lesions with probe and mirror coupled with radiographs neither predicts caries activity nor a patient’s susceptibility to dental caries.

Introduction… � A simple reliable laboratory test that could predict caries activity in a particular patient or indicate a patient’s susceptibility to dental caries, would facilitate the clinical management for the following reasons: 1) To determine the need and extent of personalized preventive measures. 2) To serve as an index of the success of therapeutic measures. 3) To motivate and monitor the effectiveness of the education programmes. 4) To manage the progress of restorative procedures. 5) To identify the high risk groups and individuals.

Introduction… � Prediction of caries activity has value in the dental clinic in selection of risk groups according to the expected caries activity and in dental research for the purpose of screening and evaluation of potential therapeutic agents. � Currently no single caries activity test is sufficiently accurate or reliable to serve as a predictor of potential caries activity for the individual patient.

Classification Of Caries Activity Tests Microbial Tests � Lactobacillus Colony Count Test � Dentocult Lactobacilli Test/ Dip Slide Method � Synder Test � Alban’s Test � Mutans Group Of Streptococci Screening Test 1) Plaque/ Toothpick Method 2) Saliva/ Tongue Blade Method 3) S. Mutans Dip Slide Method � Swab Test � Cariostat test

Classification Of Caries Activity Tests For Evaluating Salivary Defence � Enamel solubility test � Salivary reductase test � Dentobuff test/ salivary buffer capacity test � Saliavry viscosity test � Salivary flow rate test � Fosdick calcium dissolution test � Dewar test

Caries Activity Versus Caries Susceptibility � Many papers refer to laboratory caries activity tests as an assay for the disease susceptibility. � Caries activity refers to the increment of active lesions, including new and recurrent lesions that occur over a stated period of time. � Susceptibility refers to the inherent propensity of the host and the target tissue, the tooth, to be afflicted by the caries process. � In a highly susceptible person even a relatively low cariogenic challenge may result in dental caries, whereas in a patient who is highly resistant to the caries process, a high cariogenic challenge may not be able to produce dental caries.

Caries Activity Versus Caries Susceptibility… � Caries activity tests do not measure the innate susceptibility of the patient to dental caries. � The current tests measure the degree to which the local environmental challenge (diet) favors the probability of new carious lesions. � In considering the tests it is important to keep in mind that the three primary factors; bacterial flora, local substrate and the host interact in determining the caries activity. � Since lab caries activity tests tend to measure only one parameter, that is quantity of a specific bacterial group or their ability to produce acid, the interpretation of the test is more reliable when coupled with good clinical assessment.

Caries Activity Testing Caries activity testing is essential to: Establish an initial baseline level of cariogenic pathogens as a basis for future evaluation and preventive dentistry counseling. 2) Ensure a low level of caries activity before starting any extensive restorative procedure. 3) Monitor patient behaviour towards reducing the number of S. mutans and Lactobacilli as parts of counseling to curtail sucrose intake. 1)

Lactobacillus Colony Count � The first and initially the most widely used microbiological method for assaying caries activity was the lactobacillus colony count, first purposed by Hadley in 1933. � On the basis of microbial analyses of carious dentin, especially salivary Lactobacillus counts, a specific etiologic role of Lactobacillus in the development of caries lesions emerged between 1915 and 1929. � The credit for improved culture techniques for lactobacilli growth and the first systematic investigation of the quantitative incidence of L. acidophilus and caries goes to Rodriguez (1930, 1931).

Lactobacillus Colony Count… � Sensitivity: the probability that a screening procedure will give a positive finding which is in agreement with the validating criteria. � Specificity: the probability that a screening procedure will give a negative finding which is in agreement with the validating criteria.

Lactobacillus Colony Count… � As it was originally described the technique of the lactobacillus count consisted of chewing on a piece of paraffin to collect 2 to 8 ml of saliva, which was then diluted to 10. 0 ml with sterile physiologic saline. � The specimen was shaken by hand for 3 minutes and 0. 1 ml was spread over the surfaces of tomato-juice peptone agar plates (p. H 5. 0)

Lactobacillus Colony Count… � Counts made after 3 to 4 days incubation at 37 o. C, represented the number of lactobacilli per milliliter in the constant volume of the first dilution � This was modified by Jay P in 1949, so that 1. 0 ml. of saliva was added to 4. 0 ml. of acid glucose infusion broth (p. H 5. 0) to give a 1: 5 dilution of the original specimen and 0. 1 of this dilution spread over the medium.

Lactobacillus Colony Count… � The purpose of the acid glucose broth was to furnish a qualitative answer for the presence or absence of gram positive bacilli. � Criticisms of the technique centered around: 1) The crudity of the medium. 2) Failure to indicate physiologic behavior of the organisms cultured 3) Overgrowth of plates by yeast forms and mold contaminants. 4) Length of incubation. 5) Statistical inaccuracies.

Lactobacillus Colony Count… No. of lactobacilli per ml of saliva Caries activity 0 -1000 Light or none Less than 10, 000 Slight Less than 100, 000 Moderate More than 1, 000 Marked
 Useful for monitoring the effectiveness of restorative dentistry")
Lactobacillus Colony Count… Advantages Disadvantages 1) Useful for monitoring the effectiveness of restorative dentistry and care completion. 2) Simple to carry out. 3) Useful as a screening test for caries activity in large groups. 1) Inaccurate for predicting the onset of caries. 2) It does not completely exclude the growth of other aciduric microorganisms. 3) Counts involving individuals are not that reliable. 4) It only takes five minutes to do the test, but the result are not available for several days. 5) Counting is a tedious procedure.
 � A new dip-slide method for")
Lactobacillus Colony Count… Dentocult (Orion Diagnostica, Helsinki. Finland) � A new dip-slide method for counting lactobacilli and other aciduric microorganisms in human saliva, Dentocult® has described by Larmas (1975). � The test can be performed in a dentist's office without any special equipment. The technique also has the advantage that the result can be visualized by the patient. � This method correlates very well with the conventional selective lactobacillus agar technique (Birkhed et al 1981).

Lactobacillus Colony Count… Dentocult® - LB kit includes: � Paraffin tablet for chewing to stimulate saliva secretion � Dip-slide coated with a slight modification of Rogosa SL agar designed for the isolation of oral lactobacilli. � An evaluation chart which shows numbers of lactobacilli per ml saliva in four classes � A cup or tube � A funnel � An incubator

Lactobacillus Colony Count… The person chews A piece of paraffin at least one minute. The saliva is then spat out in a cup or tube. The collected saliva is poured over both sides of the slide, the excess let to drip off.

Lactobacillus Colony Count… Insert the slide into its plastic tube, and tighten it. Incubate at 37°C for 4 days. After 4 days, the number of adherent colonies on the slide is compared with the chart.

Lactobacillus Colony Count… Colony Density, CFU/ml
 is based")
Colorimetric Snyder Test � This simple colorimetric test devised by Snyder (1951) is based upon the rate of acid production when a sample of stimulated saliva is inoculated into a glucose and agar containing medium at p. H 4. 7 -5. � The medium contains a color indicator, bromocresol green, which changes from blue-green at p. H 4. 7 -5. 0 to yellow at p. H 4. � This test essentially estimates the number of both aciduric and acidogenic organisms in saliva because it relies on the production of additional acid under already acidic culture conditions. (Snyder et al, 1962)

Colorimetric Snyder Test… Procedure � 0. 2 ml stimulated saliva collected by chewing paraffin before breakfast is thoroughly mixed with 10 ml melted agar-containing medium in a test tube, allowed to solidify and then incubated at 37°C. � The amount of acid produced by the oral acidogenic flora is detected by the changes in the p. H indicator. and is compared to an uninoculated control tube after 24, 48 and 72 h of incubation.

Colorimetric Snyder Test… The classical formula of the Snyder agar per litre of purified water: � Pancreatic digest/casein: 13. 5 gm � Yeast extract: 6. 5 gm � Dextrose: 20 gm � Sodium chloride: 5 gm � Agar: 16 gm � Bromocresol green: 0. 029 gm

Colorimetric Snyder Test… � Tube 1: uninoculated snyder tube � Tube 2: no color change indicates no caries activity � Tube 3 : slight color change indicates mild caries activity � Tube 4: significant color change indicates moderate caries activity � Tube 5: complete color change indicates marked caries activity.

Colorimetric Snyder Test… Time in Hours 24 48 72 Color Yellow Caries Activity Marked Definite Limited Color Green Caries activity Continue test Inactive

Colorimetric Snyder Test… � One advantage of the Snyder test is its relative simplicity. � The test correlates well with the lactobacillus colony count and with the number of existing open lesions. � No test is foolproof in predicting, with a high degree of reliability, the expected caries increment for an individual. However, this test is of value in assessing the oral environmental cariogenic challenge.

Colorimetric Snyder Test… � Thus, a persistently high lactobacillus count or a persistently rapid rate of acid formation as in the Snyder test suggests that the environmental potential for caries development is present, whereas negative results suggest a low environmental challenge. Disadvantage 1) 2) Time consumed is more. Sometimes the color change is not that clear.

S. mutans Colony Count � Although lactobacilli were considered as prime etiologic agents for dental caries during that period, Clarke (1924), detected S. mutans at the front of the histological lesion of dentinal caries, whereas lactobacilli were isolated from the body of a lesion. � First was the classic experiment of Orland et al. in 1955 in which caries was induced in rats associated with a Streptococcus strain. � This was soon followed by a series of experiments by Fitzgerald Keyes and Van Houte 1980, which showed that caries in rodents was a transmissible disease caused by streptococci.

S. mutans Colony Count… � Similar strains were subsequently isolated from man and were found to be identical with the species S. mutans previously described by Clarke (1924). � Besides its strong acidogenic potential, mutans streptococci produce glucan, a major virulence factor not synthesized by other oral streptococci. � The importance of this glucan for the formation of a waterinsoluble plaque matrix in promoting the accumulation of mutans streptococci on human teeth and colonization of other organisms in supragingival plaque was reviewed by Guggenheim (1970) and Van Houte (1983).

Streptoccocus mutans Levels in Saliva � S. mutans is reported to be associated with a high risk for initiation of coronal caries and the presence of incipient smooth surface lesions. (Klock and Krasse, 1977, Kohler and Bratthall, 1979) � The frequency of isolation of S. mutans is high prior to initiation of lesions as contrasted to the lactobacilli which have a predilection for existing carious lesions. � This is an important reason why several clinics utilize S. mutans counts as an adjunct in caries management.

Streptoccocus mutans Levels in Saliva… Efforts to develop a S. mutans caries activity test run into the same problems as posed by other microbiological tests. � There is, first, the difficulty of distinguishing between a carrier state and a cariogenic infection. � Another problem relates to the finding that S. mutans may constitute less than 1% of the total flora of plaques, these concentrations can be extremely variable, with as much as a 100 fold difference between samples from the same site. (Duchin and Van Houte, 1978) � Also, S. mutans tends to be located at specific sites only, salivary counts neither pinpoint its location on teeth or estimate its degree of infection at a given site. �

S. mutans Dip Slide Method � This test classifies salivary samples according to estimates of S. mutans colonies growing on modified MSA. � In this method, the stimulated saliva is collected for five minutes and is poured over the agar coated plastic slide, completely wetting the surface and the excess allowed to drain off. � After the slides are dry two disks containing 5 gm bacitracin are placed in the middle of the inoculated agar about 20 mm from each other.

S. mutans Dip Slide Method… � The slide is then incubated in a tube containing CO 2 tablet for 48 hrs. � A zone of inhibition 10 -20 mm in diameter is formed around each bacitracin disk. � If present S. mutans appears as small blue colonies growing within the zone of inhibition � The colony density is compared to a model chart and classified as: 0 - negligible 1 - less than 100, 000 S. mutans CFU/ml of saliva 2 - 100, 000 -1000, 000 S. mutans CFU/ml of saliva 3 – more than 1000, 000 S. mutans CFU/ml of saliva

Dentocult® SM Strip Mutans Kit � Paraffin tablet for chewing � Strip selective broth Bacitracin � An incubator � An evaluation chart which shows numbers of mutans streptococci in four classes

Dentocult® SM Strip Mutans. . . Colony Density � Class 0 -1 = < 100 000 CFU/ml saliva � Class 2 = 100 000 -1. 000 CFU/ml saliva � Class 3 = > 1, 000 CFU/ml saliva Class 2 and 3 = High ”risk value”
 has an")
The Swab Test � This test developed by Grainger et al, (1965) has an advantage over the lactobacillus count and the Snyder test in that no collection of saliva is necessary. � The test is, therefore, particularly valuable in evaluating caries activity in very young children.

The Swab Test … Principle � The Swab test is based on the same principle as the Snyder test, it measures the aciduric-acidogenic component of the oral flora after a suitable incubation period by employing a color indicator in the test medium or by directly reading the p. H on a p. H meter. � In the Swab test, the oral flora is sampled by swabbing the buccal surfaces of the teeth with a cotton applicator which is subsequently incubated in the medium. � The change in p. H following a 48 -hour incubation is read on a p. H meter, or the color change is read by use of a color comparator.

The Swab Test … Interpretation : � p. H 4. 1 and < 4. 1 � p. H 4. 2 to 4. 4 � p. H 4. 5 to 4. 6 � p. H 4. 6 and over = Marked caries activity. = Active = Slightly active = Caries inactive

Interpretation of Swab Test Caries Status Swab Test Prognosis No clinical lesions Negative (tube remains green indicating no acid) No lesions No clinical lesions Positive (tube goes yellow Potential caries activity indicating acid high, incipient lesions production) likely established and may be seen radiographicaly or in a few months clinically

Interpretation of Swab Test… Caries Status Swab Test Prognosis Minor pits Negative or slightly positive Caries of developmental defects or incipient lesions possible Established lesions some in need of treatment Test positive More caries Past caries but no treatment needs Test negative None or very few lesions expected

Interpretation of Swab Test… Caries Status Swab Test Prognosis Past caries but no treatment needs Test positive New caries continuing in proportion to length of retention of sweets in mouth during the day
 � It is a colorimetric caries activity test developed")
Cariostat The Cariostat (Dentsply-Sankin, Tokyo) � It is a colorimetric caries activity test developed by Shimono and Sobue in 1974. � The cariostat test is reliable in predicting the short term caries experience in toddlers and long term caries experience in 10 yr old s.

Cariostat… � The test medium is a semi-synthetic liquid containing 20% sucrose and p. H indicators to display the continuous p. H decrease of the test medium caused by microorganisms gathered in the patient’s plaque sample. � The microorganisms in the dental plaque metabolize sucrose and produce acids that react to these p. H indicators, thus leading to colorimetric change.

The Cari. Screen Caries Susceptibility Test � The test is a simple 1 -minute chair-side bacterial test for assessing patients’ caries susceptibility. � After years of biofilm research from leading experts, we now understand that there are numerous strains of acid-producing bacteria which play a role in the caries infection. � This means we need a broad spectrum method to diagnose it, as opposed to culturing for one or two specific strains of bacteria.

The Cari. Screen Caries Susceptibility Test… � The Cari. Screen utilizes ATP bioluminescence technology to detect the levels of acid-producing, decay-causing bacteria residing in an individual’s plaque. � Adenosine triphosphate (ATP) is the energy molecule found in all cells. A common characteristic among acid-producing bacteria is that they contain up to 100 times more ATP than non-acid-producing strains. � When this ATP is brought into contact with the unique liquid- stable, bioluminescence enzymes (luciferase) in the Cari. Screen Swab, light is emitted in direct proportion to the amount of ATP present.

The Cari. Screen Caries Susceptibility Test… � The Cari. Screen Meter measures the amount of light generated in this reaction and provides information about the potential levels of cariogenic bacteria present in the biofilm. � The reading appears on the Cari. Screen Meter as a number of Relative Light Units (RLU’s) which corresponds to a healthy versus a cariogenic biofilm.
 Main Features: � Use of a somewhat softer medium")
Alban Test (Modified Snyder Test) Main Features: � Use of a somewhat softer medium that permits the diffusion of saliva and acids. � Use of simpler sampling procedure in which the patient expectorates directly into tubes that contain the medium.
… To prepare the Alban test medium the following materials")
Alban Test (Modified Synder Test)… To prepare the Alban test medium the following materials are required: � Snyder test agar � A small scale to measure 60 grams. � A 2 liter Pyrex glass to melt the medium. � A funnel to dispense the medium into test tubes. � 10 - 16 mm test tubes with screw caps.
… Scale for Scoring: 1. No colour change = ‘-’")
Alban Test (Modified Synder Test)… Scale for Scoring: 1. No colour change = ‘-’ 2. Beginning colour change (from top of medium down) = ‘+’ 3. One half colour change (from top down) = ‘++’ 4. Three fourths colour change = ‘+++’ (from top down) 5. Total colour changes to yellow = ‘++++’

Stimulated Saliva � The protective role of saliva is demonstrated by the rampant caries seen in human subjects with marked salivary hypofunction and in desalivated animals. � In normal cases, however, the relationship between saliva flow and coronal or root caries experience is doubtful and to examine the concept that stimulation of saliva might have protective effects against caries, one must look beyond a simple correlation between caries and flow rate.

Stimulated Saliva � Protective properties of saliva which increase on stimulation include salivary clearance, buffering power, and degree of saturation with respect to tooth mineral. � These benefits are maximized when saliva is stimulated after the consumption of fermentable carbohydrates by increasing the potential for remineralization.

Stimulated Saliva � Plaque acid production is neutralized and experimental lesions in enamel are remineralized, when gum is chewed to stimulate saliva after a carbohydrate intake. � The p. H-raising effects are more easily explained by the buffering action of the stimulated saliva than by clearance of carbohydrates.

Stimulated Salivary Stimulation And Plaque p. H � Plaque p. H studies provide a way of examining in the human oral cavity the effects both of salivary clearance and of buffering. � The p. H response to the ingestion of individual food items can reflect their rate of clearance and the flow rate of the saliva they elicit (Edgar et al, 1975).

Buffer Capacity Test � The buffering capacity of saliva is important for the maintenance of normal p. H levels in saliva and plaque. � Ericsson Y (1959) and Aluluusua et al (1990), reported that low secretion might indicate a low buffering capacity and a weak inverse relation to dental caries. � Both the salivary secretion and buffering capacity differ at different parts of the mouth, therefore, the composition and acidogenicity of plaque may be different when situated close to a salivary duct or hidden deep down in a fissure.

Buffer Capacity Test… � The test is quantified using either a p. H meter or color indicator. � This test measures the number of milliliters of acid required to lower the p. H of saliva through an arbitrary p. H interval, such as from p. H 7 to 6, or the amount of acid or base necessary to bring color indicators to their end point.

Buffer Capacity Test… Interpretation � There is an inverse relation between the buffering capacity of saliva and caries activity. � The saliva of individuals who have a considerable number of carious lesions, frequently have low acid-buffering capacity than the saliva of those who are relatively caries free. � Saliva samples requiring less than 0. 45 ml of standard acid in this test have low buffer capacity and those requiring 0. 45 ml or more have high buffer capacity.
 Procedure § One drop")
Buffer Capacity Test… Dentobuff Strip Test (Ericson and Bratthal, 1998) Procedure § One drop of stimulated saliva is placed on a test strip containing an acid and p. H indicator. § After 5 min, till reaction between saliva and acid has taken place color of test pad is compared to color chart of p. H indicator. § This identifies saliva with low, intermediate and high buffer capacity.

Buffer Capacity Test… blue green yellow • • • Blue ≥ 6. 0 High Green 4. 5– 5. 5 Intermediate Yellow ≤ 4. 0 Low
 Principle � It is based on the fact that")
Enamel Solubility Test (Susceptibility Test) Principle � It is based on the fact that when glucose is added to the saliva containing powdered enamel, organic acids are formed. � These in turn decalcify the enamel resulting in an increase in the amount of soluble calcium in the saliva-glucose-enamel mixture. � The extent of increased calcium determined by the calcium determination instrument, is supposedly a direct measure of the degree of caries susceptibility.
… Disadvantages � Not generally suited for office procedures. �")
Enamel Solubility Test (Susceptibility Test)… Disadvantages � Not generally suited for office procedures. � Test is not simple, equipment required are complex. � High cost. � Special training is required.

Fosdick Calcium Dissolution Test Principle � This test measures the milligrams of powdered enamel dissolved in 4 hrs by acid formed when the patient’s saliva is mixed with glucose and powdered enamel. Procedure � Saliva is stimulate by having the patient chew gum or paraffin. � 25 ml of this saliva is collected and part of it is analysed for calcium content. � The remaining saliva is placed in an 8 inch sterile test tube with 0. 1 gm of powdered human enamel.

Fosdick Calcium Dissolution Test. . � The tube is sealed and shaken for 4 hrs at body temperature, after which it is again analyzed for calcium content. � The chewing of chewing gum to stimulate saliva produces sugar, if the paraffin is used 5% glucose is added. � The amount dissolution increases as the caries activity increases.

Fosdick Calcium Dissolution Test. . . Advantage � In limited studies, the correlation reported is good. Disadvantage � The test is not simple and requires complex equipments. � The test is expensive and require trained personnels.
… Evaluation Color Time Score Caries Activity Blue 15 mins")
Salivary Reductase Test (Susceptibility Test)… Evaluation Color Time Score Caries Activity Blue 15 mins 1 Non conducive Orchid 15 mins 2 Slightly conducive Red 15 mins 3 Moderately conducive Red Immediately 4 Highly conducive Pink or white Immediately 5 Extremely conducive
… Advantage � No incubation required. � Quick results. Disadvantage")
Salivary Reductase Test (Susceptibility Test)… Advantage � No incubation required. � Quick results. Disadvantage � Test results vary with time after food intake and brushing.

Oratest � Unfortunately, many of these caries activity tests requires extensive work up time and additional equipment. � Rosenberg et al in 1989 developed Oratest, a simple, economical, non-invasive and less time consuming test for estimating the oral microbial level.

Oratest… Principle � Oratest is based on the rate of oxygen depletion by micro- organisms. � Under aerobic conditions the bacterial enzyme, aerobic dehydrogenase transfers electrons or protons to oxygen. � Once oxygen gets utilized by the aerobic organisms and an anaerobic environment is attained, methylene blue acts as an electron acceptor and gets reduced to leucomethylene blue.

Caries Susceptibility Varies: � In Different Individuals, � In An Individual In Different Teeth � Also On The Different Surfaces Of Each Tooth

Caries Risk Assessment � As caries is preventable, the diagnosis of caries as a tooth lesion is not sufficient for a treatment plan. � The clinician must devise a need-related treatment plan on the basis of certain scientific diagnosis. In doing so, he or she should assess a patient’s caries risk status because it provides an estimate of future caries activity. � Risk is defined as the probability that a harmful event will occur.

Caries Risk Assessment… � The caries risk assessment is performed in order to introduce casual measures before irreversible lesions become established. � It is important first to distinguish between risk factors and risk indicators. � Risk Factor: plays an important role in the etiology of the disease. They are the lifestyle and biochemical determinants to which the tooth is directly exposed and which contribute to the development or progression of the lesion, e. g plaque, saliva, diet etc.

Caries Risk Assessment… � Risk Indicator: it is a factor or circumstance that is indirectly related to the disease, e. g socioeconomic factors (socially deprived, low education level, poor economy), factors related to general health (diseases, handicap) and epidemiological factors ( living in a high caries area).

Risk Factors RISK FACTOR Social History Medical History Fluoride Use HIGH RISK LOW RISK • Low knowledge of dental diesease • Irregular dental visits • Family: general poor oral care • Dentally aware • Regularly scheduled appointment • Low caries in siblings • Medically compromised • Disabled/ handicapped • Xerostomia as a result of medication or radiation therapy • No serious medical problem • No medications for chronic diseases • Normal salivary flow • No physical problems/ handicaps • Does not live in a fluoridated area • Use of fluoridated toothpaste but irregular brushing • Lives in fluoridated area • Lived in a fluoridated area as a small child • Use of fluoride toothpaste regularly • Weekly use of fluoride mouthrinse

Risk Factors… RISK FACTOR Dietary Habits Biofilm Control HIGH RISK LOW RISK • Frequent sugar intake • Frequent snacking • Not familiar with food guide pyramid • Chewing of tobacco occasionally • Infrequent sugar intake • Rarely snacking in between meals • Use of xylitol containing chewing gums • Irregular brushing and other oral care • Use of orthodontic appliance/ prosthesis with irregular cleaning • Poor manual dexterity or handicap • High biofilm scores • Regular brushing at least two times daily • Use of dental floss daily • No appliance use requiring regular use • No handicap • Low biofilm scores

Risk Factors… RISK FACTOR Clinical/ Oral HIGH RISK • Previous caries • Presence of new caries / white spot lesions • Multiple restorations • Unsealed deep pits and fissure • Exposed root surfaces LOW RISK • No new caries • Few restorations • Sealants in pits and fissures • Exposed root surfaces with regular fluoride application

Caries Risk Indicator Low Risk Moderate Risk • Optimal fluoride exposures • Suboptimal systemic both systemic and topical fluoride exposure with optimal topical exposure • Consumption of simple sugars limited to mealtime • Between meal snacking (12) • High caregiver socioeconomic status • Midlevel caregiver (financially stable) socioeconomic status • Regular dental visits • Irregular use of dental services High Risk • Suboptimal topical fluoride exposure • Frequent between meal snacking (3 or more) • Low level caregiver socioeconomic status • Active caries present in the mother • Children with special health care needs • Conditions decreasing saliva flow (medications)
")
Caries Risk Indicator AAPD Caries-Risk Assessment Tool (CAT)
")
Caries Risk Indicator AAPD Caries-Risk Assessment Tool (CAT)

Ages To Be Considered For Caries Risk Assessment AGE WHERE? WHY? 1 yr At child health centers To prevent nursing bottle caries, early diagnosis 3 yr At dental clinic To prevent caries in primary molars 6 -7 yr At dental clinic And schools To prevent caries in first permanent molars 12 -13 yr At dental clnics Screening in school To prevent caries in second molar and premolars.

CARIOGRAM � A new method of illustrating the interaction of factors contributing to the development of caries was introduced by Bratthal et al (1999) � It is an interactive PC program for caries risk evaluation based on the interactions between caries related factors and expresses a graphic assessment of the risk. � It is a graphical picture illustrating in an interactive way the individual's/patient's risk for developing new caries in the future, simultaneously expressing to what extent different etiological factors of caries affect the caries risk for that particular patient.

CARIOGRAM… � The Cariogram does not specify a particular number of cavities that will or will not occur in the future (D. Bratthall, 2004) � It rather illustrates a possible overall risk scenario, based on what can be expected depending on the interpretation of available information. � Cariogram as an interactive PC-program has been developed for educational, preventive and clinical purpose. � It does not take over the judgement or the responsibilities of the examiner, but may serve as a valuable tool in the clinical decision-making.

CARIOGRAM… Factors Considered � Factors immediately involved in the caries process, either as ‘attack’ or ‘defence’ mechanisms, at the site of the development of the lesion. 1. On the attack side, the dental plaque, the presence of various specific microorganisms in the plaque (including mutans streptococci) and the diet can be included. 2. On the defence side for example, the salivary protective systems and the fluoride exposure can be incorporated.

CARIOGRAM… � Factors related to the occurrence of caries, without actually participating in the development of the lesion, for example various socio-economic factors and past caries experience are added. � Cariogram is both a risk model and a prediction model because it acts as a prediction model that predicts who is at high risk and it is a risk model identifying the risk factors to facilitate preventive intervention.

CARIOGRAM… Method � Information on a these factors are collected about the patient � Transferred to scores � These scores are then entered into the program � The build-in-algorithm program evaluates the data and presents the summarized result expressed as one figure- a pie diagram
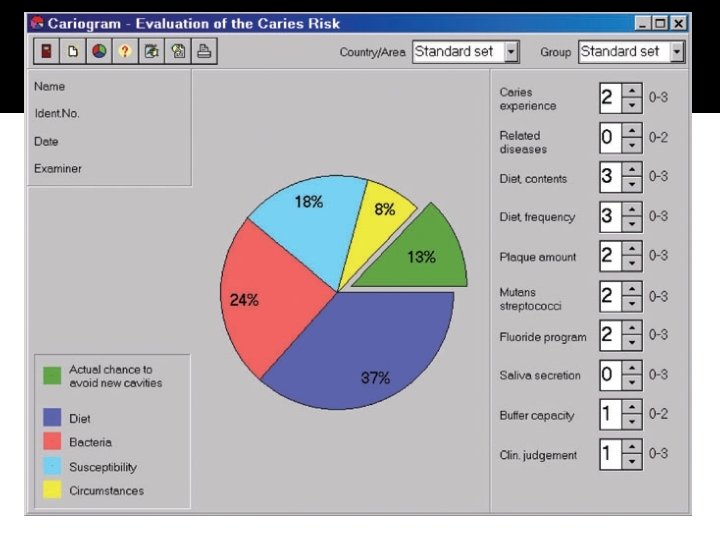

A pie circle diagram is divided into 5 sectors the following colours. � Green: Shows an estimation of the ‘chance to avoid caries’. � Dark Blue: Diet is based on a combination of amount of diet contents and diet frequency. � Red: Bacteria is based on a combination of amount of plaque and mutans streptococci. � Light Blue sector: Susceptibility is based on a combination of fluoride programs, saliva secretion and saliva buffer capacity. � Yellow sector: Circumstance is based on a combination of past caries experience and related diseases.

Chairside Diet Assessment Of Caries Risk… Counseling Strategies � Although oral health care professionals can identify patients’ food or beverage selections and dietary habits that increase their risk of developing caries, patients are responsible for changing their behaviors. � Oral health care professionals can only provide recommendations, however, the manner in which those recommendations are provided will improve the patient’s receptivity. � Knowledge of patient’s understanding of diet-disease relationships and motivation to change help the oral health care practitioners to tailor recommendations for each patient.

Thank You
- Slides: 88