Cardio Diabetes Master Class European chapter Munich Germany

Cardio Diabetes Master Class European chapter Munich, Germany May 6 -8, 2011 Presentation topic Targeting Blood Pressure : What are the Optimal Targets in CV Risk and Diabetes? Slide lecture prepared and held by: Gordon Mc. Innes, MD Professor of Clinical Pharmacology University of Glasgow, Western Infirmary Glasgow, United Kingdom

Global Mortality 2000: Impact of Correctable Risk Factors High BP Tobacco High cholesterol Underweight Unsafe sex High BMI Physical inactivity Developing region Alcohol Developed region 0 1 2 3 4 5 6 7 8 Attributable mortality in millions (total: 55, 861, 000) Adapted from The Lancet, 360, Ezzati et al. pp. 1347– 60. Copyright © 2002, with permission from Elsevier

Meta-analysis of individual Blood Pressure data for 1 million adults in 61 prospective studies Prospective Studies Collaboration Lancet 2002 360 1903 CHD mortality rate in each decade of age versus usual blood pressure at the start of that decade

Diabetes – CHD Risk Equivalent British Regional Heart Study Risk of major CHD event • No MI or diabetes 1. 00 • Diabetes diagnosed > 60 years 1. 54 • Diabetes diagnosed < 60 years 2. 39 • Prior MI 2. 51 Wannamethee SG et al, Arch Intern Med 2011; 171: 404 410

Benefits of antihypertensive treatment proportional to reduction in blood pressure ACE/CA Relative risk of stroke ACE/DBB ARB/other ACE/plac CA/DBB More/less CA/plac Systolic blood pressure difference between randomised groups (mm. Hg) Results of prospectively-designed overviews of randomised trials. Lancet 2003; 362: 1527 -35.

Benefits of Antihypertensive Treatment Absolute Risk Reduction

UKPDS : Tight Glucose vs Tight BP Control and CV Outcomes in UKPDS 0 Stroke Any Diabetic Endpoint DM Deaths Microvascular Complications 5% % Reduction In Relative Risk -10 10% 12% -20 24% * -30 32% * *P <0. 05 compared to tight glucose control -40 37% * 44% -50 * Tight Glucose Control Tight BP Control (Goal <6. 0 mmol/l or 108 mg/d. L) (Average 144/82 mm. Hg) UKPDS 1998

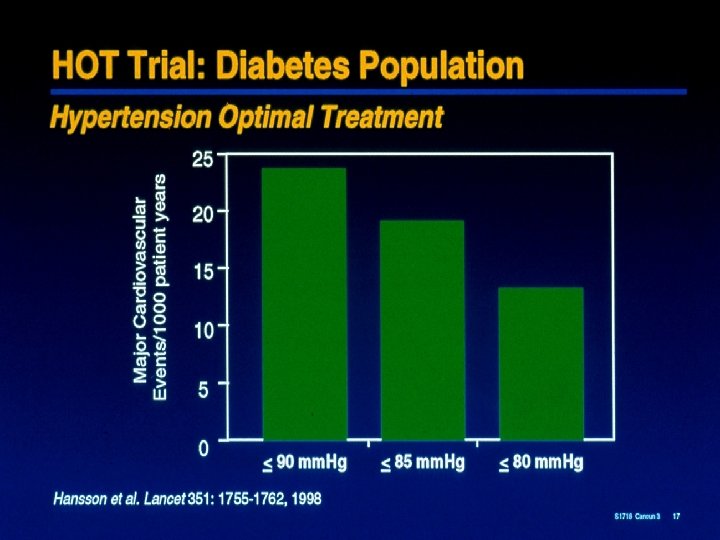
HOT Study: Effects of blood pressure on cardiovascular events • Minimum blood pressures around which the maximum benefits of treatment can be expected are – systolic between 130 mm. Hg-140 mm. Hg – diastolic between 80 mm. Hg- 85 mm. Hg • Between 5 -10 cardiovascular events can be prevented in every 1000 patients successfully treated for 1 year Hansson L, et al. Lancet 1998; 351: 1755 62
 Study Intensive BP-lowering decreases cardiovascular risk in patients with hypertension,")
Hypertension Optimal Treatment (HOT) Study Intensive BP-lowering decreases cardiovascular risk in patients with hypertension, especially among those with diabetes Major CV events per 1000 patient years 30 24. 4 25 All patients (n=18 790) Diabetics (n=1501) 20 18. 6 15 10 9. 9 10. 0 11. 9 9. 3 5 0 90 mm Hg 85 mm Hg 80 mm Hg Target DBP group Lancet 1998; 351: 1755– 1762
 Incidence")
UKPDS: Microvascular Endpoints, MI, and SBP Adjusted incidence per 1000 patient years (%) Incidence of microvascular endpoints and MI by updated mean SBP* 50 MI Adjusted for age, sex, and ethnic group Microvascular endpoints Expressed for white men, 40 50– 54 years old at baseline and with mean diabetes duration of 10 years 30 20 10 0 110 *Updated mean SBP = average of the baseline and all available annual measurements 120 130 140 150 160 170 Updated mean SBP (mm. Hg)* SBP = systolic blood pressure Adler et al BMJ 2000; 321: 412 -419.
")
Reduced blood pressure slows the rate of GFR decline Mean arterial pressure (mm. Hg) 95 98 101 104 107 110 113 116 119 Decline in GFR (m. L/min/year) 0 -2 r = 0. 69; P < 0. 05 -4 -6 Untreated hypertension -8 -10 -12 130/85 140/90 -14 Bakris et al. Am J Kidney Dis 2000; 36: 646– 661

More Versus Less Intensive BP Control Meta-analysis : RR BP diff Stroke CHD HF Major CV event CV deaths Total mortality DM No DM All 6. 0/4. 6 0. 64 0. 84 0. 69 0. 75 0. 67 0. 73 3. 7/3. 3 0. 89 1. 13 1. 10 1. 01 1. 30 1. 07 0. 76 0. 95 0. 82 0. 87 0. 93 0. 89 BPLTTC, Arch Intern Med 2005; 165: 1410 1419
 < 140/90 < 130/80 Europe")
Blood Pressure Targets Uncomplicated. DM CRF US (2003 ) < 140/90 < 130/80 Europe (2007) < 140/90 < 130/80 WHO/ISH (2004) SBP < 140 < 130/80 UK (2004) < 140/85 < 130/80 China (2005) < 140/90 < 130/80
 and Stroke by Diastolic Blood Pressure Strata 35")
INVEST: Incidence of Myocardial Infarction (MI) and Stroke by Diastolic Blood Pressure Strata 35 Incidence (%) of MI or Stroke 30 MI Stroke 25 20 15 10 5 0 ≤ 60 >60 to ≤ 70 >70 to ≤ 80 >80 to ≤ 90 >90 to ≤ 100 >100 to ≤ 110 >110 DBP (mm Hg) Messerli FH et al Ann Intern Med 2006; 144: 884 - 893
 in")
ESH guidelines - Reappraisal • Rigorous control of BP (< 130 mm. Hg) in diabetes or prior CV disease not supported by trial evidence • J-curve phenomenon unlikely except perhaps in advanced occlusive disease Mancia G, Blood Pressure 2009
 <140/85 130–")
Recommendations for BP Goals BHS-IV 1 ESH-ESC 2 BP goal (mm. Hg) <140/85 130– 139/80– 85 Diabetes mellitus <130/80 130– 139/80– 85 Kidney disease <130/80* 130– 139/80– 85 Other high risk (stroke, myocardial infarction) <130/80 130– 139/80– 85 Type of hypertension Uncomplicated Complicated *Lower if proteinuria is >1 g/day 1. Williams B et al J Human Hypertension 2004 2. Mancia et al. Blood Pressure 2009
 Per-Indap Placebo (n=5569) (n=5571) Combined")
ADVANCE: Primary Outcomes number of events RR reduction (95%CI) Per-Indap Placebo (n=5569) (n=5571) Combined Macro & Microvascular Events 861 938 9% (0 to 17%) Macrovascular Events 480 520 8% (-4 to 19%) Microvascular Events 439 477 9% (-4 to 20%) favours per-indap 0. 5 Average BP during follow-up 140. 3 / 77. 0 mm. Hg Placebo 137. 4 / 74. 8 mm. Hg Peridopril-Indapamide favours placebo 1. 0 Hazard Ratio 2. 0 ADVANCE Collaborative Group 2007

ADVANCE & ACCORD in context - UKPDS Incidence of myocardial infarction & microvascular end points by mean systolic BP, adjusted for age, sex, & ethnic group expressed for white men aged 50 54 yrs at diagnosis & mean duration of diabetes of 10 yrs 50 incidence/1000 patient. yrs (%) ACCORD ADVANCE UKPDS 40 Myocardial Infarction 30 Microvascular Endpoints 20 10 0 110 120 130 140 150 mean systolic BP (mm. Hg) 160 170 UKPDS 36: 2000

Risk of Stroke in DM or Impaired FBS Messerli FH, Bangalore S JACC 2011; 57: 114 - 115
- Slides: 20