Cardiac palpation By Mohamed Ahmad sharawe Palpation of

Cardiac palpation By Mohamed Ahmad sharawe
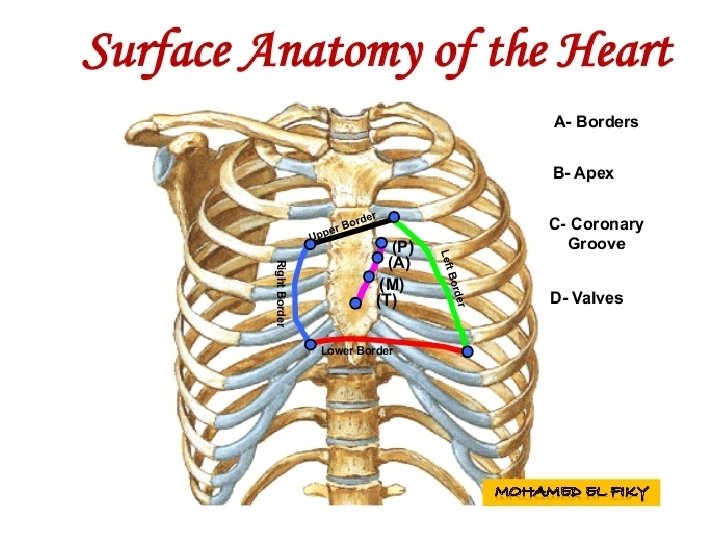
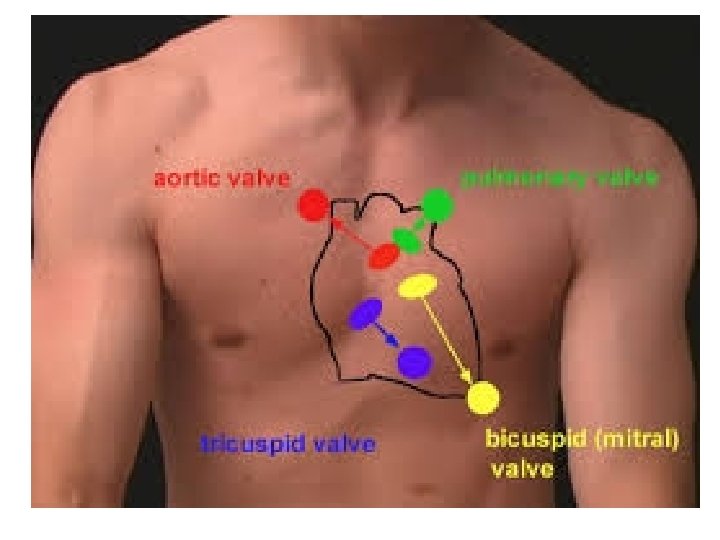
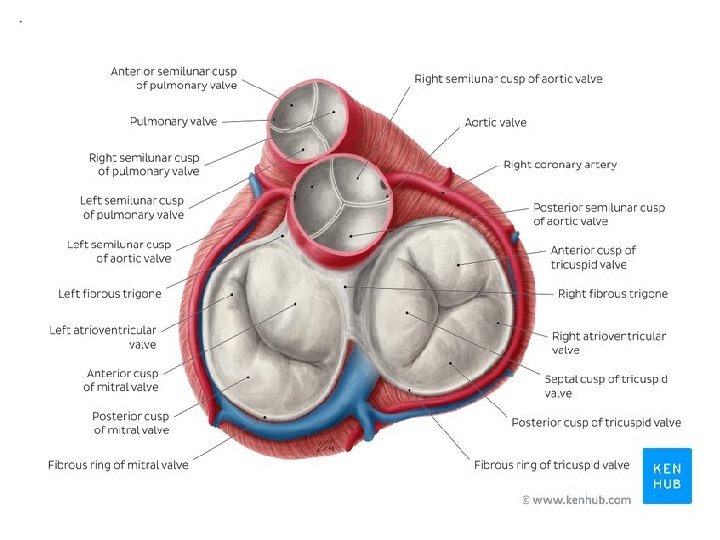
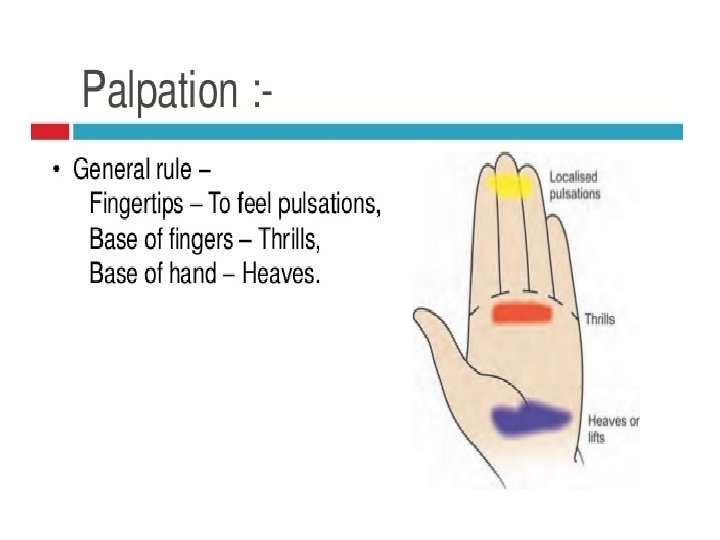

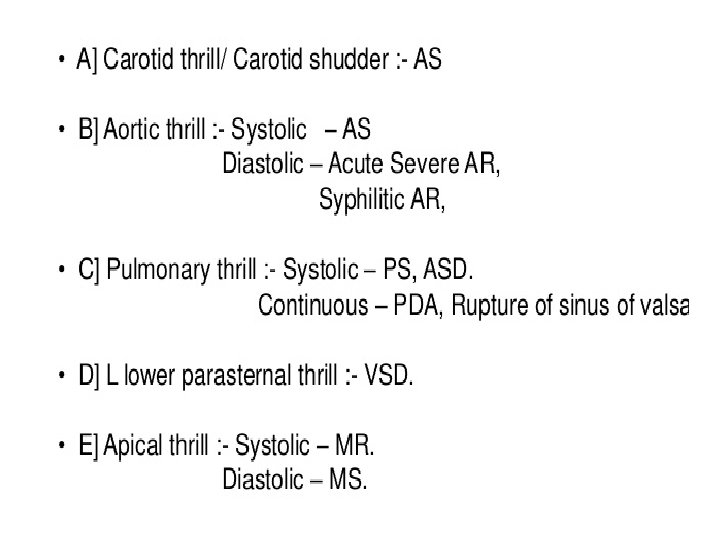
Palpation of the precordium The valve areas are palpated for abnormal pulsations (palpable heart murmurs known as thrills) and precordial movements (known as heaves). Heaves are best felt with the heel of the hand at the sternal border.

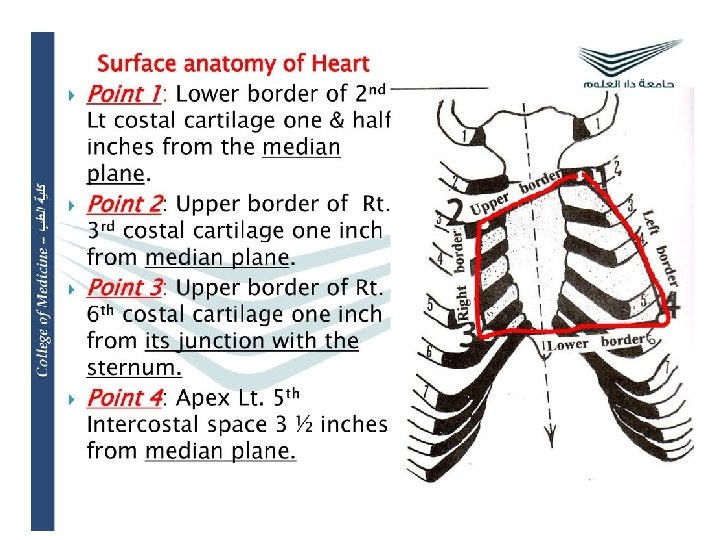
The apex beat called the apical impulse, is the pulse felt at the point of maximum impulse (PMI), which is the point on the precordium farthest outwards (laterally) and downwards (inferiorly) from the sternum at which the cardiac impulse can be felt.

What do we note in the apex? Presence Location Size (is it localized or diffuse? ) Amplitude (is it forceful? ) Duration (is it abnormally sustained? ) Type (assess based on above parameters, details are below) Thrill
 related to contraction at the")
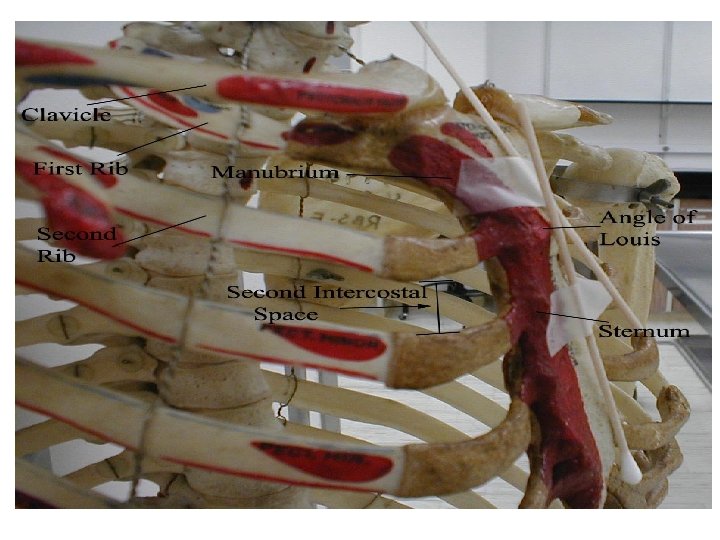
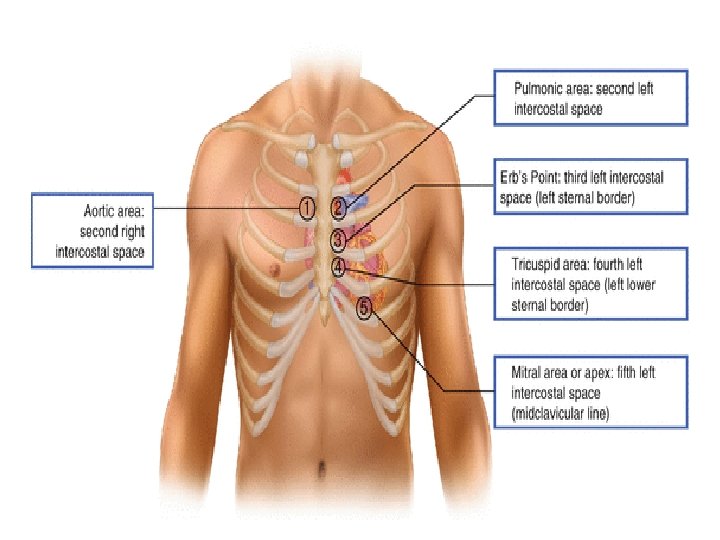
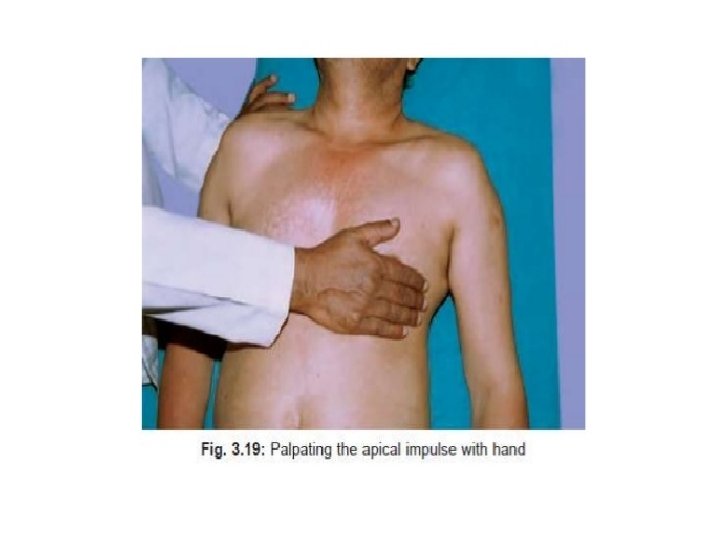
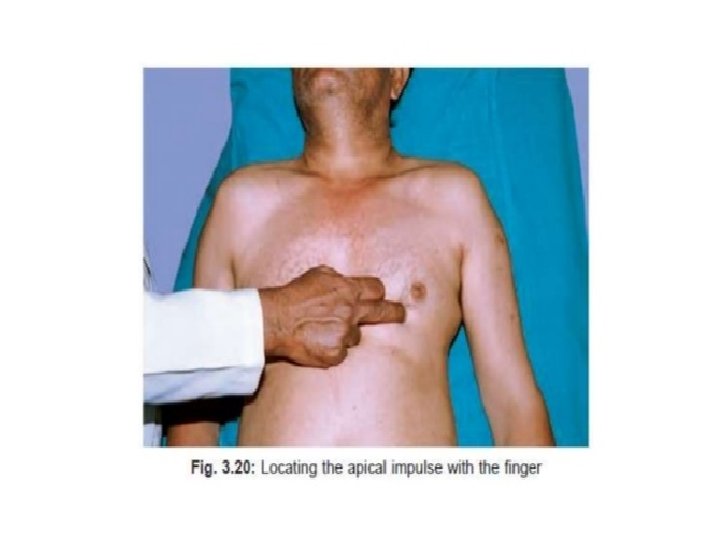
Can you feel a Point of Maximum Impulse (PMI) related to contraction at the apex of the underlying left ventricle? If so, where is it located? After identifying the rough position with the palm of your hand, try to pin down the precise location with the tip of your index finger. The normal sized and functioning ventricle will generate a penny sized impulse that is best felt in the mid-clavicular line, roughly at the 5 th intercostal space.

If the ventricle becomes dilated, most commonly as the result of past infarcts and always associated with ventricular dysfunction, the PMI is displaced laterally. In cases of significant enlargement, the PMI will be located near the axilla.

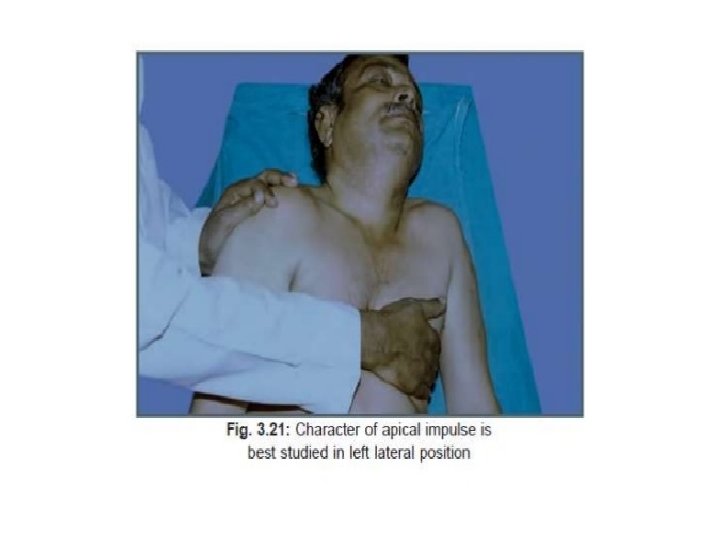
Occasionally, the PMI will not localize to any one area, which does not necessarily indicate ventricular enlargement or dysfunction. Obesity and COPD may also limit your ability to identify its precise location. Palpating while the patient is in the left lateral decubitus position can make the PMI more obvious.

Localized apex: Palpable in a single intercostal space and the longest diameter of the pulsation is within 4 cm. A localized apex is normal. Diffuse apex: Apex palpable in more than one intercostal space or longest diameter more than 4 cm, even within a single intercostal space.
 of apex beat? The normal apex beat is")
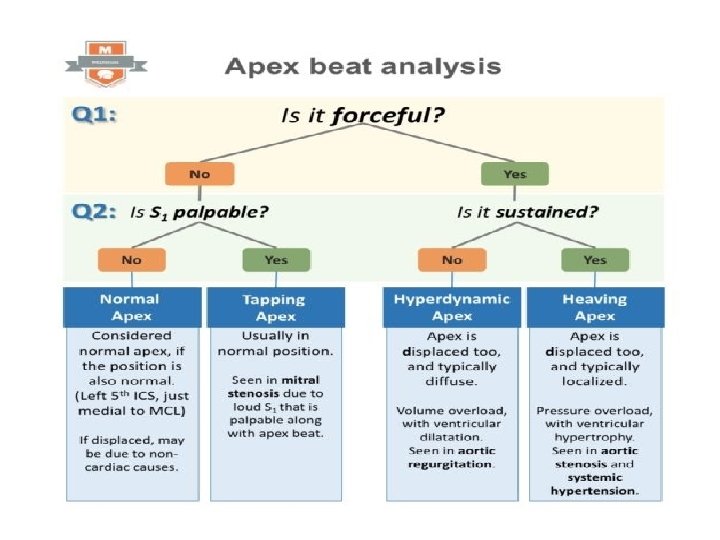
Which are the abnormal types (characters) of apex beat? The normal apex beat is a localized pulsation Tapping Apex – This is an almost normal apex beat with a palpable first heart sound. Importantly, we have to recognize that the feeling of tapping is due to the loud first heart sound heard in mitral stenosis.

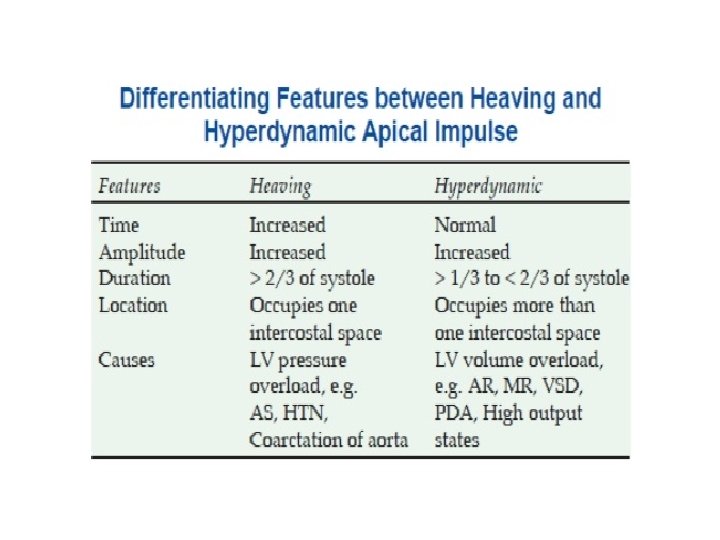
Hyperdynamic Apex – This is classically seen in volume overload conditions where there is ventricular dilatation (aortic regurgitation, hyperdynamic circulation etc. ). Hyperdynamic apex is a forceful but ill-sustained pulsation that is palpable over a larger area than usual (diffuse). Heaving Apex – Classically seen in pressure overload conditions that result in ventricular hypertrophy (aortic stenosis, systemic hypertension etc. ). Heaving apex is a forceful and sustained pulsation that is typically localized.

Double Impulse Apex – Two impulses felt during systole rather than the normal single pulsation. We see this in HCM (hypertrophic cardiomyopathy), as the poor left ventricular compliance results in an S 4 (fourth heart sound). A palpable S 4 and the sustained apex impulse give an impression of ‘double’ impulse in this condition. Dyskinetic Apex – An apex that is uncoordinated, seen in myocardial infarction when there are dyskinetic movements of the infarcted myocardium (typically an apical ventricular aneurysm). Retracting Apex – In patients with constrictive pericarditis, the apex ‘retracts’ during systole. Consequently, the fibrosed pericardium prevents the normal outward thrust during systole but allows rapid filling of the left ventricle during diastole. This contributes to the impression that the apex is ‘retracting’ during systole.

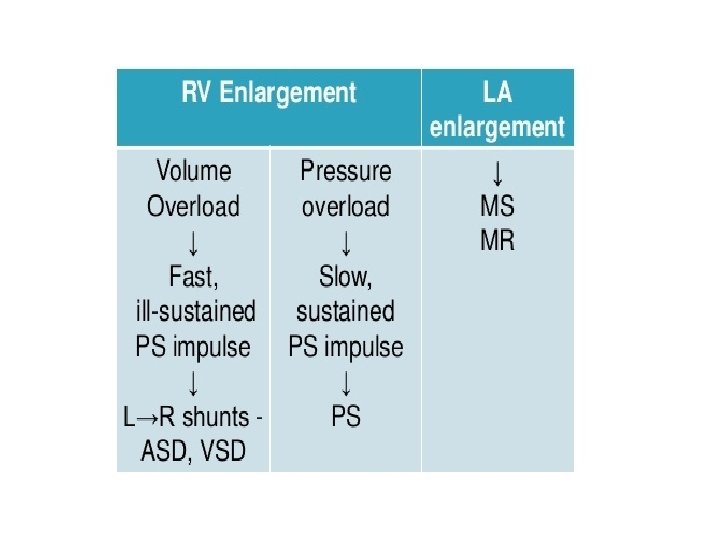
What causes DISPLACEMENT of the apex beat? Assessment of the tracheal position is important, because, tracheal deviation, along with the displacement of apical impulse, suggests mediastinal shift as a result of lung fibrosis, collapse, pneumothorax etc. If the trachea is central, but the apex is displaced, the causes are: Left ventricular enlargement – the apex displacement is downwards and lateral. Right ventricular enlargement – the apex displacement is lateral.

What causes ABSENCE of the apex beat? Absent apical impulse may be due to physiological and pathological causes. This mnemonic is helpful: DR POPE Physiological causes: Dextrocardia. Though it will be missing at the ‘usual’ location on the left side, it will be present on the right side. Apex is behind a Rib. In this case, it may not be palpable in an intercostal space. Just turning the patient to the left lateral position will reveal the apex beat, confirming this cause. Pathological causes: Pericardial effusion Obesity and thick chest wall Pleural effusion (left sided) Emphysema

- Slides: 30