CARE OF PRETERM AND POSTTERM INFANTS BSN 4

CARE OF PRE-TERM AND POST-TERM INFANTS BSN – 4 C RLE GROUP 2 IAN V. SUMAGAYSAY, MAN, RN FACILITATOR

ANATOMY AND PHYSIOLOGY OF NORMAL PREGNANCY

IMPORTANT TERMS: GRAVIDITY Gravida: woman who is pregnant Gravidity: pregnancy Multigravida: woman who has had two or more pregnancies Multipara: woman who has completed two or more pregnancies to stage of fetal viability Nulligravida: woman who has never been pregnant

IMPORTANT TERMS: PARITY • Parity: number of pregnancies in which fetus or fetuses have reached viability, not the number of fetuses born • Nullipara: woman who has not completed pregnancy with a fetus or fetuses who have reached the stage of fetal viability • Primipara: A woman who has completed one pregnancy with a fetus or fetuses who have reached 20 weeks of gestation • Multipara: A woman who has completed two or more pregnancies to 20 weeks of gestation or more

IMPORTANT TERMS: GESTATIONAL AGE OF PREGNANCY • Preterm: a pregnancy that has reached 20 weeks of gestation but ends before completion of 37 weeks of gestation • Late preterm: a pregnancy that has reached between 34 weeks 0 days and 36 weeks 6 days of gestation • Early term: a pregnancy that has reached between 37 weeks 0 days and 38 weeks 6 days of gestation • Full term: a pregnancy that has reached between 39 weeks 0 days and 40 weeks 6 days of gestation • Late term: a pregnancy that has reached between 41 weeks 0 days and 41 weeks 6 days of gestation • Post term: a pregnancy that has reached between 42 weeks 0 days and beyond of gestation
")
ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Pregnancy Tests Ø Human chorionic gonadotropin (h. CG) – is the earliest biochemical marker for pregnancy Ø Production of h. CG begins as early as the day of implantation Ø In urine, about 26 days after conception Ø Level of h. CG increases until it peaks at about 60 to 70 days of gestation Ø Remains stable until about 30 weeks and then gradually increases until term Ø Higher than normal levels of h. CG may indicate ectopic pregnancy, abnormal gestation, or multiple gestation Ø Abnormally slow increase or decrease in h. CG levels may indicate impending miscarriage

SIGNS OF PREGNANCY Ø Adaptations of Pregnancy Ø Signs of Pregnancy Ø Presumptive Ø Changes felt by the woman Ø Probable Ø Changes observed by an examiner Ø Positive Ø Those signs that are attributed only to the presence of the fetus

ADAPTIONS TO PREGNANCY Ø Reproduction System and Breasts Ø Uterus Ø Changes in Size, Shape, and Position Ø Phenomenal uterine growth in the first trimester is stimulated by high levels of estrogen and progesterone Ø 7 weeks of gestation- is the size of a large hen’s Egg Ø 10 weeks gestation-is the size of an orange (twice nonpregnant size) Ø 12 weeks of gestation-is the size of a grapefruit Ø Pregnancy may “show” after 14 weeks

ADAPTIONS TO PREGNANCY • Lightening • Hegar Sign • At approximately 6 weeks of gestation, softening and comprehension of the lower uterine segment • Uterine fundus presses on the urinary bladder causing the woman to have urinary frequency

A NURSE EMPLOYED IN A PRENATAL CLINIC NOTES PHYSICIAN DOCUMENTATION IN A CLIENT’S CHART THAT INDICATES THE PRESENCE OF HEGAR’S SIGN IN THE CLIENT. THE NURSE UNDERSTANDS THAT THIS SIGN INDICATES THAT: 1. The mother is feeling fetal movement 2. The client is complaining of irregular, painless contractions 3. A soft blowing sound was heard when the uterus was auscultated 4. Lower uterine segment thinning is present

ADAPTIONS TO PREGNANCY ØChanges in Contractility ØBraxton Hicks sign- Soon after the fourth month of pregnancy, uterine contractions can be felt through the abdominal wall ØContractions are irregular, painless, and occur intermittently throughout pregnancy

ØContractions facilitate uterine blood flow through the intervillous space of the placenta ØContractions are painless, some women complain that they are annoying ØAfter the 28 th week, these contractions become more definite ØCan be mistaken for true labor

ADAPTIONS TOPREGNANCY ØUteroplacental Blood Flow Ø Placental perfusion depends on the maternal blood flow to the uterus Ø Blood flow increase rapidly as the uterus increase in size Ø Normal term pregnancy, one sixth of the total blood volume is within the uterine vascular system Ø Rate of blood flow through the uterus average from 450 to 650 ml/min at term

ADAPTIONS TO PREGNANCY Ø Cervical Changes Ø Softening of the cervical tip may be observed about the beginning of the sixth week Ø Goodell's sign is brought about by the increase vascularity, slight hypertrophy, and hyperplasia (increase in number of cells) Ø Muscle and its collagen-rich connective tissue become loose, edematous, high-elastic, and increase in volume

ØGlands near the external os proliferate beneath the stratified squamous epithelium, giving the cervix consistency characteristic of pregnancy ØFriability is increased; that is the cervix bleeds easily when scraped or touched

A NURSE IS REVIEWING THE RECORD OF A CLIENT WHO HAS JUST BEEN TOLD THAT A PREGNANCY TEST IS POSITIVE. THE NURSE NOTES THAT THE PHYSICIAN HAS DOCUMENTED THE PRESENCE OF GOODELL’S SIGN. THE NURSE DETERMINES THAT THIS SIGN IS INDICATIVE OF: 1. The presence of fetal movement 2. A soft blowing sound that corresponds to the maternal pulse while auscultating the uterus 3. The presence of human chorionic gonadotropin (h. CG) in the urine 4. A softening of the cervix

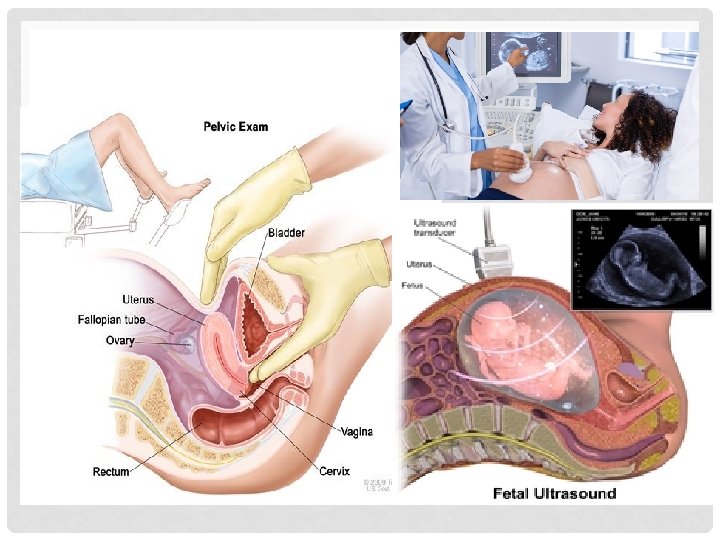
ANATOMY AND PHYSIOLOGY OF PREGNANCY • Changes related to the presence of the fetus Ø Ballottement- passive movement of the unengaged fetus Ø Can be identified generally between the sixteenth and eighteenth week • Technique of palpating a floating structure by bouncing it gently and feeling it rebound • Palpate the fetus • Examiner places a finger within the vagina and taps gently upward causing the fetus to rise • Fetus sinks, • And a gentle tap is felt on the finger

ADAPTATIONS TO PREGNANCY

ADAPTIONS TO PREGNANCY Ø Vagina and Vulva Ø Chadwick sign-increased vascularity results in a violet -bluish color of the vagina mucosa and cervix Ø Leukorrhea- is a white or slightly gray mucoid fluid occurs in response to cervical stimulation by estrogen and progesterone

ØMucus fills the endocervical canal, resulting in the formation of the mucous plug Øp. H of vaginal secretions is more acidic during pregnancy, ranging from 3. 5 to 6. 0 ØResult of increased production of lactic acid caused by Lactobacillus acidophilus acting on glycogen in the vaginal epithelium

A PREGNANT CLIENT CALLS THE NURSE AT THE HEALTH CARE CLINIC AND REPORTS THAT SHE HAS NOTICED A THIN, COLORLESS, VAGINAL DRAINAGE. THE NURSE MOST APPROPRIATELY TELLS THE CLIENT: 1. To come to the clinic immediately 2. That this is a normal occurrence during pregnancy 3. To douche once daily 4. To use tampons if the discharge is bothersome

ADAPTIONS TO PREGNANCY ØBreast ØFullness, heightened sensitivity, tingling, and heaviness of the breasts ØNipples and areolae become more pigmented, secondary pinkish areolae develop ØColostrum- the creamy, white-to-yellowish to orange pre-milk fluid

ADAPTIONS TO PREGNANCY

A NURSE IS PROVIDING INSTRUCTIONS TO A PREGNANT CLIENT IN THE THIRD TRIMESTER OF PREGNANCY REGARDING MEASURES TO ASSIST IN REDUCING BREAST TENDERNESS. THE NURSE TELLS THE MOTHER TO: • 1. Avoid wearing a bra • 2. Wash the nipples and areola area daily with soap • 3. Wear tight-fitting blouses or dresses to provide support • 4. Wear soft-textured clothing
 Heart")
ADAPTIONS TO PREGNANCY ØGeneral Body System ØCardiovascular System Ø Slight cardiac hypertrophy (enlargement) Heart returns to normal after childbirth Ø Diaphragm is displaced upward by the enlarging uterus Ø Between 14 and 20 weeks of gestation the pulse increase about 10 to 15 beats/min Ø Palpitations may occur
 is")
ANATOMY AND PHYSIOLOGY OF PREGNANCY ØBlood Pressure Ø Arterial blood pressure (brachial artery) is affected by age, activity level, presence of health problems, and the circadian rhythm Ø Diastolic blood pressure usually remains the same as the prepregnancy level but then gradually decreases until 24 to 32 weeks Ø After 32 weeks, the diastolic blood pressure gradually returns to normal

ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Blood Volume and Composition Ø Blood volume increases by approximately 1200 to 1500 ml Ø Increase consists of 1000 ml of plasma plus 450 ml red blood cells (RBCs) Ø Blood volume starts to increase at about the tenth to twelfth week Ø Plasma increases exceeds the increase in the RBC production Ø Total white cell count increase during the second trimester and peaks during the third trimester

ANATOMY AND PHYSIOLOGY OF PREGNANCY ØCardiac Output ØCardiac output increases from 30% to 50% over the nonpregnant rate by the thirty-second week of pregnancy ØCirculation and Coagulation Times Ø Circulation time decreases slightly by week 32

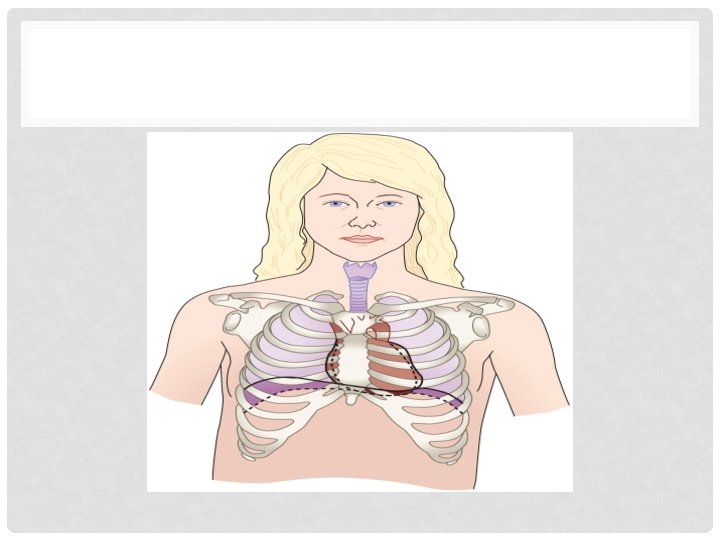
ANATOMY AND PHYSIOLOGY OF PREGNANCY ØRespiratory System Ø Maternal oxygen requirements increase in response to the acceleration in the metabolic rate and the need to add to the tissue mass in the uterus and breasts Ø Upper respiratory tract becomes more vascular in response to elevated levels of estrogen Ø Congestion within the tissues of the respiratory tract gives rise to several conditions commonly seen during pregnancy

ANATOMY AND PHYSIOLOGY OF PREGNANCY ØPulmonary Function Ø Respiratory changes in pregnancy are related to the elevation of the diaphragm and chest wall changes Ø Pregnant women become more aware of the need to breathe; some may even complain of dyspnea at rest, especially in the third trimester
 Ø BMR varies considerably in")
ANATOMY AND PHYSIOLOGY OF PREGNANCY ØBasal Metabolic Rate (BMR) Ø BMR varies considerably in women at the beginning of and during pregnancy Ø BMR returns to nonpregnant levels by 5 to 6 days after birth Ø Pregnant women may experience heat intolerance Ø Lassitude and fatigability after only slight exertion are experienced by many women in early pregnancy Ø Greater need to sleep

ANATOMY AND PHYSIOLOGY OF PREGNANCY ØAcid-Base Balance ØAlterations in acid-base balance indicate that the pregnancy is a state of respiratory alkalosis compensated by mild metabolic acidosis ØChanges also facilitate the transport of CO 2 from the fetus and O 2 release from the mother to the fetus

ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Fluid and Electrolyte Balance Ø Pooling of fluid in the legs latter pregnancy decreases renal blood flow Ø Pooling of blood in the lower legs is sometimes referred as to physiologic edema or dependent edema and requires no treatment Ø In pregnant women, however, tubular reabsorption of glucose is impaired Ø Proteinuria usually does not occur in normal pregnancy except during labor or birth

ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Integumentary System Ø Chloasma- facial melasma Ø Usually fades after birth Ø Linea nigra- is a pigmented line extending from the symphysis pubis to the top of the fundus in the midline Ø Striae gravidarum- or stretch marks seen over the abdomen Ø Birth they usually fade, although they never disappear completely
-are tiny, star-shaped")
ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Integumentary System Ø Vascular spiders (angiomas)-are tiny, star-shaped or branched Ø Bluish in color and do not blanch with pressure Ø Palmar erythema-pinkish-red, diffuse mottling or well-defined blotches that are seen over the palmar surfaces of the hands Ø Cholestasis of pregnancy-the most common cause of pruritic rash Ø Epulis- a red, raised nodule on the gums that bleeds easily Ø Nail growth may be accelerated Ø Hirutism- excessive growth of hair or growth of hair in unusual places

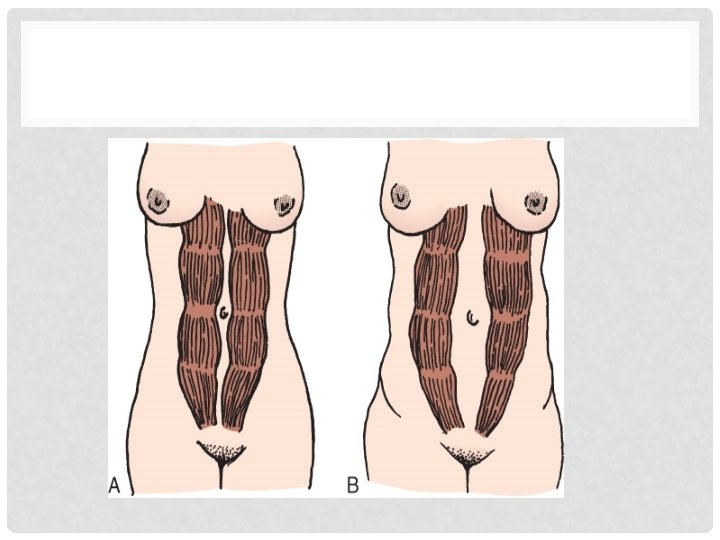
ANATOMY AND PHYSIOLOGY OF PREGNANCY Ø Musculoskeletal System Ø Walking is more difficult, and the waddling gait of the pregnant woman called “the proud walk of pregnancy” Ø Ligamentous and muscular of the middle and lower spine may be severely stressed

ANATOMY AND PHYSIOLOGY OF PREGNANCY • Neurologic System • Edema involving the peripheral nerves, which may result in carpal tunnel syndrome • Tension headache is common when anxiety or uncertainty complicates pregnancy • “Light-headedness”, faintness, and even syncope are common during early pregnancy • Hypocalcemia may cause neuromuscular problem such as muscle cramps and tetany

ANATOMY OF PHYSIOLOGY AND PREGNANCY Ø Gastrointestinal System Ø Appetite Ø Morning sickness or nausea and vomiting of pregnancy appears at about 4 to 6 weeks of gestation and usually subsides by the end of the third month Ø Pica- nonfood cravings, such as for ice, clay, and laundry starch Mouth Ø Pytalism- excessive salvation, which may be caused by the decrease in unconscious swallowing by the woman when nauseated or from stimulation of salivary glands by eating starch Esophagus, Stomach, Intestines, Ø Pyrosis- “Acid Indigestion” or heartburn Ø Constipation Ø Pregnant woman has hemorrhoids

TEXTBOOK DISCUSSION ØPRE TERM INFANT Classifications: Ø Premature infant or Preterm birth Ø neonates born at less than 37 weeks' gestation Ø leading cause of neonatal mortality Ø most common reason for antenatal hospitalization Ø three primary causes of mortality: respiratory failure, infection, and Late Preterm- born between 34 and 36 weeks of pregnancy Moderately Preterm- born between 32 and 34 weeks of pregnancy congenital malformation Very Preterm- born at less than 32 weeks of pregnancy Extremely preterm- born at or before 255 weeks of pregnancy

RISK FACTORS FOR PRETERM BIRTHS • • • Age of mother Previous Early birth Closely spaced pregnancies Decidual Hemorrhage Lifestyle and Environmental Factors • Multiple gestation • History of abortion • • • Polyhydramnios Infections Cervical insufficiency Shorter cervical length Ethnicity Medical conditions

SIGNS AND SYMPTOMS OF PRETERM LABO ØChange in type of vaginal discharge (watery, mucus or bloody) ØIncrease in amount of discharge ØPelvic or lower abdominal pressure ØConstant low, dull backache ØMild abdominal cramps, with or without diarrhea ØRegular or frequent contractions or uterine tightening, often painless Ø Ruptured membranes

ØPOST TERM INFANT Ø An overly mature baby that has not been born until well after the usual term pregnancy. A post-term baby is one born 2 weeks (14 days) or more after the usual 9 months (280 days) of gestation. Ø "postdate infant" and "postmature infant"

RISK FACTORS FOR POST TERM BIRTHS Ø Advanced maternal age (35 y. o & above) Ø Primigravidas Ø Obesity Ø History of Post term pregnancy (27% with one prior prolonged pregnancy and 39% with 2 prior prolonged pregnancies) Ø Genetic Predisposition(relative risk is 1. 3) Ø Inaccurate dating Ø Male fetus (3: 2)

POST TERM PREGNANCY COMPLICATIONS Fetal Macrosomia -an infant who is over 8 pounds, 13 ounces when born. Placental Insufficiency -also known as uteroplacental vascular insufficiency, occurs when the placenta fails to deliver adequate oxygen and nutrients to the infant. Meconium Aspiration -is marked by an infant breathing in amniotic fluid and meconium (newborn feces) shortly after birth.

DEFINITION Ø URINARY TRACT INFECTION Ø defined as significant bacteriuria in the presence of a constellation of symptoms such as dysuria (painful urination), increased urinary frequency and urgency, suprapubic discomfort and costovertebral angle tenderness. Ø It is a common cause of infections, particularly among young, sexually active women; an estimated 1 in 3 women will develop a urinary tract infection before the age of 24 years.

SCHEMATIC DIAGRAM

SIGNS AND SYMPTOMS PREMATURE Integumentary • Thin, smooth, shiny skin that is often transparent (can see veins under skin) • Soft, flexible ear cartilage • Newborn jaundice • Body hair (lanugo) In mother • Contractions every 10 minutes or more often • Backache, usually in lower back Respiratory • Neonatal respiratory distress syndrome, extra air in the tissue of the lungs Neurological • Bleeding into the brain or damage to the • (pulmonary interstitial emphysema), or bleeding in the lungs (pulmonary brain's white matter • hemorrhage) • Lack of reflexes for sucking and • Problems breathing due to immature lungs, swallowing, leading to feeding pneumonia, patent ductus arteriosus. difficulties • Abnormal breathing patterns (shallow, irregular pauses in breathing called apnea)

Cardiovascular • Patent ductus arteriosus In mother • Flu-like symptoms such as nausea, vomiting, or diarrhea Gastrointestinal • Lower muscle tone and less activity than full-term infants • Problems feeding due to trouble sucking or coordinating swallowing and breathing • Severe intestinal inflammation (necrotizing enterocolitis) • In mother • Flu-like symptoms such as nausea, vomiting, or diarrhea Reproductive • Enlarged clitoris (in female infants) • Small scrotum that is smooth and has no ridges, and undescended testicles (in male infants) • In mother • Cramping in the lower abdomen or menstruallike cramps • Fluid leaking from your vagina • Bag of water breaks • Increased pressure in your pelvis or vagina Musculoskeletal • Less body fat can lead to low body temperature, • Small size, with a disproportionately large head Lymphatic • Infection or neonatal sepsis Hematologic • Anemia • Low blood sugar (hypoglycemia)

Postmature Integumentary Reproductive • • In mother • A reduced volume of amniotic fluid may cause a reduction in the size of the uterus. • Meconium-stained amniotic fluid may be seen when the membranes have ruptured • Dry, loose, peeling skin Overgrown nails Abundant scalp hair Visible creases on palms and soles of feet Green, brown, or yellow coloring of skin from meconium staining (the first stool passed during pregnancy into the amniotic fluid) Neurological • More alert and "wide-eyed" Musculoskeletal • Minimal fat deposits • Decreased amount of soft-tissue mass • In mother • Before delivery there may be reduced fetal movement.

CLIENT ASSESSMENT DATA BASE

LIFESTYLE INFORMATION • Activity/Rest She lives in a third floor condominium and uses stairs in the morning when going to work as her morning exercise. She works long periods of standing as a secretary for a university president. • Circulation During physical examination her Blood Pressure was 130/80 and history reveals that she had sudden palpitations during her work. • Elimination The frequency of her bowel movement is 2 -3 times a day with watery stools. • Food/Fluid She loves to eat spicy foods and dark leafy vegetables, eggplant, squash, celery, green peas and tomatoes. And can consume 2 -3 bottles of alcoholic drinks as her stress reliever.

LIFESTYLE INFORMATION • Pain/Discomfort She had symptoms of urinary tract infection for the past few and she noticed some mild abdominal pain and thought it was irritation from the bladder infection. • Respiration Physical assessment reveals that her respiratory rate is 22 breaths per minute and her manner of breathing deep and shallow with the use of accessory muscles noted. • Safety She accidentally slipped in the bathroom while taking a bath because she's in hurry to go to work but no bleeding occurs. • Teaching/Learning She so does not go on a her regular schedule for prenatal check-up

TESTS AND DIAGNOSIS FOR PREMATURE BIRTHS

Uterine Monitoring

• Lab tests • Maturity amniocentesis Tests and diagnosis for postmature births: • Menstrual History • Fetal Ultrasonography • Ballard Score

MANAGEMENT 1. MEDICAL INTERVENTIONS Premature Post mature a. Mother b. Infant

2. PHARMACOLOGIC INTERVENTIONS Premature a. Mother b. Infant

3. SURGICAL MANAGEMENT Preterm Births a. mother Cervical cerclage b. Infant Cardiac Surgery

Post-term Stripping the membranes Mechanical dilation Labor Induction

4. NURSING MANAGEMENT Premature Consultations Automated versus manual oxygen control Thermoregulation Skin care Fluid and electrolyte management Kangaroo mother care

Post mature Dependent Independent

NURSING PRIORITIES

GOAL OF THE DISCHARGE PLAN • The goal of the discharge plan is to ensure successful transition to home care. Therefore, Six critical components must be included in discharge planning.

1. PARENTAL EDUCATION • The participation of the parents in whatever way possible from the beginning has a positive effect on their confidence in handling the infant and readiness to assume full responsibility for the infant's care at home. • Caregivers and parents must understand that the infant's immaturity and medical status will require increased care and vigilance at home beyond that of the usual parental role.

2. COMPLETION OF APPROPRIATE ELEMENTS OF PRIMARY CARE IN THE HOSPITAL • Preparing the infant for transition to primary care begins early in the hospitalization with administration of immunizations at the recommended postnatal ages, regardless of prematurity or medical condition, completion of metabolic screening, assessment of hearing by an acceptable electronic measurement, and baseline neurodevelopmental and neurobehavioral assessment.

3. DEVELOPMENT OF MANAGEMENT PLAN FOR UNRESOLVED MEDICAL PROBLEMS • Review of the hospital course and the active problem list of each infant and careful physical assessment will reveal any unresolved medical issues and areas of physiologic function that have not reached full maturation.

4. DEVELOPMENT OF THE COMPREHENSIVE HOME-CARE PLAN • Content of the home-care plan may vary with the infant's diagnoses and medical status, the common elements include (1) identification and preparation of the in-home caregivers • (2) formulation of a plan for nutritional care and administration of any required medications • (3) development of a list of required equipment and supplies and accessible sources, • (4) identification and mobilization of the primary care physician, the necessary and qualified home-care personnel and community support services, • (5) assessment of the adequacy of the physical facilities within the home, • (6) development of an emergency care and transport plan, and • (7) assessment of available financial resources to ensure the capability to finance home-care costs

5. IDENTIFICATION AND INVOLVEMENT OF SUPPORT SERVICES • The psychological, social, economic, and educational condition and needs of the family should be addressed from the beginning of the infant's hospitalization, noting strengths that can support the infant's continued adaptation, growth, and development and any risk factors that may contribute to an adverse infant outcome.

6. DETERMINATION AND DESIGNATION OF FOLLOW-UP CARE • Arrangements for an initial appointment with the primary care physician should be made before discharge. Specific follow-up appointments with each involved surgical specialist and pediatric medical subspecialist should be made, giving attention to grouping the appointments as much as possible for the convenience of the family. A plan should be developed and discussed for emergency care and transportation to a hospital, should it be necessary.

INNOVATIONS

DOH, PHILHEALTH TO LAUNCH BENEFIT PACKAGES FOR LOW-BIRTH-WEIGHT AND PREMATURE BABIES IN 2017 • During the first-ever National Summit on Prematurity and Low Birth Weight, the Department of Health (DOH) and the Philippine Health Insurance Corporation(Phil. Health) launched new benefit packages for premature infants and small newborns. By next year, new moms and their babies will be able to avail of these packages which include treatment and services for basic care to more complex care for those who need it.

The benefit package, called the Z Benefits for Premature and Small Newborns, will provide necessary care to moms at risk of premature delivery and babies suffering preterm and low birth weight complications. It will be available to all Phil. Health members in selected government and private health facilities. Medication Coverage that range from P 600 to P 3, 000 can include medication to treat preeclampsia and eclampsia, and antenatal corticosteroids for pregnant women at risk of preterm delivery to help develop the baby’s lungs. Hospital transfer Coverage of P 4, 000 can include a pregnant woman’s transfer to a health facility that can provide the specialized care needed by the mother and child. Baby’s benefits Coverage for infants can range from P 24, 000 to P 135, 000, which can include specialized care (kangaroo mother care and Unang Yakap, for example) for premature babies and newborns with a low birth weight.
- CAPABLE FACILITY • network of facilities that can")
COMPREHENSIVE EMERGENCY OBSTETRIC AND NEWBORNCARE (CEMONC)- CAPABLE FACILITY • network of facilities that can perform the six signal obstetric functions for BEm. ONC, as well as provide caesarean delivery services, blood vi banking and transfusion services, and other highly specialized obstetric interventions. It is also capable of providing neonatal emergency interventions, which include at the minimum, the following: (1) newborn resuscitation; (2) treatment of neonatal sepsis/infection; (3) oxygen support for neonates; (4) management of low birth weight or preterm newborn; and (5) other specialized newborn services. These facilities can also serve as high volume providers for IUD and VSC services, especially tubal ligations. It should also provide an itinerant team that will conduct out-reach services to remote communities. The itinerant team is typically composed of 1 physician (surgeon), 1 nurse and 1 midwife.
 are state or multi-state networks of")
PERINATAL QUALITY COLLABORATIVES • Perinatal quality collaboratives (PQCs) are state or multi-state networks of teams working to improve the quality of care for mothers and babies. PQC members identify health care processes that need to be improved and use the best available methods to make changes as quickly as possible. • PQCs have contributed to important improvements in health care and outcomes for mothers and babies, including: • Reductions in deliveries before 39 weeks of pregnancy without a medical reason. • Reductions in health care–associated bloodstream infections in newborns. • Reductions in severe pregnancy complications.

RESEARCHES • Underlying Mechanisms Ø Inflammation in pregnancy: its roles in reproductive physiology, obstetrical complications, and fetal injury. Ø Midtrimester amniotic fluid concentrations of interleukin-6 and interferongamma-inducible protein-10: evidence for heterogeneity of intra-amniotic inflammation and associations with spontaneous early (<32 weeks) and late (>32 weeks) preterm delivery. Ø Stretch activates human myometrium via ERK, caldesmon and focal adhesion signaling. Ø Variants of stretch-activated two-pore potassium channel TREK-1 associated with preterm labor in humans. Ø Damage-associated molecular patterns (DAMPs) in preterm labor with intact membranes and preterm PROM: a study of the alarmin HMGB 1. Ø Risk of spontaneous preterm birth in relation to maternal depressive, anxiety, and stress symptoms.

• Predicting preterm delivery ØTransabdominal evaluation of uterine cervical length during pregnancy fails to identify a substantial number of women with a short cervix. ØPreterm delivery and low birth weight in singleton pregnancies conceived by women with and without a history of infertility. ØProteomic identification of serum peptides predicting subsequent spontaneous preterm birth.

• Preventing Preterm Birth ØPrevention of recurrent preterm delivery by 17 alphahydroxyprogesterone caproate. ØProgesterone supplementation and the prevention of preterm birth. ØActivity restriction among women with a short cervix.

• Caring for Preterm Infants ØThe impact of drug metabolizing enzyme polymorphisms on outcomes after antenatal corticosteroid use. ØMethicillin-resistant and susceptible Staphylococcus aureus bacteremia and meningitis in preterm infants. ØLong-term outcomes after repeat doses of antenatal corticosteroids.

COMPILED BY BSN – 4 C RLE GROUP 2: • • • • Albay, Deserey Fajamolin Amboy, Jonnie Faye Nathalie Manero Amiscua, Chezka Danielle Ganzon Asada, Sian Grace Española Baldimor, Jason Rehum Escobar Baldonado, Khryss Paula Sombilon Camposano, Janet Cudo De Julian, Divine Mercy Braza Gallego, Jaya Teresa Lira Nuyad, Rizzi Fern Grace Alabo Portigo, Renz Richard Margoma Salmo, Claire Gelogo Sernicula, Ma. Hearty Clavel Villegas, Norbeth Angelie Japitan
- Slides: 82