Cardiac Medications Anticoagulants Anti platelet agents Ace inhibitors

Cardiac Medications • • • Anticoagulants Anti platelet agents Ace inhibitors Angiotensin 2 receptor blockers Beta blockers Combined beta and alpha blockers Calcium channel blockers Cholesterol lowering medications Digitalis diuretics

Direct Adrenergic Antagonists • Alpha blockers • Beta blockers • Alpha plus beta blockers

Adrenergic Receptor Responses to Stimulation LOCATION RECEPTOR RESPONSE Blood vessels alpha 1 and beta 2 Cardiac muscle beta 1 AV Node beta 1 heart rate Constriction / dilation Increased contractility Increased Cardiovascular SA Node Increased

LOCATION RECEPTOR RESPONSE beta 2 motility alpha 1 Decreased Gastrointestinal Muscle Sphincters Constriction

LOCATION RECEPTOR RESPONSE alpha 1 Constriction alpha 1 and beta 2 Ejaculation Contraction/ relaxation Genitourinary Bladder sphincter Penis Uterus

LOCATION RECEPTOR RESPONSE beta 2 Dilation/relaxation Respiratory Bronchial muscles

Alpha selective Blockers • Divided into alpha 1 and alpha 2 receptors • Differentiated by their location on nerves • • • 1 selective: (ends with –sin or –cin) Prazosin, Terazosin Doxazocin, Tamsulocin • 2 selective: (inhibits Negative feedback) • Yohimbine

Alpha 1 blockers • Effects: Blocks vaso- and aterioconstriction vasodilation and arteriodilaton Decrease in Blood pressure. • Blocks alpha receptors in the eye (pupillary dilator muscle) Miosis • Reduces Bladder tone and allows for more motility (especially in patients with Urinary retention, BPH)

Alpha 1 blockers Uses/Side effects • Drugs Arteriodilation, used in Raynauld’s Phenomenon • Increase Urinary Motility, used in Urinary rentention or BPH (Prazosin/Tamsulosin is most commonly used in BPH) • Side effects: Nasal Congestion, Hypotension

2 selective blockers • Yohimbine • Prevents Negative feedback Increased Release of Epinephrine and Norepinephrine • Claimed to be an Aphrodisiac • Potential uses: Impotence, Co-administrated with drug induced sexual dysfuction
 � Phenoxybenzamine (Non-competitive) � Phentolamine (competitive)")
Alpha Blockers (non-selective) � Phenoxybenzamine (Non-competitive) � Phentolamine (competitive)

Phenoxybenzamine • Non-competitive alpha adrenergic antagonist. • Net effect: α 1 blockage > α 2 blockage • Uses: malignant HTN, Pheochromocytoma, HTN 2° to Clonidine Withdrawal, Cheese Reaction

Phentolamine • Non-selective Competitive Alpha Blocker • Used in HTN, Cocaine induced HTN. • Decreases the workload of the heart, and decreases the risk of MI

Competitve Antagonist Vs. Non-competitive Antagonist

phenoxybenzamine Non-competitive Alpha receptor antagonist - used in pheochromocytoma, malignant hypertension, Clonidine Withdrawal, Cheese Syndrome Prazosin, tamsulosin, doxazosin 1 selective: uses-mild to moderate HTN, BPH, Raynaud’s yohimbine 2 antagonist: Used in impotence

Alpha Blockers side effects Body System Side/Adverse Effects Cardiovascular Palpitations, orthostatic hypotension, tachycardia, edema, dysrhythmias, chest pain CNS Dizziness, headache, drowsiness, anxiety, depression, vertigo, weakness, numbness, fatigue

Body System Side/Adverse Effects Gastrointestinal Nausea, vomiting, diarrhea, constipation, abdominal pain Other Incontinence, nose bleeding, tinnitus, dry mouth, pharyngitis, rhinitis

Prasosin Selective a 1 - adrenoblocker Administration • treatment of essential hypertension • stabile cardiac insufficiency Side effects “phenomenon of first dose”: sudden decreasing of blood pressure and even development of orthostatic collapse after first administrations of the drug Prophylaxis: administration of half-dose before sleep

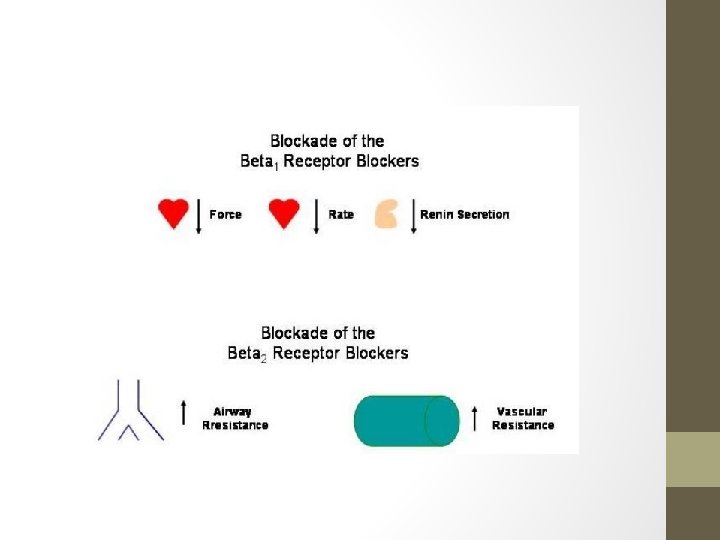
Beta blockers • Most widely used antihypertensive drugs • Two subgroups: 1. Nonselective Beta Blockers (Propranolol Beta 1 & Beta 2) • Reduce heart rate, decrease force of ventricular contraction, suppress impulse conduction through the AV node, suppress secretion of renin, bronchoconstriction. 2. Cardioselective Agents (Metoprolol-Beta 1 only) • Same as nonselective except it does not block bronchial beta 2 receptors so does not increase airway resistance

Uses of Beta Blockers • Anti-angina: decreases demand for myocardial oxygen • Cardioprotective: inhibits stimulation by circulating catecholamine • • Class II antidysrhythmic Antihypertensive Treatment of migraine headaches Glaucoma (topical use)

Side effects of Beta blockers Body System Side/Adverse Effects Blood Agranulocytosis, thrombocytopenia Cardiovascular AV block, bradycardia, congestive heart failure, peripheral vascular insufficiency CNS Dizziness, mental depression, lethargy, hallucinations

Beta Blockers Body System Side/Adverse Effects Gastrointestinal. Nausea, dry mouth, vomiting, diarrhea, cramps, ischemic colitis Other Impotence, rash, alopecia, bronchospasms

Beta Blocking Agents: Nursing Implications • Rebound hypertension or chest pain may occur if this medication is discontinued abruptly. • Patients should notify their physician if they become ill and unable to take medication. • Inform patients that they may notice a decrease in their tolerance for exercise; dizziness and fainting may occur with increased activity. Notify the physician if these problems occur.

• • Monitor BP, HR Monitor activity tolerance Monitor liver enzymes, renal function studies Instruct patient to change positions slowly to avoid syncope episodes • Monitor for respiratory distress • Monitor for hyper and hypoglycemia • Take with foods to decrease GI side effect (nausea, diarrhea).

pharmacokinetics

toxicity

Clinical presentation

Treatment

Adrenergic Blocking Agents: Nursing Implications • Remember that alpha blockers may precipitate hypotension. • Remember that beta blockers may precipitate bradycardia, hypotension, heart block, CHF, and bronchoconstriction. • Avoid OTC medications because of possible interactions. • Possible drug interactions may occur with: • • • Antacids (aluminum hydroxide type) Diuretics and cardiovascular drugs Oral hypoglycemic agents
 Bradycardia Heart block CHF Increased")
Monitor for side effects, including: Hypotension Tachycardia (alpha blockers) Bradycardia Heart block CHF Increased airway resistance Fatigue Lethargy Depression Insomnia Vivid nightmares
")
Alpha and Beta Antagonists • • Labetalol (doesn’t cross Placenta, also used in pregnancy) Blocks alpha receptors Decrease BP Blocks beta receptors Decreases HR Used in Severe HTN, Angina
 There are different types of vasodilators, including: • Arterial dilators (mainly affect")
VASODILATORS (VENODILATORS) There are different types of vasodilators, including: • Arterial dilators (mainly affect the arteries) • Venous dilators (mainly affect the veins) • Mixed dilators (affect veins and arteries) Direct vasodilators • Hydralazine (Apresoline) • Sodium Nitroprusside • Minoxidil

• Vasodilator drugs can be classified based on their site of action (arterial versus venous) or by mechanism of action. Some drugs primarily dilate resistance vessels (arterial dilators; e. g. , hydralazine), while others primarily affect venous capacitance vessels (venous dilators; e. g. , nitroglycerine). Most vasodilator drugs, however, have mixed arterial and venous dilator properties (mixed dilators; e. g. , alpha-adrenoceptor antagonists, angiotensin converting enzyme inhibitors). • It is more common, however, to classify vasodilator drugs based on their primary mechanism of action
 is a direct-acting smooth muscle relaxant used to treat hypertension")
Hydralazine • Hydralazine (Apresoline) is a direct-acting smooth muscle relaxant used to treat hypertension by acting as a vasodilator primarily in arteries and arterioles. By relaxing vascular smooth muscle, vasodilators act to decrease peripheral resistance, thereby lowering blood pressure and decreasing afterload

Clinical Use • Hydralazine is not used as a primary drug for treating hypertension because it elicits a reflex sympathetic stimulation of the heart (the baroreceptor reflex). The sympathetic stimulation may increase heart rate and cardiac output, and in patients with coronary artery disease may cause angina pectoris or myocardial infarction. Hydralazine may also increase plasma renin concentration, resulting in fluid retention. In order to prevent these undesirable sideeffects, hydralazine is usually prescribed in combination with a betablocker (e. g. , propranolol) and a diuretic. • Hydralazine is used to treat severe hypertension, but again, it is not a first-line therapy for essential hypertension. However, hydralazine is the first-line therapy for hypertension in pregnancy, with methyldopa.

Side effects • Common side-effects include: • § Diarrhea • § Compensatory tachycardia due to baroreceptor reflex ->Angina • § Headache • § Loss of appetite • § Nausea or vomiting • § Depression • § Drug-Induced Lupus Erythematosus • • Patients given hydralazine over a period of six months may develop a lupus-like syndrome or other immune-related diseases that, in general, are reversible withdrawal.

Minoxidil • Minoxidil is an antihypertensive vasodilator medication also known for its ability to slow or stop hair loss and promote hair regrowth • Minoxidil was first used exclusively as an oral drug (trade name Loniten) to treat high blood pressure. However, it was discovered to have an interesting side-effect: Minoxidil may cause increased growth or darkening of fine body hairs. When the medication is discontinued, the hair will return to normal within 30 to 60 days.

Side effects • Side effects of oral minoxidil may include swelling of the face and extremities, rapid and irregular heartbeat, lightheadedness • Pseudoacromegaly is an extremely rarely reported side effect of large doses of oral minoxidil.

Sodium Nitroprusside • Rapidly and consistently acting vasodilator • Relaxes both resistance and capacitance vessels • Unlike hydralazine it produces decrease in cardiac work and no reflex tachycardia. • Improves ventricular function in heart failure by reducing preload • Uses: Hypertensive Emergencies • Adverse effects: All are due release of cyanides (thiocyanate) – palpitation, pain abdomen, disorientation, psychosis, weakness and lactic acidosis.

Calcium Channel Blockers • Drugs the prevent calcium ions from entering cells • Vascular Smooth Muscle: • Calcium channels regulate contraction • If channels are blocked, contraction will be prevented and vasodilation will result • Act selectively on peripheral arterioles and arterioles of the heart (no effect on veins)

Indications • Hypertension • Prinzmetal’s angina: • Chest pain caused by vasospasm of the coronary arteries usually occurring at rest rather than during exercise. • Chronic stable angina • A-fib or flutter; Paroxysmal supraventricular tachycardia

Nursing Interventions • Monitor BP, HR, heart rhythm • Monitor liver enzymes, renal function • Take with food to increase absorption • Assure stool softener is ordered to prevent constipation

• Three chemical families in CCB’s • Verapamil: • Blocks calcium channels in blood vessels and in the heart • Used for: • Angina Pectoris (vasodilation) • Hypertension • Cardiac dysrhythmias • Careful administration/contraindications: • Cardiac failure, AV block, sick sinus syndrome • Diltiazem: similar to Verapamil

• Nifidipine - Relaxes vascular smooth muscle and dilates coronary and peripheral arteries - More effect on vessels less on myocardium • Used for: • Prophylaxis of Angina Pectoris (vasodilation) • Hypertension

Nitrates • Vasodilators • 2 nd line of pharmacologic intervention • Decrease O 2 demand allow more blood to coronary arteries • Decreased pre-load • Decreased after-load • Increased blood flow to Ischemic Myocardium

Available forms: Sublingual Ointments Chewable tablets Inhalable sprays Capsules Intravenous solutions
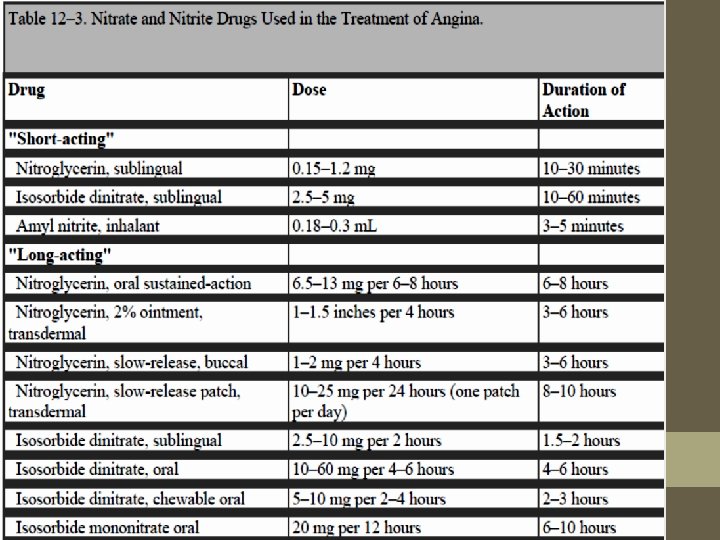

• Used to treat or prevent angina • Relieves anginal pain by relaxing smooth muscles in the blood vessels (vasodilation) by several mechanisms • Dilate veins • Dilate coronary arteries • Dilate arterioles

Adverse Effects • Headache • Usually diminish in intensity and frequency with continued use • Tachycardia • postural hypotension • Flushing • Dizziness • Tolerance may develop

Nitrate Tolerance • Occurs with chronic administration of long acting nitrates. • Efficacy of drug diminishes with chronic exposure. • To overcome this tolerance the dose schedule aims to leave your blood free of nitrate, or with very low levels of it, for a few hours each day. This is why the slow-release tablets may not be prescribed at equal intervals throughout the day. This can result in your body being free of nitrate in the early hours when you are asleep

Nitroglycerin sublingual tablets • Nitroglycerin sublingual tablets should not be chewed, crushed, or swallowed. They work much faster when absorbed through the lining of the mouth. Place the tablet under the tongue or between the cheek and gum, and let it dissolve. Do not eat, drink, smoke, or use chewing tobacco while a tablet is dissolving. • Nitroglycerin sublingual tablets usually give relief in 1 to 5 minutes. However, if the pain is not relieved, you may use a second tablet 5 minutes after you take the first tablet. If the pain continues for another 5 minutes, a third tablet may be used. If you still have chest pain after a total of 3 tablets, contact your doctor or go to a hospital emergency room right away. Do not drive yourself and call 911 if necessary.
 while you are using")
Precautions While Using nitroglycerin • Do not take sildenafil (Viagra®) while you are using nitroglycerin. Using these medicines together may cause blurred vision, dizziness, lightheadedness, or fainting. • Dizziness, lightheadedness, or fainting may occur, especially when you get up quickly from a lying or sitting position. Getting up slowly may help. Also, lying down for a while may relieve dizziness or lightheadedness. • Dizziness, lightheadedness, or fainting is also more likely to occur if you drink alcohol, stand for long periods of time, exercise, or if the weather is hot. While you are taking nitroglycerin, be careful to limit the amount of alcohol you drink. Also, use extra care during exercise or hot weather or if you must stand for long periods of time.

ANTIARRHYTHMIC DRUGS • • • Class I: Sodium Channel Blockers Class II: Beta Blockers Class III: Potassium Channel Blockers Class IV: Calcium Channel Blockers Class V: Other Antidysrhythmic Drugs

Class I – blocker’s of fast Na+ channels • Subclass IA procainamide quinidine Good oral bioavailability Used as IV to avoid hypotension Metabolized in the liver

Class IA Drugs Uses � Supraventricular and ventricular arrhythmias � Quinidine is rarely used for supraventricular arrhythmias � Oral quinidine/procainamide are used with class III drugs in refractory ventricular tachycardia patients with implantable defibrillator � IV procainamide used for hemodynamically stable ventricular tachycardia � IV procainamide is used for acute conversion of atrial fibrillation including Wolff-Parkinson-White Syndrome (WPWS)

Class IA Drugs Toxicity quinidine AV block Torsades de pointes arrhythmia because it ↑ ERP (QT interval) Shortens A-V nodal refractoriness (↑AV conduction) by antimuscarinic like effect ↑digoxin concentration by : 1 - displace from tissue binding sites 2 - ↓renal clearance Ventricular tachycardia procainamide Asystole or ventricular arrhythmia Hypersensitivity : fever, agranulocytosis Systemic lupus erythromatosus (SLE)-like symptoms: fever, pleural-pericardial inflammation. Symptoms are dose and time dependent

Class IB Drugs • They shorten Phase 3 repolarization • ↓ the duration of the cardiac action potential Class IB lidocaine mexiletine tocainide

Agents of Class IB Lidocaine � Used IV because of extensive 1 st pass metabolism � Lidocaine is the drug of choice in emergency treatment of ventricular arrhythmias � Has CNS effects: drowsiness, numbness, convulstion, and nystagmus Mexiletine � These are the oral analogs of lidocaine � Mexiletine is used for chronic treatment of ventricular arrhythmias associated with previous myocardial infarction Adverse effects: 1 - neurological effects 2 - negative inotropic activity Uses üThey are used in the treatment of ventricular arrhythmias arising during myocardial ischemia or due to digoxin toxicity üThey have little effect on atrial or AV junction arrhythmias (because they don’t act on conduction velocity)

Class IC Drugs � They markedly slow Phase 0 fast depolarization � They markedly slow conduction in the myocardial tissue Class IC flecainide propafenone Notice: Class 1 C drugs are particularly of low safety and have shown even increase mortality when used chronically after MI
 Mechanism of action � Negative inotropic and chronotropic")
Class II ANTIARRHYTHMIC DRUGS (β-adrenergic blockers) Mechanism of action � Negative inotropic and chronotropic action. � Prolong AV conduction (delay) � Diminish phase 4 depolarization suppressing automaticity(of ectopic focus) Uses � Treatment of increased sympathetic activity-induced arrhythmias such as stress- and exercise-induced arrhythmias � Atrial flutter and fibrillation. � AV nodal tachycardia. � Reduce mortality in postmyocardial infarction patients � Protection against sudden cardiac death
: was proved to reduce the incidence of")
Class II ANTIARRHYTHMIC DRUGS • Propranolol (nonselective): was proved to reduce the incidence of sudden arrhythmatic death after myocardial infarction • Metoprolol Øreduce the risk of bronchospasm selective • Esmolol: ØEsmolol is a very short-acting β 1 -adrenergic blocker that is used by intravenous route in acute arrhythmias occurring during surgery or emergencies

Class III ANTIARRHYTHMIC DRUGS K+ blockers �Prolongation of phase 3 repolarization without altering phase 0 upstroke or the resting membrane potential � They prolong both the duration of the action potential and ERP � Their mechanism of action is still not clear but it is thought that they block potassium channels

Class III sotalol amiodarone ibutilide Uses: ØVentricular arrhythmias, especially ventricular fibrillation or tachycardia ØSupra-ventricular tachycardia ØAmiodarone usage is limited due to its wide range of side effects
 • Amiodarone is a drug of multiple actions and is still not")
Amiodarone (Cordarone) • Amiodarone is a drug of multiple actions and is still not well understood • It is extensively taken up by tissues, especially fatty tissues (extensive distribution) • t 1/2 = 60 days • Amiodarone antiarrhythmic effect is complex comprising class I, III, and IV actions • Dominant effect: Prolongation of action potential duration and refractoriness • It slows cardiac conduction, works as Ca 2+ channel blocker, and as a weak βadrenergic blocker Toxicity Ø Most common include GI intolerance, tremors, ataxia, dizziness, and hyper-or hypothyrodism Ø disturbed night vision Ø Others: liver toxicity, photosensitivity, gray facial discoloration, neuropathy, muscle weakness, and weight loss Ø The most dangerous side effect is pulmonary fibrosis which occurs in 25% of the patients
 v. Calcium channel blockers decrease inward Ca")
Class IV ANTIARRHYTHMIC DRUGS (Calcium Channel Blockers) v. Calcium channel blockers decrease inward Ca 2+ currents resulting in a decrease of phase 4 spontaneous depolarization (SA node) v. They slow conductance in Ca 2+ currentdependent tissues like AV node. v. Examples: verapamil & diltiazem Because they act on the heart only and not on blood vessels.
 channels prevention of repolarization")
Mechanism of action � They bind only to depolarized (open) channels prevention of repolarization So they act only in cases of arrhythmia because many Ca 2+ channels are depolarized while in normal rhythm many of them are at rest � They prolong ERP of AV node ↓conduction of impulses from the atria to the ventricles Uses q. More effective in treatment of atrial than ventricular arrhythmias. q. Treatment of supra-ventricular tachycardia preventing the occurrence of ventricular arrhythmias q. Treatment of atrial flutter and fibrillation

contraindication q. Contraindicated in patients with pre-existing depressed heart function because of their negative inotropic activity Adverse effects q. Cause bradycardia, and asystole especially when given in combination with β-adrenergic blockers

Treatment of atrial flutter/fibrillation 1 st: Reduce thrombus formation by using anticoagulant warfarin 2 nd: Prevent the arrhythmia from converting to ventricular arrhythmia: First choice: class II drugs: • After MI or surgery • Avoid in case of heart failure Second choice: class IV Third choice: digoxin • Only in heart failure of left ventricular dysfunction 3 rd: Conversion of the arrhythmia into normal sinus rhythm: Class III: IV ibutilide, IV/oral amiodarone, or oral sotalol Class IA: Oral quinidine + digoxin (or any drug from the 2 nd step) Class IC: Oral propaphenone or IV/oral flecainide Use direct current in case of unstable hemodynamic patient
 • IV followed by oral •")
Treatment of ventricular arrhythmia Premature ventricular beat (PVB) • IV followed by oral • Early after MI First choice: class II Second choice: amiodarone Avoid using class IC after MI ↑ mortality Treatment of ventricular tachycardia • Repeat injection First choice: Lidocaine IV Second choice: procainamide IV • Adjust the dose in case of renal failure Third choice: class III drugs • Especially amiodarone and sotalol
 torsades de pointes. Classes II and IV bradycardia (don’t combine")
(IA, IC, class III) torsades de pointes. Classes II and IV bradycardia (don’t combine the two) In atrial flutter use (1 st ↓impulses from atria to ventricular to preventricular tachycardia) 1. Class II 2. Class IV 3. Digoxin. 2 nd convert atrial flutter to normal sinus rhythm use: 1. Ibutilide 2. Sotalol 3. IA or IC. If you use quinidine combine it with digoxin or β blocker (because of its anti muscarinic effect) Avoid IC in myocardial infarction because it ↑ mortality

Other Antidysrhythmic Drugs • Adenosine: • Slows conduction through the AV node • Treats SVT • Short plasma half life (less than 10 seconds) • Given IVP—closest IV site to the heart, followed by push of saline

Digoxin

pharmacology

toxicity

Clinical presentation

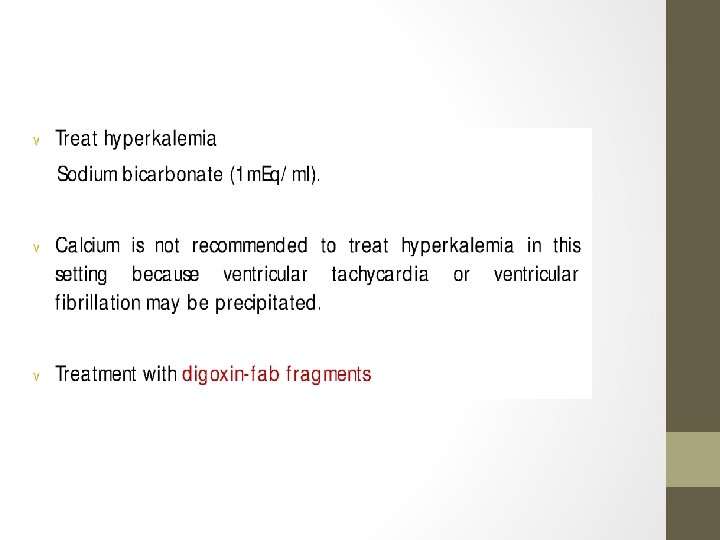
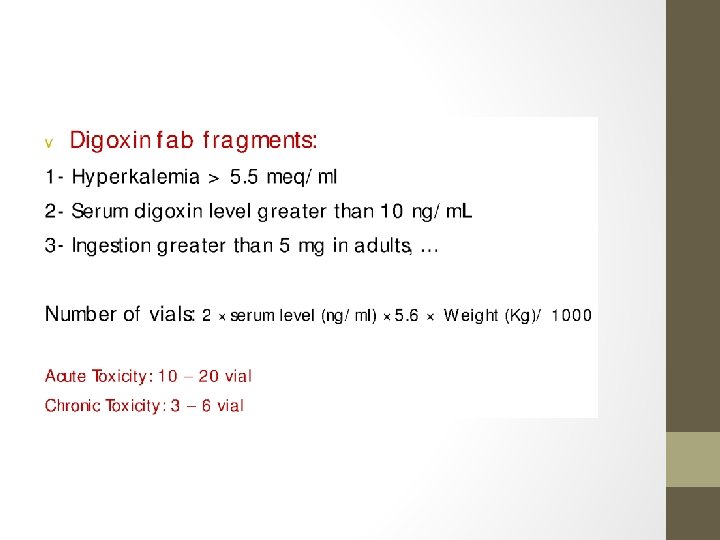
treatment
- Slides: 87