Care Redesign Population Health Beth Averbeck MD Senior

Care Redesign & Population Health Beth Averbeck, MD Senior Medical Director, Primary Care, Health. Partners Chris Kodl, MD Division Medical Director, Endocrinology, Health. Partners This presentation is provided free-of-charge and is supported by Grant Number 1 L 1 CMS-331480 -01 -00 from the U. S. Department of Health & Human Services, Centers for Medicare & Medicaid Services. The contents provided in this webinar are solely the responsibility of the presenters and do not necessarily represent the official views of HHS or any of its agencies.

Beth Averbeck, MD Currently serves as Health. Partners’ Senior Medical Director of Primary Care. Her areas of expertise include total cost of care, physician culture, reliability in ambulatory care and reducing disparities. She is past chair of the Quality Council of the American Medical Group Association, a board member and past chair for Minnesota Community Measurement and board vice chair of the Institute for Clinical Systems Improvement. Chris Kodl, MD Currently serves as Health. Partners’ Division Medical Director, Med Subspecialties and Department Chair of Endocrinology. He is interested in all fields of Endocrinology including diabetes, osteoporosis, calcium disorders, thyroid disease, pituitary disease, adrenal disease and hormone problems. He is committed to delivering quality care to each patient he sees.

Consumer-governed, non-profit Integrated health care delivery and financing Clinics and hospitals Health plan Twin Cities & surrounding communities (MN & Western WI) Health. Partners Medical Group – Primary Care: • 500, 000 patients • 29 locations • 400 physicians • Mixed payer population

Why Redesign? • Inconsistent results for unsustained periods of time • Poor patient access • Unexplained variation • Financial pressures for increased productivity • EHR implementation • Community transparency • AMGA 25 th percentile in physician satisfaction 2005

Care Design Work to standardize clinic workflows “The right person doing the right thing at the right time with the right patient experience. ” “Standardize to the science, customize with the patient. ”

Care Design Principles We use the following design principles to ensure our care achieves Triple Aim (health, experience, affordability) results: Reliability Reliable processes to systematically deliver the best care Customization Access Care is customized Easy, convenient to individual needs and affordable and values access to care and information Coordinated care across sites, specialties, conditions and time

Care Model Process Before The Visit Scheduling Reception • Insurance verification • Check-in • Scheduling • Message triage • Forms Pre-visit Planning CMA/LPN • Registry • Message triage • LPN standing orders • Test results • Immunization During the Visit Check-in RN’s Visit • Phone triage • Protocol driven care • Warfarin management • Medication refill • Abnormal test triage • Care Coordination • Action Plan After the Visit Between Visits Follow-up Between Visits Clinician • Leader of care team • Diagnosis and treatment • Engaging patients in their care • Directing members of care team • Care plans

Care Model Process: Upgrades • Clinic upgrade training sessions 2 X yearly - Two, 4 hour sessions Re-evaluate & reduce Improvement requires change Train everyone!

Case Example: Approach to Diabetes Care • Teamwork is a key skill – Specific roles and responsibilities – Delegate and trust – Proactively identify patients (registry work) – Reach out to patients who need to come in for a visit or need support between visits • Increasing use of technology – e. visits and scheduled telephone visits (STV) – tele-health • Engage patients in healthy lifestyle choices (‘health coaching’) • Standing orders for pharmacists and diabetes nurse specialists

Patient With Diabetes Vs. “Diabetic” Medication List 45 total medications: • 4 hypertension • 2 lipid • aspirin • 2 glycemic • 5 mental health • 7 topical John Smith, Patient History • • • Hyperlipidemia DM Type 2 Pain Low Back Obstructive Sleep Apnea Hypopnea Schizophrenia NOS Depression Major NOS Hemorrhoids Internal NOS Gastroesophageal Reflux Disease Obesity Morbid Psoriasis Atypical chest pain

Care Model Process: Includes Diabetes During the Visit Before The Visit Scheduling Reception • Contact patients to schedule Pre-visit Planning CMA/LPN Check-in • Registry • Standing orders for Hb. A 1 c, LDL test • Preventive services • Collaborative documentation & template for diabetes Visit RN’s • Care coordination • Action plan • Health coaching • Support for newly diagnosed patients (same day) • Post hospital discharge support After the Visit Between Visits Follow-up Between Visits Clinician • Leader of care team • Diagnosis and treatment • Engaging patients in their care • Directing members of care team • Care plans

Diabetes “Neighborhood” Care Team Registered Dietitian Nutritionist Diabetes Nurse Specialist • • Patient Matching meter to coverage Medication adjustment Help with registries Support behavior change • Balancing eating and activity with medication and monitoring Pharmacist • • Lipids Blood pressure Poly pharmacy Medication coverage and cost Clinician System support: Lab standing orders & EHR decision support *Diabetes Nurse Specialists and Dietitian Nutritionists can both be Certified Diabetes

Role of Specialist • Referrals – Glycemic control • • • Primary management of patients with Type I Co-management Population consultant Endocrine Hotline (for clinicians/staff only) Content expert

Population Consultant Moving knowledge and information, not patients A new approach to diabetes care in Endocrinology: • Share knowledge and best practices through the use of tele-video • Discuss difficult diabetes cases with experts and other providers • Build relationships with colleagues *Modeled after Project ECHO

Measurement: Optimal Diabetes Care Measure: Optimal Diabetes Care - % of patients ages 1875 with diabetes who have the following: • • • Statin use or LDL < 70 (patients > 40 years) A 1 c with a value less than 8. 0 Blood pressure less than 140/90 Documented non-tobacco user Aspirin use (vascular disease) *NQF Endorsed

Using Data as Information Transparency What Data is Our Patients are Measuring Wrong Sicker the wrong condition Data could be right Data is never perfect and it’s good enough
: Optimal Diabetes Care")
2016 Minnesota Community Measurement (MNCM): Optimal Diabetes Care

Clinic/Clinician Results Health. Partners Medical Group Optimal Diabetes Care March 2016 Summary Report
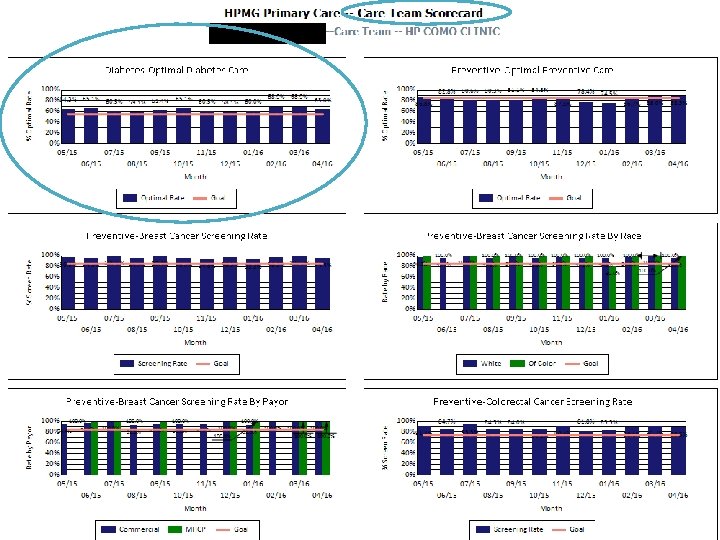

Care Team Scorecard Meetings Structure Process Site Leaders send plans to division leaders • Meet every 90 days with site leadership • Physician/Clinician, LPN/CMA, RN • Celebrate & share • Identify opportunities and learn • Test improvements: care teams and leaders partner • Identify best practices • Reward and recognize • Share with others

Care That Meets The Needs of The Person Equality Equity

Customization Cultural specific diet Support during Ramadan Preservation vs. threat of loss

Standardization Improves Care Optimal Diabetes Care 60% 52% 50% 46% 40% 38% 30% 20% 10% patients who are white patients of color MHCP (public programs) 4 Q 16 3 Q 16 2 Q 16 1 Q 16 4 Q 15 3 Q 15 2 Q 15 1 Q 15 4 Q 14 3 Q 14 2 Q 14 1 Q 14 3 Q 13 4 Q 13 2 Q 13 1 Q 13 4 Q 12 3 Q 12 2 Q 12 1 Q 12 4 Q 11 3 Q 11 1 Q 11 2 Q 11 4 Q 10 3 Q 10 2 Q 10 1 Q 10 4 Q 09 3 Q 09 2 Q 09 1 Q 09 4 Q 08 3 Q 08 2 Q 08 1 Q 08 4 Q 07 3 Q 07 2 Q 07 1 Q 07 0% non-MHCP Measure: % of HPMG patients with diabetes have statin on current medication list (or LDL <70 for patients >40), have had an A 1 c in the last 12 months with a value <8. 0, last recorded blood pressure <140 and <90, documented non-tobacco user and documented regular aspirin user.

Saves 343 hearts, 51 legs & 810 pairs of eyes each year 80 70% 70 60% 50 40% 40 30% 30 Optimal Diabetes % Events/1000 60 20% 20 10 10% 0 0% 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 AMI/1000 AMPUTATIONS/1000 NEW RETINOPATHY CASES/1000 OPTIMAL DIABETES RATE Health. Partners’ 35, 601 members with diabetes in 2015 suffered 343 fewer heart attacks, 51 fewer leg amputations and 810 people did not experience eye complications compared to what would have happened to the same 35, 601 plus members in 2000.

AMGA Physician Satisfaction Survey 2005 Preauthorization Dimension Percentile Ranking 75 th Quality Colleagues Computers Compensation 50 th Resources Compensation Leadership 25 th 2005 Staff Patients Admin Time Working AMGA Correlation with Overall Satisfaction

AMGA Physician Satisfaction Survey 2016 Colleagues Preauthorization Paper Work Staff Quality Resources Leadership Administrators Computers Compensation Dimension Percentile Ranking 75 th Patients Time Working 50 th 25 th 2016 AMGA Correlation with Overall Satisfaction Health. Partners

Contact Information Beth Averbeck, MD Beth. M. Averbeck@healthpartners. com Chris Kodl, MD Christopher. T. Kodl@healthpartners. com

Thank You!
- Slides: 29