Care Management The Transition to Meeting NCQA Standards










































- Slides: 52
Care Management: The Transition to Meeting NCQA Standards for PCMH Clyde H. Satterly, MD, MBA SUNY Upstate Medical University, Dept of Family Medicine
PCMH Recognition Getting started n Review the Standards (Physician Practice Connections-Patient Centered Medical Home (PPC-PCMH) version n Found at publications@ncqa. org n Survey tool is available for $80 n
Survey Tool Fee is $80 to register n Online Survey Tool n Can download the standards for review n Allows self assessment for readiness to apply for recognition n Takes about two hours to do rough estimate n Will result in a quick score n
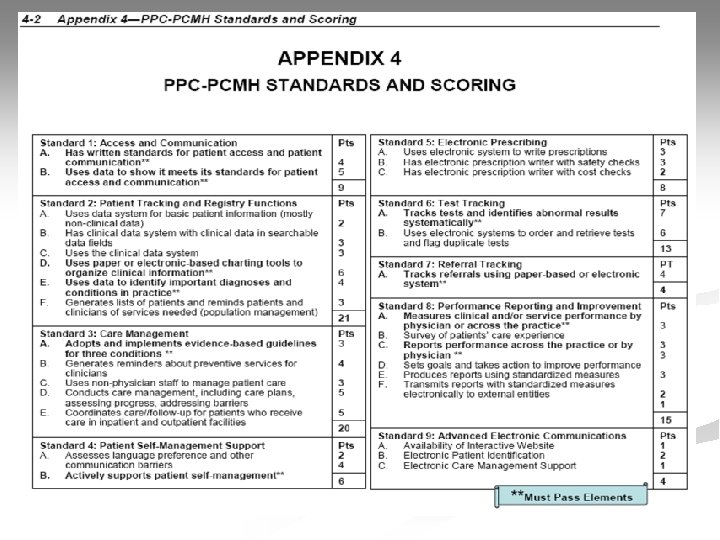
Survey Tool takes you through the nine Standards n There are 10 must pass elements of 30 n Must get a 50% score on a given element to pass n 5/10 elements , Level I Recognition n 10/10 elements 50% or greater, Level II n 10/10 elements 75% or greater, Level III n
Standard 3 Care Management Possible 20 of the total 100 points n Not too straightforward n Contains one of the 10 must pass elements for recognition n
Element A n Source: PPC-PCMH Version Standards
Clinically Important Conditions Chronic recurrent condition that practice sees n Can be the same as the most frequently seen conditions n Must be the ability to treat/change the condition n Can be condition that the practice has targeted for performance improvement n
Clinically Important Conditions There is no hierarchy among them n They will be used in fulfilling Standards 2, 3, 4 and 9 n Goal is for the practice to adopt evidenced based guidelines for the conditions n The guidelines must be meaningful to the clinicians in the practice n Must be consistent with standards of care they want to follow n
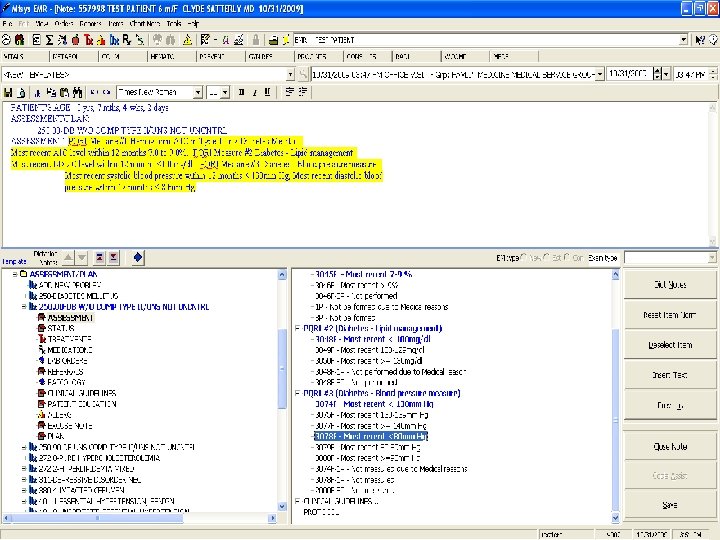
SUNY Upstate Family Medicine Medical Service Group n n n Hypertension Diabetes Mellitus Hyperlipidemia n n Same items we used for PQRI reporting Currently reporting stats for Medicare only but practice has adopted the guidelines for all patients
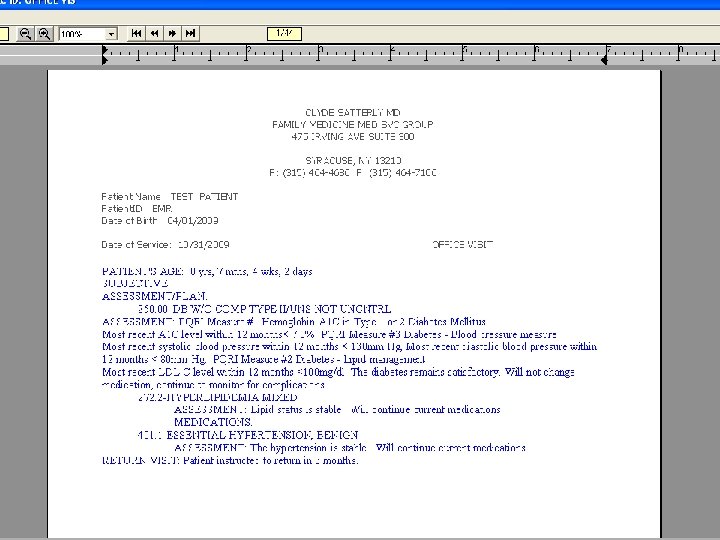
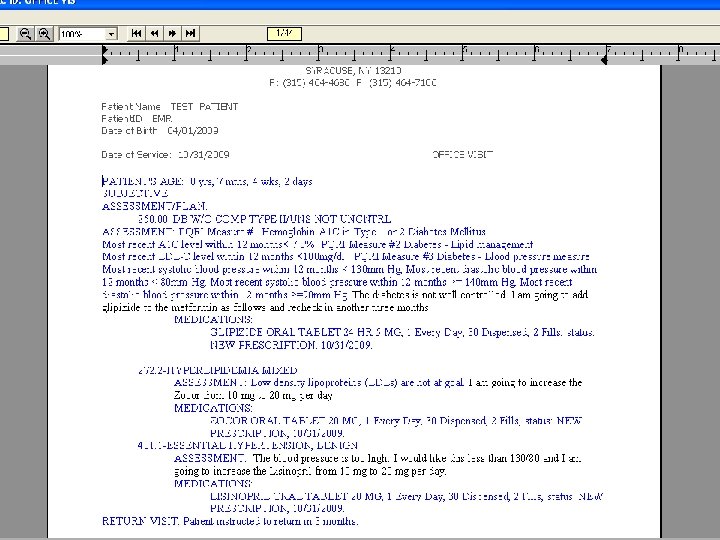
Data Source Organizers or algorithms for developing treatment plans n Flow sheets or templates for documenting progress n Registry (such as PQRI) n Screenshots for treatment plans and documenting progress n
Element B n Source: PPC-PCMH-Version Standards
Preventive Service Clinician Reminders n Age appropriate screening tests n n n n Colonoscopy Hemoccult Mammogram PAP Smear DEXA Cholesterol Diabetes
Preventive Service Clinician Reminders n Age appropriate immunizations n n n Pneumovax Seasonal flu H 1 N 1 flu Tetanus booster Childhood immunizations
Preventive Service Clinician Reminders n Age appropriate risk assessments n n Smoking Diet Depression Fall prevention
Preventive Service Clinician Reminders n Counseling n n n Smoking Cessation Diet/Exercise Alcohol/Substance Abuse Seatbelt use Safety helmets
Data Source Paper based system-submit templates, flow sheets, algorithms or reminders n EHR-submit reports generated or can use screen shots n The practice must demonstrate that clinicians have decision support available for interaction with patients (in appointments, by phone, email, etc. ) n
SUNY Upstate Family Medicine Medical Service Group Screen shots from EMR
Element C n Source: PPC-PCMH Version Standards
Practice Organization The emphasis is on a team approach to managing patient care n Shared responsibilities maximize each team members level of training and expertise n In larger practices this might involve the use of nurse case managers n
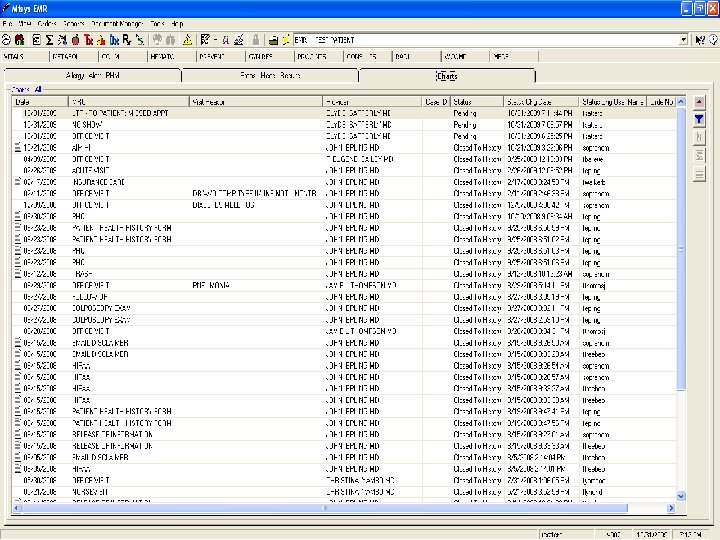
Practice Organization n Non physician staff remind patients of appointments and collect information prior to appointments n n Next follow up noted in both chart note and on encounter form Nurse orders labs prior to visit Nurse assures labs/tests in chart at time of visit Reminder Pro calls patient day before
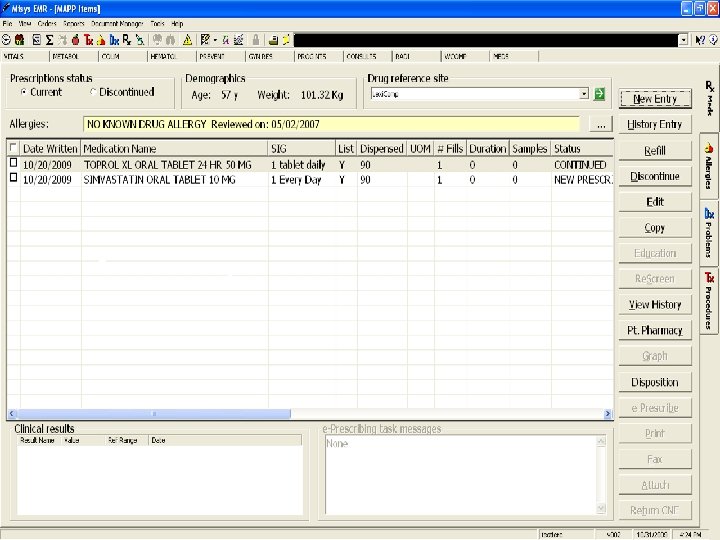
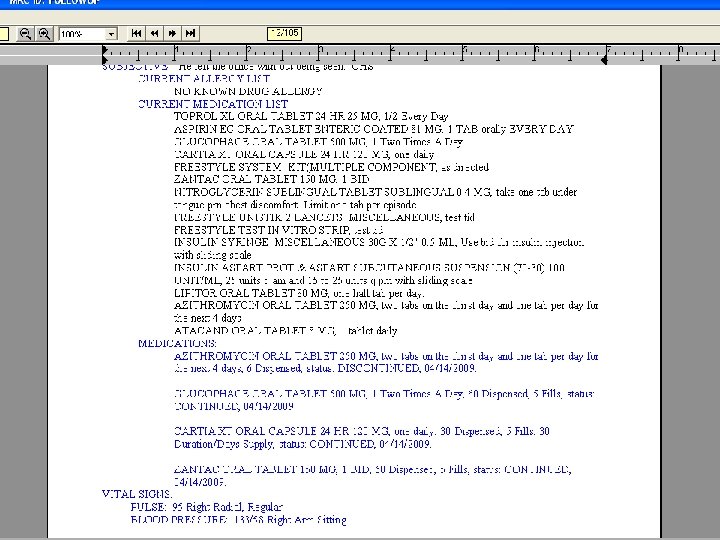
Practice Organization n Non physician staff execute standing orders for medication refills n n n All routine medications are filled for #30 with 5 refills or #90 with 1 refill IF recent f/up in 6 mos If no recent f/up then #30 with no refill If refill of controlled substance then only if chart indicates okay and refill is not early
Practice Organization n Non physician staff educate patients/families about managing conditions n n In process for SUNY Currently setting up group visits Posting our intranet for standard patient education materials the nurse can use Currently some nurses do more than others
Practice Organization n Non physician staff coordinate care with disease management or case management programs n n n In process for SUNY Currently doing this with home health care agencies Some health plans are offering case management programs here
Data Source Supporting information required here is basic n Staff job descriptions n Procedure and protocol manuals n EMR screen shots n
Element D n Source: PPC_PCMH Version Standards
Element D - Cont’d n Source: PPC-PCMH Version Standards
Care Management of Important Conditions Note the practice must document at least 4 of the 11 items are met to a degree of greater than 10% for all three conditions n This item is scored only once by a chart review n Chart review looks at a three month period n
Care Management of Important Conditions Number of patients for whom each item is entered _________________ Total number of patients seen at least once in the last three months
Care management of Important Conditions Not all patients with important conditions need care management n The patient may already be achieving good outcomes n In this case a notation in the chart indicating the patient is on target is sufficient n
Care Management of Important Conditions n Item #4 Assessing patient progress toward goals
Care Management of Important Conditions n Item#5 Reviewing medication lists with patients
Care Management of Important Conditions Items #7 -8 The barriers to be addressed may include the patient’s lack of understanding, motivation, financial need, insurance issues or transportation problems n Documentation of barriers and what, if anything, was done to address them n
Care Management of Important Conditions Item#9 Important appointments are those that the practice has requested the patient to make in order to follow standards of care (e. g. , follow-up visits for monitoring blood pressure, blood sugar or lipid levels. ) n The practice should follow up if these appointments are not kept n
Care Management of Important Conditions n Item #10 Examples of longitudinal patient data may include graphs or flow sheets showing blood pressure, weight, Hgb A 1 c, LDL levels etc over time
Care Management of Important Conditions n Item#11 Examples of after visit follow up may include checking with patients to confirm they filled a prescription or received care with a consultant.
Element E n Source: PPC-PCMH Version Standards
Element E – Cont’d n Source: PPC-PCMH Version Standards
Continuity of Care A facility may be a hospital, emergency room, skilled nursing facility or surgical center n The practice does NOT wait for these patients to make an appointment but contacts them directly n
Continuity of Care n Need for nursing home care is anticipated n The patient receives care at another facility n The patient has frequent ER visits or hospitalizations n The patient needs care of a specialist n n Practice provides the facility with appropriate information The practice reviews data to identify these patients and contacts them for follow up or reviews care plans of the patients Practice identifies these patients as needing case management and arranges for such (practice can do this internally or can use external organization) The practice makes referral and consults with the specialist and carries out recommendations
Data Source n n n The level of documentation is basic Protocols showing practice timeframe for follow-up after a hospital stay or ER visit Documentation showing how these patients are identified (hospital or ER printouts etc) Documentation of nursing facility care plans that have been reviewed Case management notes Medical record notes
zzzzzzzz…