CARDIAC STRESS TESTING WHO WHEN WHY AND HOW






















")




 � ETT is first line; if it correlates with")























- Slides: 54
CARDIAC STRESS TESTING: WHO, WHEN, WHY, AND HOW Ross S. Pacini, M. D.
Objectives � Understand basic indications and contraindications to stress testing � Understand the differences between types of stress tests and know which one to order � Learn about some of the newer data on stress testing, especially in regards to “screening” stress tests
Background � ETT has been around for a long time; Dr. Bruce originally published his protocol in 1963 � Nuclear SPECT imaging was developed in the 1980’s � Stress echocardiography developed concurrently but became more popular in the 1990’s
Background � Indications and implications have changed dramatically with improvements in medical therapy �ASA was novel in the 1980’s; first statin was marketed in 1987 � Key Point: Stress testing is not designed to detect any CAD, but to detect obstrucive CAD �>50% LM; >70% epicardial artery
Background � Fundamental to understanding stress testing or any diagnostic test is this man’s work.
Bayes’ Theorem � Bayes work in the 1700’s is what drives our stress testing model today � His theory basically says that the posttest probability of an event is driven dramatically by the pre-test probability �The usefulness of a test is in the intermediate pre-test probability
An example �A new blood test can determine the likelihood that a person will produce intelligent children � Who needs the test? �A MENSA scholar with a known IQ of 160 �An accountant with a college degree but some dyslexia �An Oakland Raiders fan who sits in the Black Hole (my example of an incredibly dumb person )
In the same way also… � Who needs a stress test? � 55 y/o male with DM, HTN, HL, 50 pack-year smoking hx, and typical angina � 62 y/o female with right-sided chest pain q 23 days that is brought on by exertion � 25 y/o male with a single episode of chest pain after eating a spicy meal?
Interpretation of results � 1 st pt: Pre-test is 95%; with a positive test, it is 99%. With a negative test, it is 90% � 3 rd pt: Pre-test is 3%; with a positive test, it is 10%; with a negative test, it is 1% � 2 nd pt: Pre-test is 45%; with a positive test, it is 87%; with a negative test, it is 10%
So… � Key Point: The determination of your pre -test probability is the key to deciding who needs a stress test.
Determining Risk � Exercise stress test guidelines* tell us to quantify angina using 3 characteristics �Substernal location of chest pain �Provoked by exertion or emotional stress �Relieved by rest or NTG � Typical/Definite angina: 3/3 � Atypical/Probable: 2/3 � Nonanginal Chest Pain: 1/3 � Asymptomatic: 0/3 * Gibbons, et al. Journal American Collge of Cardiology, 2002.
Determining Risk -Note that testing is appropriate for intermediate risk -Also note that asymptomtatic folks are all LOW risk
More simply � You all are obviously very capable of determining general cardiac risk, but if you need help, check Framingham risk score �<10% is low risk � 10 -20% is intermediate �>20% is high-risk � Very low risk, reassure; very high risk, call me! Stress those in between.
Once you’ve decided to stress � Each stress test can be broken down into a stress component and an “imaging” component � Stress component include exercise (preferred), dobutamine, Persantine (dipyridamole), adenosine, Lexiscan (regadenoson), and pacing. � “Imaging” components include EKG (first line), echo, and nuclear.
Stress Component � Exercise is preferred method of stress �Get physiologic data including BP, heart rate recovery, arrythmia evaluation, etc �Don’t exercise pt’s who can’t exercise ○ Those with significant leg or back issues ○ Those who are unsteady ○ Those who can’t reach 85% of MPHR �There are protocols other than Bruce that can be considered
Stress Component � Dipy, Adenosine, and Regadenoson are all vasodilator stress agents �Vasodilate coronaries creating a steal phenomenon in stenosed vessels �Most important contraindications are severe reactive airway disease and serious bradyarrhythmias/AV conduction defects �Caffeine interferes with effects; pt must have at least 12 hours (24 preferred) without caffeine
Stress Component � Dobutamine is a beta-agonist, causing elevated heart rate and contractility �Most important contraindication is the presence of serious ventricular arrythmias �B-blockers will interfere with effect, so should be held
Stress component � It is possible to stress using atrial or esophogeal pacing � Obviously, not done routinely; I’ve done it once, and I did it incorrectly
Imaging Component � EKG is first-line for those who have an interpretable EKG �LBBB �WPW �Dig Effect �LVH �Paced rhythm �>1 mm ST depression on resting ECG
Imaging component � Most ECG’s are interpretable �RBBB �Minor ST-T wave changes �Occasional PVC’s � Caveat: Location of ST depression does not correlate with area of ischemia
Imaging Component � Stress ECG is also very useful for determining functional capacity and efficacy of therapy � We can evaluate more than just the ECG
Imaging Component � Echocardiography looks at several views of all walls of the LV and compares them at rest and stress, looking for hypokinesis of affected wall � Requires good echo windows �Not obese �No bad COPD
Imaging component � Pt must be able to transfer quickly after exercise (time-dependent study) � Important caveat: ordering a stress echo does not mean that valves or other structures will be evaluated; we only look at 4 basic views of LV cavity, so if need other evaluation, please order a standard echo.
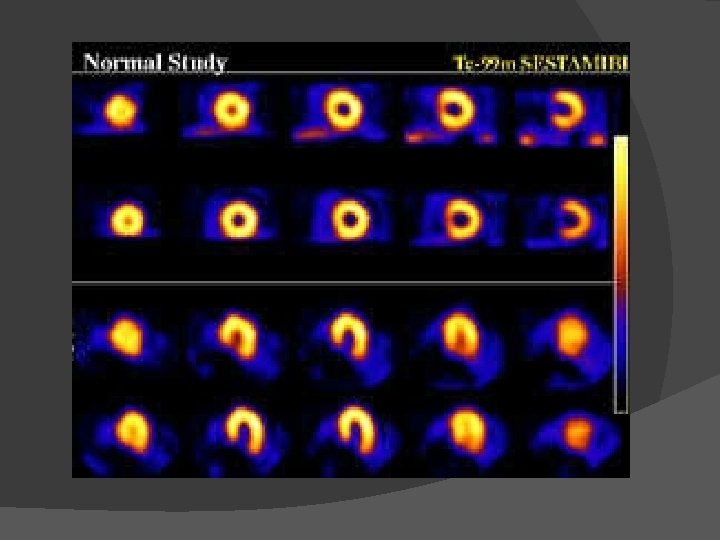
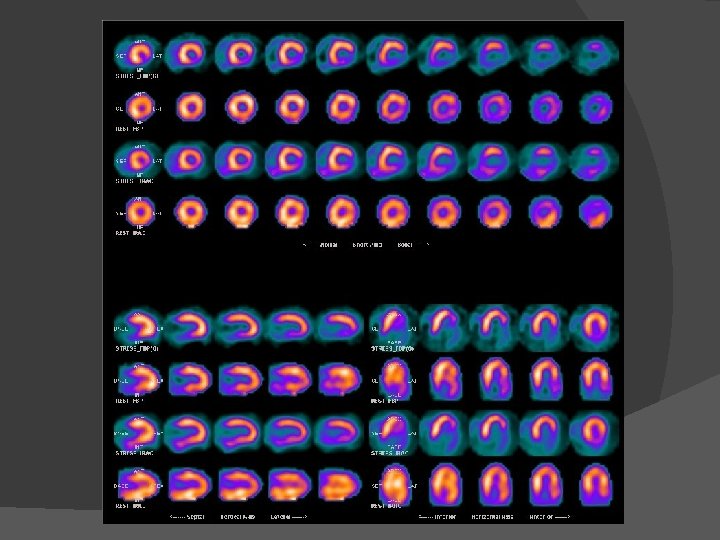
Imaging Component � Nuclear perfusion imaging evaluates blood flow to various walls, comparing rest and stress � Probably the most versatile test, though obesity and bowel interference can be a problem � Caveat: long test (pt’s should plan for 23 hours)
Putting it together � Need to pick both a stress and an imaging component that fits your patient � Vasodilators OK for either nucs or echo, but most often used with nucs � Dobutamine can be used with either echo or nucs � Again, exercise is preferred modality
Putting it together � For most patients, a standard exercise treadmill test is first line and preferred �Pt’s who can exercise and have interpretable ECG’s � Use imaging for those who cannot exercise, have uninterpretable ECG, or have non-diagnostic or suspicious ETT
What about accuracy? � ETT: Sens=68%; Spec=77% �Accuracy=73% � Exercise Echo 1: Sens=88%; Spec=79% � Dobs Echo 1: Sens=81%; Spec=80% � Exercise Nuc 2: Sens=87%; Spec=73% � Vasodilator Nuc 2; Sens=89%; Spec=75% 1: Heart. 2003 January; 89(1): 113– 118 2: Circulation. 2003; 108: 1404 -1418
My personal bias (No evidence) � ETT is first line; if it correlates with my suspicion, I’m done; if not, I pursue imaging � If I want the test to be positive, I will pursue a nuc (probably overcalls) � If I want the test to be negative, I will pursue a stress echo (probably undercalls)
What about cost? � Obviously, hospitals charge much more than this, but here are Medicare reimbursements* for each test: �ETT: $89 �Stress Echo: $208 + cost of stress agent �Nuc: $503 + cost of stress agent �Most cost effective to start with ETT *http: //www. midmark. com/Marketing%20 Collateral/CPT-Stress. pdf
Special Considerations � Yes, women have a higher false positive ETT rate; guidelines still say it is first line. � B-blockers, CCB’s: Generally, if trying to diagnose CAD, I recommend holding. If trying to evaluate success of therapy, I recommend continuing
Special Considerations � In pt’s with a LBBB, preferred test is a vasodilator nuclear scan � In pt’s with previous CAD, some sort of imaging test is preferred (ie, not just a standard treadmill).
Contraindications � Almost nothing is absolute, but two key areas to avoid/ask cardiology: �Severe outflow tract obstruction: HCM, Aortic Stenosis (can be done, but must be done very carefully) �Key Point: Unstable Coronary Symptoms. These people can die on the treadmill
Screening Stress Tests � Remember what I said in the beginning; a stress test is there to detect hemodynamically significant CAD, not just any CAD � As a general rule, you should approach asymptomatic patients with standard risk stratification using Framingham Risk Score and family history; most of the time, a stress test is not needed
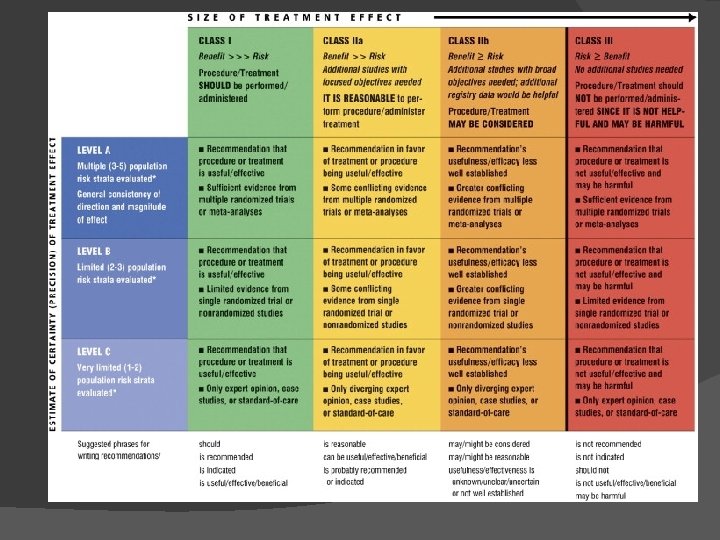
Asymptomatic Adults � Recently published guidelines* give excellent guidance, and I will just quote them: �An exercise ECG may be considered for cardiovascular risk assessment in intermediate-risk asymptomatic adults (including sedentary adults considering starting a vigorous exercise program), particularly when attention is paid to non. ECG markers such as exercise capacity. (Class IIb, LOE B) *J Am Coll Cardiol. 2010; 56(25): e 50 -e 103
Asymptomatic Adults �Stress echocardiography is not indicated for cardiovascular risk assessment in low- or intermediate-risk asymptomatic adults. (Exercise or pharmacologic stress echocardiography is primarily used for its role in advanced cardiac evaluation of symptoms suspected of representing CHD and/or estimation of prognosis in patients with known coronary artery disease or the assessment of patients with known or suspected valvular heart disease). Class III, LOE C
Asymptomatic Adults �Stress MPI may be considered for advanced cardiovascular risk assessment in asymptomatic adults with diabetes or asymptomatic adults with a strong family history of CHD or when previous risk assessment testing suggests high risk of CHD, such as a CAC score of 400 or greater (Class IIb, LOE C)
Asymptomatic Adults �Stress MPI is not indicated for cardiovascular risk assessment in low- or intermediate-risk asymptomatic adults (Exercise or pharmacologic stress MPI is primarily used and studied for its role in advanced cardiac evaluation of symptoms suspected of representing CHD and/or estimation of prognosis in patients with known CAD). Class III, LOE C
What about diabetics? � In 2009, we got the DIAD trial* (Detection of Ischemia in Asymptomatic Diabetics) �Enrolled pt’s 50 -75 y/o with DM dx’d after age 30 and no h/o DKA or CAD �Important exclusion criteria: h/o angina, stress test or heart cath in last 3 years, abnormal EKG, or other indication for stress testing *JAMA. 2009; 301(15): 1547 -1555
DIAD trial �A total of 1, 123 patients were eventually randomized: 50% to usual care; 50% to receive an adenosine MPI (nuclear) scan. � Primary endpoint was a composite of cardiac death and non-fatal MI. � Patients were followed for a median of 5 years
DIAD trial � Overall event rate was 2. 9% giving an average event rate of 0. 6%/yr. � Total events were 32: 15 in the screening group and 17 in the nonscreening group [HR 0. 88 (0. 44 -1. 8), p=0. 73]
DIAD trial � Interestingly, event rate in those with normal or only small defects was 2%, while in those with medium or large defects, it was 12. 1%. � In other words, NPV of normal MPI was 98%; PPV for all positive MPI was 6%; for medium or large defects, it was 12%.
DIAD trial � Conclusion of authors was that asymptomatic diabetic patients do not benefit from screening stress tests � A few notable caveats �Very low event rate (0. 6%) �Probably low-risk patients �Significant amount of long-term crossover �Excellent medical control of risk factors
DIAD trial � The key points here for me are twofold: � 1. Risk factor modification is the key, not stress testing � 2. Risk factor modification works! (ie, not everyone needs a stent…but that’s a separate talk)
What about Pre-Op Patients? � Pre-operative evaluation for non-cardiac surgery is a whole separate talk in itself � An evolving field, but recent guidelines* are pretty clear on this point: most patients do not need a stress test prior to surgery *J Am Coll Cardiol 2009; 54
Pre-op evaluation To the best of my knowledge, no recent trial has shown any benefit of pre-operative stress testing or revascularization � There are no class I recommendations for pre-operative stress testing; the best the guidelines will give you is a IIa recommendation for pt’s with 3 risk factors who cannot do 4 METs and are undergoing vascular surgery…do you see a lot of those patients? �
It’s positive…now what? � First rule is, don’t panic (haven’t seen this yet here in Grand Junction) � Second, treat those patients like you would any CAD patient �Start ASA �Check Lipids and treat to LDL <100 (<70) �Control BP � Separate out stable from unstable symptoms to the best of your ability
It’s positive…now what? � Most patients probably deserve a cath, but not all need it and some aren’t candidates (multiple comorbidities, etc) � Now is a good time to consult cardiology
Local Resources � One member of Western Slope Cardiology is at CH 8 -11 M-F �Offer ETT, Nucs, and now stress echos �Sit in office outside RT; available for questions, consults, guidance � St. Mary’s offers all tests � Western Slope Cardiology Diagnostic Center �ETT, Exercise Echo, all Nucs
Contact information � Main office line is 298 -2482 for both scheduling stress tests and to speak to any cardiologist � Again, cardiologist on site at CH from 811 each weekday � We are more than happy to help you choose the proper test
Key Points � Stress tests aim to detect obstructive CAD � Determining pre-test probability is fundamental to deciding who to stress � A standard exercise treadmill test is first line for most patients � “Screening” stress tests should be rare events (? Pilots, very high risk DM, very high risk surgery)
Questions…or complaints?