Cardiorespiratory Fitness Assessment and Aerobic Exercise Program Purpose

Cardiorespiratory Fitness Assessment and Aerobic Exercise Program

Purpose of Clinical Exercise Testing To evaluate person’s ability to tolerate increasing levels of work output parameters measured include but are not limited to ▪ ▪ ▪ ECG hemodynamic response symptomatic ischemia electrical abnormalities exertion related problems

APPLICATIONS Diagnostic, Prognostic and Therapeutic Exercise Prescription Occupation Activities of daily living

Indications for Testing: Clinical Testing: Post MI, CABGS, etc. and Diagnostic ▪ Usually done in medical setting Functional Testing ▪ Usually done in laboratory/research or Health/Fitness facility ▪ Client Project

Exercise Capacity -METS Usually described in terms of a percentage of “normal” in units of METS 1 MET: Resting metabolic rate at 3. 5 ml O 2/kg/min 1 MET is equivalent to a metabolic rate consuming 1 kilocalorie per kilogram of body weight per hour. 1 MET = the energy (oxygen) used by the body as you sit quietly, perhaps while talking on the phone or reading a book.

Calculation of METs on the Treadmill METs = Speed x [0. 1 + (Grade x 1. 8)] + 3. 5 Recall: Speed in meters/minute conversion = MPH x 26. 8 Grade expressed as a fraction
 n n Can compare")
METs---not Minutes in Diagnostic Testing (Report Exercise Capacity in METs) n n Can compare results from any mode or Testing Protocol Can Optimize Test by Individualizing for Patient Can adjust test to 8 -10 minute duration (aerobic capacity--not endurance) Can use prognostic power of METs

Prognostic Power of METs © 1 MET = "Basal" = 3. 5 ml O 2 /Kg/min © 2 METs = 2 mph on level © 4 METs = 4 mph on level © < 5 METs = Poor prognosis if < 65; © limit immediate post MI; ©cost of basic activities of daily living © 10 METs = As good a prognosis with medical therapy © 13 METs = Excellent prognosis, regardless of other exercise responses © 16 METs = Aerobic master athlete © 20 METs = Aerobic athlete

DIAGNOSTIC TESTING Not appropriate for the general population Age, gender, risk factors , symptoms and vigor of exercise will determine test necessity Geared toward individuals with a higher probability of disease

Guidelines for Exercise Testing Types of Tests Maximal vs. Submaximal Choice depends on clients age, risk stratification, reasons for doing the test Modes of Testing: Treadmill Bicycle Ergometer Arm Ergometer

CLINICAL TEST MODALITIES Treadmill--yields the highest VO 2 and HR Hand rails--needs and purposes Stop belt--Stop exercise Additional directions for the novice like? ? ?
 and HR Better HR and BP measures")
MORE Cycle ergometers--lower VO 2 (5 -25%) and HR Better HR and BP measures Less expensive, less noise, less space Driven by patient motivation Localized fatigue Arm ergometery-lower VO 2 (20 -30%)

PROTOCOLS Based on purpose of test, desired outcomes and the individual Bruce, Ellestad--larger incremental changes-for healthy Naughton, Balke-Ware smaller incremental changes--for older and deconditioned Can customize a protocol Treadmill incline a constant 5% and velocity increased 0. 75 km/h (. 5 mi/h) each minute. Submax tests-used for individuals that are too unstable or high risk to take to max

PROTOCOLS Submax tests are usually terminated based on a predetermined end point like 120 bpm or a MET level of 5 Most end points are patient specific Ramp Protocol-- increasingly popular--based on constant and continuous increase in workloadseemingly more accurate in estimations and more individualized
")
Types of Measurements: Direct or indirect measurement of VO 2 (evaluation of cardiovascular fitness) Heart Rate Blood Pressure RPE 12 -Lead ECG (clinical testing)

First: Contraindications to Exercise Testing

Absolute Contraindications Recent significant change in resting ECG suggesting significant ischemia, recent myocardial infarction (within 2 days), or other acute cardiac events Unstable angina Uncontrolled cardiac arrhythmias causing symptoms or hemodynamic compromise Uncontrolled symptomatic heart failure Acute infections

Absolute Contraindications Severe symptomatic aortic stenosis Suspected or known dissecting aneurysm Acute myocarditis or pericarditis http: //en. wikipedia. org/wiki/File: Ao. Dissect_Schema_01 a. png

Absolute Contraindications Acute pulmonary embolus or pulmonary infarction http: //www. daviddarling. info/encyclopedia/P/pulmonary_embolism. html http: //www. e-radiography. net/radpath/p/pe. htm

Question What are relative contraindications to exercise testing? Name 3

Relative Contraindications Left main coronary stenosis Moderate stenotic valvular heart disease Known electrolyte abnormalities (hypokalemia, hypomagnesemia) Ventricular Aneurysm

Relative Contraindications Hypertrophic cardiomyopathy Severe arterial hypertension; resting diastolic BP > 110 mm Hg and/or resting systolic BP > 200 mm Hg Tachyarrhythmias or bradyarrhythmias

Relative Contraindications High-degree atrioventricular block Uncontrolled metabolic disease (e. g. , diabetes, thyrotoxicosis, or myxedema) Chronic infectious disease (e. g. , mononucleosis, hepatitis, AIDS) Neuromuscular, musculoskeletal, or rheumatoid disorders that are exacerbated by exercise

Question What are some of the general principles of exercise testing?

GENERAL PRINCIPLES OF EXERCISE TESTING Typically, you will use either a treadmill or stationary bicycle ergometer for graded exercise testing (GXT). All equipment should be calibrated before use. Begin the GXT with a 2 - to 3 -min warm-up to orient the client to the equipment and prepare the client for the first stage of the GXT

GENERAL PRINCIPLES OF EXERCISE TESTING The initial exercise intensity should be considerably lower than the anticipated maximal capacity. Exercise intensity should be increased gradually throughout the stages of the test. Rate of increase depends on the status of the individual.

GENERAL PRINCIPLES OF EXERCISE TESTING Closely observe contraindications for testing and indications for stopping the exercise test. When in any doubt about the safety or benefits of testing, do not perform the test at that time. Monitor the heart rate at least two times, but preferably each minute, during each stage of the GXT. Heart rate measurements should be taken near the end of each minute.

GENERAL PRINCIPLES OF EXERCISE TESTING If the heart rate does not reach steady state (two heart rates within ± 5 -6 bpm), extend the work stage an additional minute, or until the heart rate stabilizes. Measure blood pressure and RPE once during each stage of the GXT, in the later portion of the stage.

GENERAL PRINCIPLES OF EXERCISE TESTING Continually monitor client appearance and symptoms. For submaximal GXTs, terminate the test when the client’s heart rate reaches 70% HRR or 85% HRmax, unless the protocol specifies a different termination criterion. Also, stop the test immediately: If there is an emergency situation If the client fails to conform to the exercise protocol If the client experiences signs of discomfort.

GENERAL PRINCIPLES OF EXERCISE TESTING The test should include a cool-down period of at least 4 min, or longer if abnormal heart rate and blood pressure responses are observed. During recovery, heart rate and blood pressure should be monitored each minute. For active recovery, the workload should be no more than that used during the first stage of the GXT.

GENERAL PRINCIPLES OF EXERCISE TESTING A passive recovery is used in emergency situations and when clients experience signs of discomfort and cannot perform an active cool-down.

VO 2 Max Measurements Using Direct Gas Fractions

VO 2 Max Testing Requirements Employ at least 50% of the total muscle mass. Activities which meet this requirement include running, cycling, and rowing. The most common laboratory method is the treadmill running test. A motorized treadmill with variable speed and variable incline is employed. Be independent of strength, speed, body size, and skill. The exception to this rule is specialized tests for swimmers, rowers, skaters, etc.

VO 2 Max Testing Requirements Be of sufficient duration for cardiovascular responses to be maximized. Generally, maximal tests using continuous exercise protocols are completed in 6 to 12 minutes. Be performed by someone who is highly motivated! VO 2 max tests are very tough, but they don't last too long.

VO 2 Measurement Using Gas Fractions However, at some point, an increase in intensity will not result in an “appropriate” increase in oxygen consumption. < 150 ml/min increase with ↑ in workload Ideally, the oxygen consumption will completely flatten out despite ever-increasing workload. This is the true indication of achieving VO 2 max.

VO 2 Measurement Using Gas Fractions Other VO 2 max criteria include: No change in HR (with ↑ in workload) RER > 1. 15 RPE > 17 (Borg 6 - 20) Within 10 beats of est. HRmax Lactate > 8 m. M/L

VO 2 Max vs. VO 2 Peak VO 2 max = the maximal oxygen consumption cardiopulmonary limitation. VO 2 peak = the highest value the individual was able to attain during test. May not be VO 2 max Verified by secondary criteria protocol limitations prevent a plateau subject limitations prevent a plateau

ACSM Equations for Calculating Treadmill VO 2 without Directly Measuring Gas Fractions

The Estimate of VO 2 max How do we get there VO 2 max = SM 2 + b (HRmax - HR 2) We need to calculate estimated VO 2 values ▪ ▪ We need to calculate a slope ▪ Submax VO 2 1 (SM 1) and Submax VO 2 2 (SM 2) SM 2 is the intercept for the regression equation Using SM 1 and SM 2 Values and HR 1 and HR 2 values Estimation of HR max
")
Submax VO 2 Equations on a Treadmill Walking (1. 9 to 3. 7 mph) gross VO 2 (ml·kg-1·min-1) = [S × 0. 1] + [S × G × 1. 8] + 3. 5 Running (>5. 0 mph) gross VO 2 (ml·kg-1·min-1) = [S × 0. 2] + [S × G × 0. 9] + 3. 5 S = speed of treadmill in m·min-1; 1 mph = 26. 8 m·min-1 G = grade (% incline) of treadmill in decimal form; e. g. , 10% = 0. 10

VO 2 Max Estimation Using ACSM Equations From A Submax Test Calculate SM VO 2 for two exercise stages Use following equation to estimate VO 2 max = SM 2 + b (HRmax - HR 2) b =(SM 2 - SM 1)/(HR 2 -HR 1) This equation is for use with last and second to last exercise stages ▪ HR should be from 115 bpm to 150 bpm

Submaximal Exercise Testing and the Estimation of HR max If HR max not known then use an equation to estimate Most use equation with the assumption that HR decreases with age. “The Famous” 220 -age ▪ ± 11 bpm (+ 10 -15% error, Londeree) 208 – (0. 7 x Age) ▪ Tanaka, Monahan, and Seals found that this to be a more accurate formula for individuals over 60 and under 20 years of age. Assign Hrmax 220 -age

Question What are the assumptions related to using submaximal exercise testing to estimate VO 2 max?

Submaximal Exercise Testing Assumptions Reach steady state HR Linear relationship between HR, O 2 uptake and work intensity ▪ Curvilinear at heavier exercise Mechanical efficiency same for all Overestimates trained Underestimates untrained Stop test at 70% HRR (Karvonen) or 85% Max HR (estimated)

Question What are the indications for stopping a test either a test VO 2 max test of submaximal test when there is no ECG used? What about when there is an ECG?

Terminating the Test Termination point of testing subject requests to stop doctors orders symptom-limited guidelines observed maximal limit reached Record heart rate, blood pressure, RPE, and take ECG strip

ACSM Guidelines for Test Termination Absolute Indications Suspicion of a myocardial infarction or acute myocardial infarction (heart attack) Onset of moderate-to-severe angina (chest pain) Drop in systolic blood pressure (SBP) below standing resting pressure or drop in SBP with increasing workload accompanied by signs or symptoms Signs of poor perfusion (circulation or blood flow), including pallor (pale appearance to the skin), cyanosis (bluish discoloration), or cold and clammy skin Severe or unusual shortness of breath
 symptoms ▪ e.")
ACSM Guidelines for Test Termination Absolute Indications CNS (central nervous system) symptoms ▪ e. g. , ataxia (failure of muscular coordination), vertigo (An illusion of dizzying movement), visual or gait (pattern of walking or running) problems, confusion Serious arrhythmias (abnormal heart rhythms) ▪ e. g. : second / third degree AV block, atrial fibrillation with fast ventricular response, increasing premature ventricular contractions or sustained ventricular tachycardia Technical inability to monitor the ECG Patient's request (to stop)

ACSM Guidelines for Test Termination Relative Indications Any chest pain that is increasing Physical or verbal manifestations of shortness of breath of severe fatigue Wheezing Leg cramps or intermittent claudication (grade 3 on a 4 -point scale)

ACSM Guidelines for Test Termination Relative Indications Hypertensive response (SBP >260 mm Hg; DBP>115 mm Hg) Pronounced ECG changes from baseline ▪ >2 mm of horizontal or down sloping ST- segment depression, or >2 mm of ST-segment elevation (except in a. VR) Exercise-induced bundle branch block that cannot be distinguished from ventricular tachycardia Less serious arrhythmias (abnormal heart rhythms) such as supraventricular tachycardia
 Subject request Angina or angina-like symptoms")
Indications for Stopping Exercise Test-(no physician, no EKG) Subject request Angina or angina-like symptoms Drop (10 mm. Hg) in systolic blood pressure or failure for systolic to increase with increasing intensity Systolic > 250 mm. Hg, Diastolic > 115 No ↑ HR with ↑ in intensity Noticeable change in heart rhythm Observations: fatigue, lightheadedness, confusion, nausea, clammy skin, color Severe fatigue Equipment failure

Field Tests
")
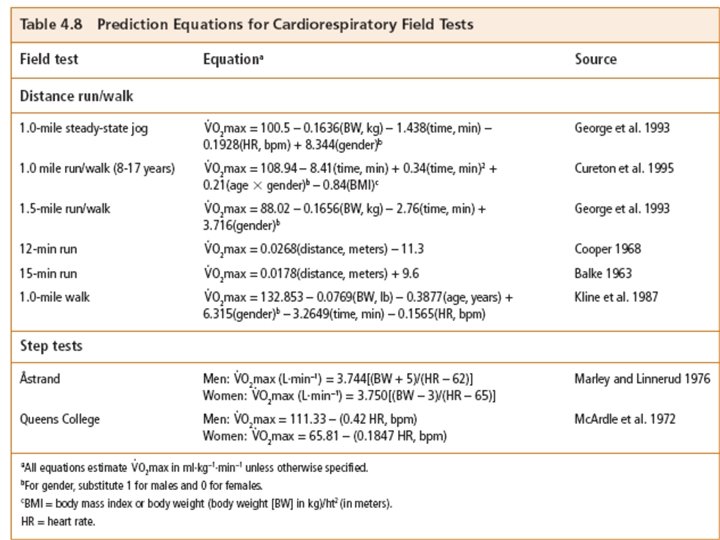
Cardiorespiratory Fitness Assessment: Field Tests Field test (see text for description of field tests) Time saving Less expensive Handle large groups Easy to administer Can classify health men (< 45 yr) and women (< 55 yr) Do not detect CHD Require client to learn how measure pulse

The Exercise Prescription for CRE

Guidelines for Exercise Prescription To Improve Health mode: rhythmic with large muscle groups intensity: moderate (~45% VO 2 max) freq: daily duration: accumulate 30 minutes/day To improve Fitness mode: rhythmic with large muscle groups intensity: 40/50 to 85 VO 2 max frequency: 3 -5 d/wk duration: 20 -30 min continuous

Phases of Training Initial Phase 0 -4 wks low intensity slow progression Improvement Phase 4 -5 months increasing intensity systematic progression, one element at a time Maintenance Phase 6 months on maintain intensity, may decrease frequency

Modes of Exercise

Methods To Monitor Intensity
 Convert VO 2 max or")
Methods To Monitor Intensity MET Method (VO 2 reserve) Convert VO 2 max or VO 2 peak to METs (Metmax) Determine the VO 2 reserve (Metmax - 1 Met) Choose a training intensity (40 -85% * VO 2 R) Add 1 MET back to the %VO 2 R Example: VO 2 max = 35 ml/kg min (1 MET = 3. 5 ml/kg min) VO 2 max = 10 MET VO 2 R = 10 MET - 1 MET = 9 MET 65%VO 2 R = 0. 65 x 9 MET = 5. 85 MET training intensity = 5. 85 MET + 1 MET = 6. 85 MET
 Estimate HRmax (220 -age) Subtract RHR (220 -age) – RHR Multiply by")
HRR (Karvonen) Estimate HRmax (220 -age) Subtract RHR (220 -age) – RHR Multiply by the intensity (percent of max effort) [(220 -age) – RHR]*% Add RHR back in {[(220 -age) – RHR]*%}+RHR ACSM recommends 40/50 -85% HRR

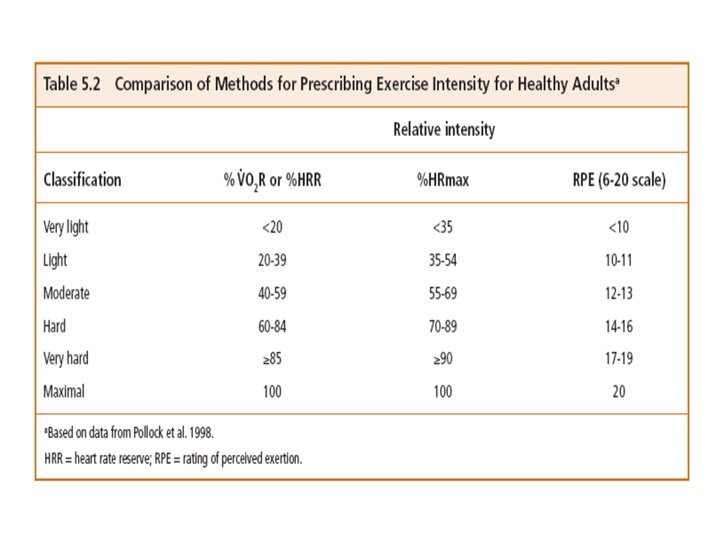
% HRmax Method ACSM recommends 55/60% to 90% HRmax % HR max x HRmax = Target HR . 60 x 170 bpm = 102 bpm %HR max does not equal %VO 2 R or%HRR 55%HRmax = 40%VO 2 R 70%HRmax = 60%VO 2 R 90%HRmax = 85%VO 2 R

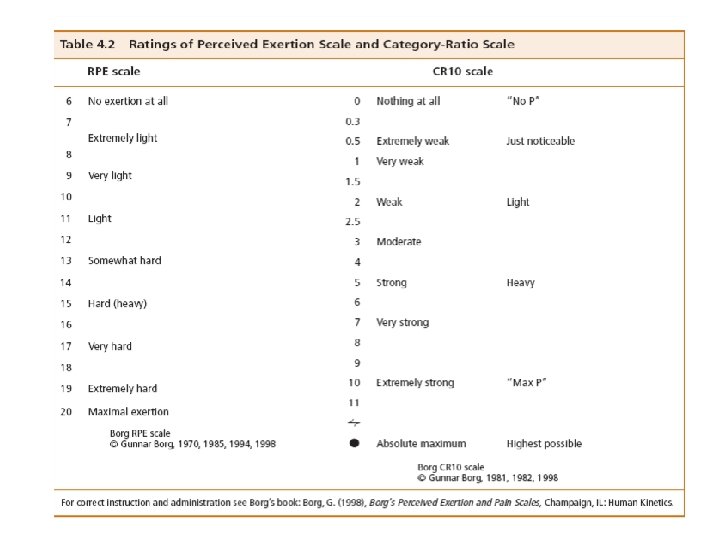
RPE Method Best to use in combination with HR Can be used alone ratings between 12 (somewhat hard) to 16 (hard) 6 No exertion at all 7 Extremely light 8 9 Very light 10 11 Light 12 13 Somewhat hard 60% 14 15 Hard 16 17 Very hard 85 % 18 19 Extremely hard HRR 20 Maximal exertion

FREQUENCY For Health moderate exercise daily For Fitness moderate/hard exercise ▪ initial phase, 3 -5 times/wk ▪ improvement phase, 5 times/wk ▪ maintenance phase, 2 -4 times/wk Persons with compromised functional capacity (Estimated VO 2 max < 10. 2 ml. kg. min) multiple daily sessions
 10")
DURATION ACSM recommends 20 to 30 min (up to 60 min or more) 10 minutes may be best for poorly fit Caloric threshold ACSM: 150 to 400 Kcal per session VO 2 L/min X 5 approximates # Kcals per minute > 1000 Kcal per week Initial: may be as low as 200 to 600 Kcal Improvement: may be from 800 to 2000 Kcal


Types of Training Continuous one, low to moderate aerobic training mode no rest intervals Discontinuous several intermittent low to high intensity exercise bouts interspersed with rest intervals ▪ Both are equally effective ▪ Drop out rate greater for high intensity discontinuous mode

Interval Training Exercise bouts interspersed with rest or lower intensity exercise bouts Design to improve aerobic endurance 3 -4 min bouts of 70 -85% VO 2 max Followed by 1. 5 -2 min bouts of 40% VO 2 max 4 -5 repeated sessions Design to improve speed anaerobic endurance One-half to 1 minute bouts of 90 -110% VO 2 max Followed by 1 -2 minute bouts of 40 -50% VO 2 max 8 -10 repeated sessions
 Demographics: List the following information for your")
Cardiorespiratory Testing For your write-up (Part II) Demographics: List the following information for your client Cardiorespiratory Fitness Assessment ▪ GXT and Field Test Comparison of GXT and field test: Compare the estimated VO 2 from the GXT and the field test. Explain any differences. Classify your client's cardiorespiratory fitness level using the VO 2 max estimate from the GXT

Cardiorespiratory Testing Aerobic Exercise Program Explain why the exercise mode was selected. Give reasons for selecting specific initial exercise intensity.
 duration, kcal/min, speed (walking or jogging")
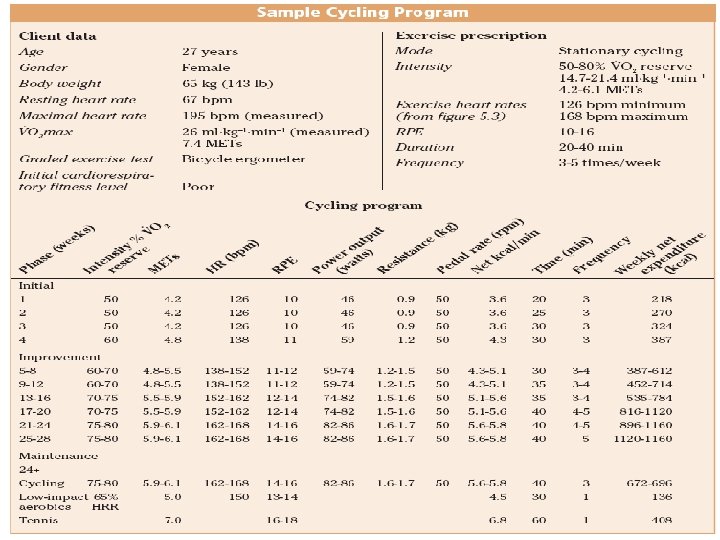
Cardiorespiratory Testing Show all calculations for intensity, (THR) duration, kcal/min, speed (walking or jogging program), work rate (cycling program), and weekly energy expenditures. ▪ Use ACSM formulas for speed or work rate calculations. Specify times for reevaluation of VO 2 max and expected percentage of improvement in VO 2 max by the time the client reaches the maintenance phase of the exercise program.
- Slides: 74