Cardiac Malpositions PRESENTER DR ANISH Cardiac Malpositions Terminology




 Dextrocardia : the")



 bend. L-loop: Leftward (“levo”) bend Cardiac looping in")











 Situs inversus")
















 Insertion (chordal attachment—straddling) Leaflet")

 Insertion (chordal attachment—straddling) Leaflet numbers Papillary muscles")


, stomach, spleen, and abdominal aorta are")





 or left atrial (polysplenia) isomerism Dextrocardia with situs ambiguus")










, surgical correction two-ventricular-type repair")

- Slides: 67
Cardiac Malpositions PRESENTER : DR ANISH
Cardiac Malpositions Terminology Looping of heart
Terminology Cardiac malposition : An abnormal intra-thoracic position of the heart. Situs : Site or position of the viscera or atria. Solitus : Normal or usual. Situs solitus : Normal position
Situs inversus: Mirror image / inversion or right/left reversal of visceral or atrial site or position Situs ambiguous : uncertain or indeterminate visceral or atrial position because of symmetric or indeterminate anatomy bilaterally
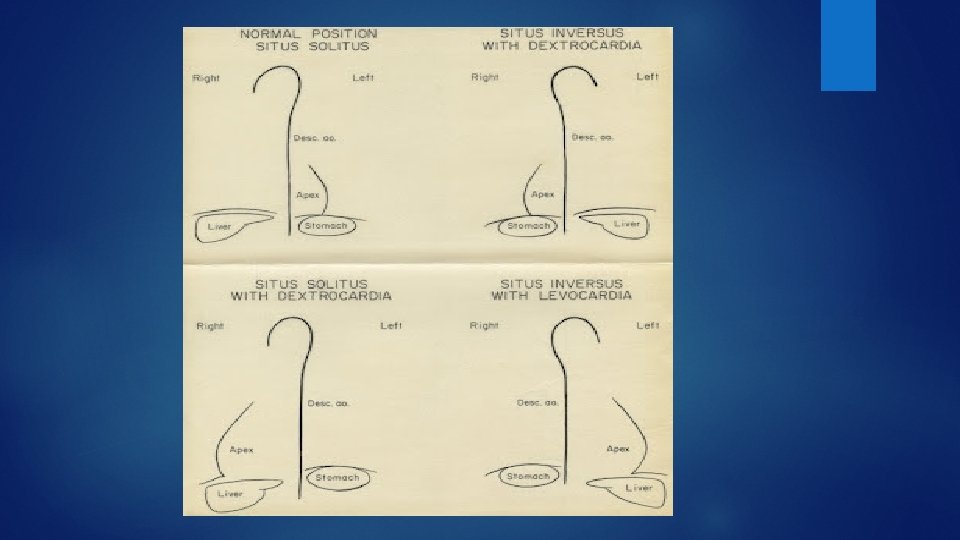
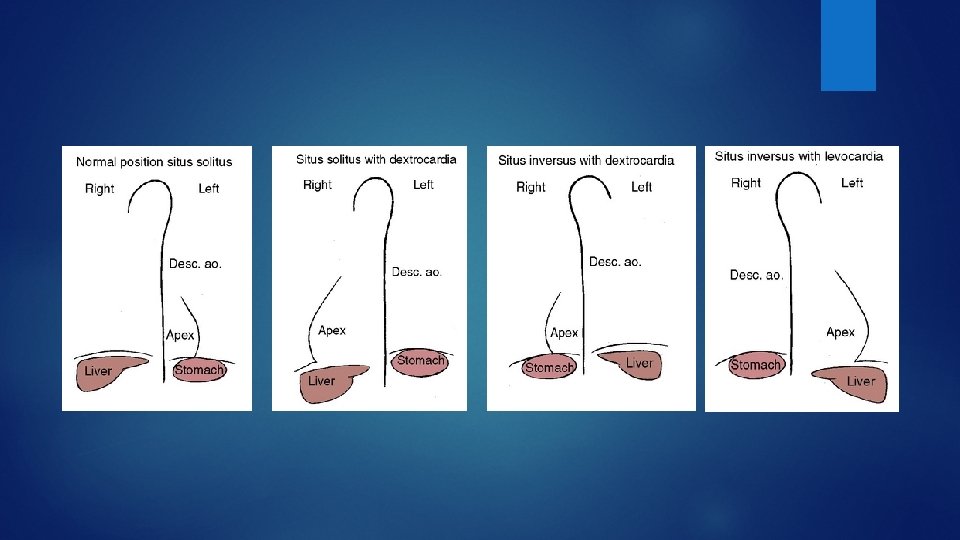
Terminology The intrathoracic Cardiac position ( levocardia / dextrocardia / mesocardia) Dextrocardia : the location of the heart in the right hemithorax with the base to apex axis to the right Mesocardia : cardiac base to apex axis directed to the midline of the thorax or with ventricular apices equally directed to both right and left sides Levocardia : cardiac location in the left hemithorax with the apex (base to apex axis) pointing to the left. Considered as cardiac malposition with situs inversus and situs ambiguus.
Terminology Displacement : An abnormal cardiac position secondary to eventration of a hemidiaphragm, agenesis of a lung, or congenital complete absence of the pericardium
Terminology Ectopia cordis : Location of the heart outside thoracic cavity
Terminology Great arterial designations: The ascending aorta and pulmonary trunk defined by their ventricle of origin and by their morphology Heterotaxy : Greek “heteros” : different and “taxis” : arrangement Isomerism : Greek “isos” : equal and “meros” part. The similarity of bilateral structures that are normally dissimilar Ø Chamber designations: Right and left
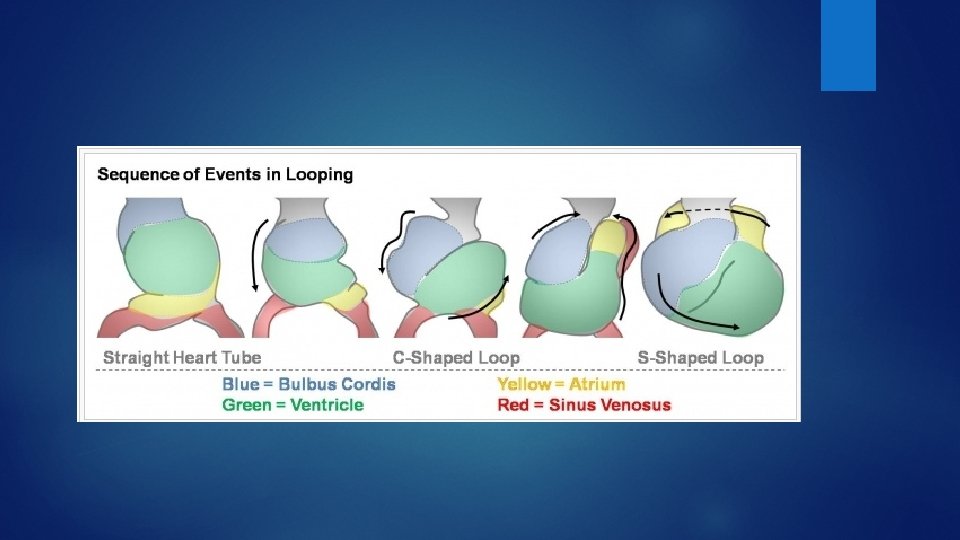
Looping of heart D-loop: Rightward (“dextro”) bend. L-loop: Leftward (“levo”) bend Cardiac looping in late fourth week and early fifth week
Looping
The straight heart tube elongates with simultaneous growth in the bulbus cordis and primitive ventricle. This forces the heart to bend ventrally and rotate to the right, forming a C-shaped loop with convex side situated on the right.
The ventricular bend moves caudally and the distance between the outflow and inflow tracts diminishes. atrium and sinus venosus become dorsal to the heart loop The atrial and outflow poles converge and myocardial cells are added, forming the truncus arteriosus.
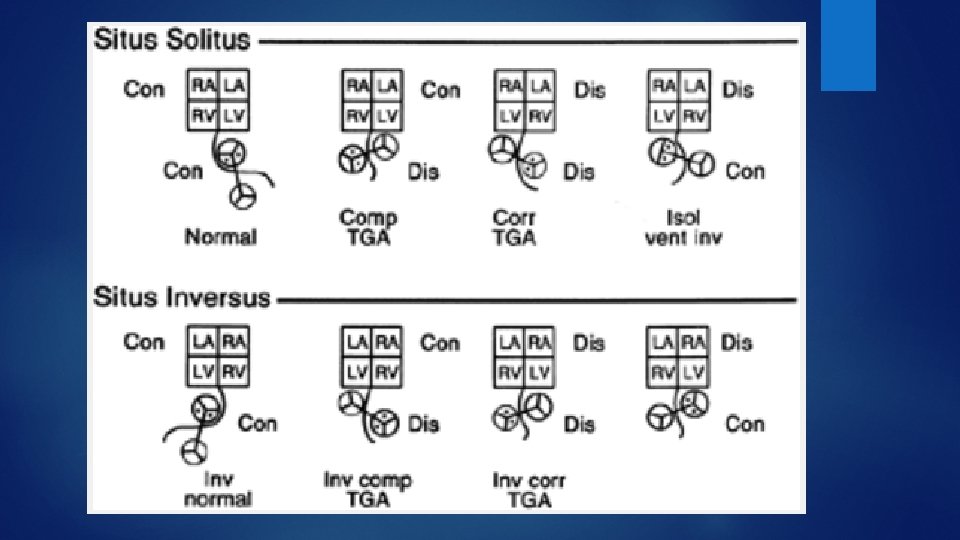
Concordance Latin “concordare” : to agree. Atrioventricular concordance: Connection of a morphologic atrium to a corresponding morphologic ventricle. Ventriculoarterial concordance: Connection of a morphologic right ventricle to a pulmonary trunk and a morphologic left ventricle to an aorta.
Discordance Latin “dis” : apart / Inappropriate. Atrio-ventricular discordance: Ventriculo-arterial discordance: A morphologic RA to LV LA to RV. A morphologic RV gives rise to the aorta, and LV to the pulmonary trunk Double discordance: Atrio-ventricular discordance together with ventriculo-arterial discordance. The result is physiologically correct circulatory flow.
Transposition of the great arteries: Each great artery arises from an anatomically discordant ventricle Malposition of the great arteries: Abnormal spatial relations of the aorta and pulmonary trunk to each other. Each of the abnormally related great arteries arises above the anatomically correct ventricle.
Situs solitus with Dextrocardia Isolated dextrocardia with AV concordance and NRGA The base-to-apex axis points to the right, so the right hemidiaphragm is lower than the left The embryonic straight heart tube initially bends rightward (d-loop) but fails to move into the left chest. Congenital heart defects: ventricular septal defect left SVC to the coronary sinus coarctation of the aorta secundum atrial septal defect anomalous pulmonary venous connections complete AV septal defect Clinical presentation depends on associated lesions
ECG atrial activation is normal, and the P-wave frontal plane axis is 70 to 80 the frontal plane QRS axis exhibits a rightward shift or right-axis deviation a gradual and progressive reduction in the QRS R-wave voltage is observed Radiographic findings heart positioned in the right chest. Volume overload lesions - evidence of pulmonary hyperperfusion. Bronchial branching patterns are normal. Visceral situs solitus is recognized by the left-sided stomach bubble and rightsided liver.
Corrected Transposition of the Great Arteries Isolated Dextrocardia with AV and VA Discordance and Left Anterior Aorta most common form of dextrocardia High incidence of associated cardiac anomalies VSD and PS DILV with hypoplastic subaortic right ventricle. Pulmonary atresia, complete AV septal defect, mitral atresia (right AV valve), tricuspid regurgitation (left AV valve) with Ebstein anomal “like malformation, anomalous systemic and pulmonary venous connections (especially with a persistent L-SVC to the RA or directly to the LA with an unroofed coronary sinus)
X-RAY & ECG findings are similar to those observed in dextrocardia with NRGA CLUE TO TGA : the initial q. R wave of the QRS complex is abnormally directed to the left consistent with abnormal septal depolarization associated with AV discordance.
Situs inversus with Dextrocardia incidence 1 in 8, 000 The thoracic and abdominal viscera are mirror images of normal morphologic right bronchus is concordant with the morphologic right atrium and a trilobed lung, SIGNIFICANCE : usually occurs with a structurally normal heart The pain of angina pectoris is in the right anterior chest and radiates to the right shoulder and right arm. The pain of appendicitis is in the left lower quadrant. Biliary colic is assigned to the left upper quadrant.
Situs inversus with Dextrocardia Inverted Normally Related Great Arteries (Left Posterior Aorta) Situs inversus totalis with persistence of normal AV and VA connections CHD : VSD TOF pulmonary atresia complete AV septal defect OS ASD. X-ray : visceral situs inversus and dextrocardia. Ecg : Atrial and ventricular voltage changes that are inverted from normal. The P-wave axis is directed to the right and inferiorly because of atrial inversion
Situs Inversus with Dextrocardia, Atrioventricular Concordance, and Ventriculoatrial Discordance with Left Anterior Aorta Inverted form of complete TGA The hemodynamics and physiology identical to TGA ECG : inverted P-wave axis because of the atrial inversion more evidence of associated right and left ventricular hypertrophy because of transposition physiology
Situs Inversus with Dextrocardia Atrioventricular and Ventriculoatrial Discordance, with Right Anterior Aorta inverted form of corrected TGA Rare the segmental cardiac connections theoretically are physiologically correct associated severe anomalies results in profound hemodynamic impairment
Situs Inversus with Dextrocardia, AV Discordance, and VA Concordance with Inverted NRGA Represents the inverted form of isolated ventricular inversion hemodynamics are comparable with those of complete TGA extremely rare cardiac abnormalities common atrium common AV valve severe right ventricular hypoplasia.
Isolated Levocardia Normal position and base to apex cardiac axis implies that either situs inversus (3% to 14% )or situs ambiguus is present. AV and VA discordance or double-outlet right ventricle with anterior right aorta : inverted form of corrected TGA AV discordance was present with atrial situs inversus : ventricular noninversion / d-loop The lungs and abdominal viscera are mirror images of normal. Associated with complex congenital heart disease
Mesocardia longitudinal axis of the heart lies in the midsagittal plane, with the heart possessing no distinct apex. very low incidence Mostly with situs solitus consisted of normal hearts VA discordance with AV discordance (corrected TGA ) VA discordance without AV discordance (complete transposition of the great arteries) Mesocardia with a d-bulboventricular loop in situs solitus is a variation of normal
Physical examination Percussion : Cardiac borders Right sided liver Left-sided stomach Cardiac dullness in supine position but turned moderately to the left and then moderately to the right, because the heart decreases to the side of the base-to-apex axis In situs solitus with a right thoracic heart, the apical right ventricle retracts, and the systemic morphologic left ventricle generates an outward systolic impulse adjacent to the lower right sternal border
Auscultation signs should be compared along the left and right sternal borders and at the cardiac apices, alternating from side to compare analogous right and left thoracic sites. Splitting of the second sound is prominent in the second intercostal space on same side of cardiac situs
ECG The direction of the P wave is determined by atrial situs unless the atrial pacemaker is ectopic In situs solitus, atrial depolarization from a right sinus node results in normal P-wave axis. In situs inversus, atrial depolarization is initiated by a left sinus node, so P waves are inverted in leads 1 and a. VL and upright in lead a. VR. A left atrial ectopic rhythm is indicated by negative P waves in lead 1 and isoelectric or negative P waves in left precordial leads. The Valsalva maneuver transiently returns an ectopic atrial focus to the right sinus node. Ø Dome and dart P wave in lead V 1/2 : a left atrial ectopic focus irrespective of atrial situs
ECG Situs inversus with Dextrocardia: reversed ventricular activation and reversed repolarization. lead 1: QRS negative & the T wave inverted, lead a. VR resembles a. VL and vice versa, right precordial leads resemble leads from corresponding left precordial sites. Septal Q waves appear in right precordial leads because septal depolarization is from right to left. The electrocardiogram can be “corrected” by reversing the limb leads and recording chest leads from the right precordium
ECG situs solitus with dextrocardia : depolarization in the frontal plane is counterclockwise Q waves in leads 1 and a. VL. prominent R waves in leads V 1 and V 2 prominent RS complexes in most of the remaining right precordial leads. Normal left-to-right septal depolarization results in Q waves at standard left precordial sites For “correcting” : limb leads unchanged, chest leads recorded from right precordial sites.
Chest x-ray The first identify the orienting letters L and R. Situs dermination Establish the cardiac axis The relative levels of the 2 hemidiaphragms Identify concordant bronchial morphology The ascending aorta is convex at the left basal aspect of the heart
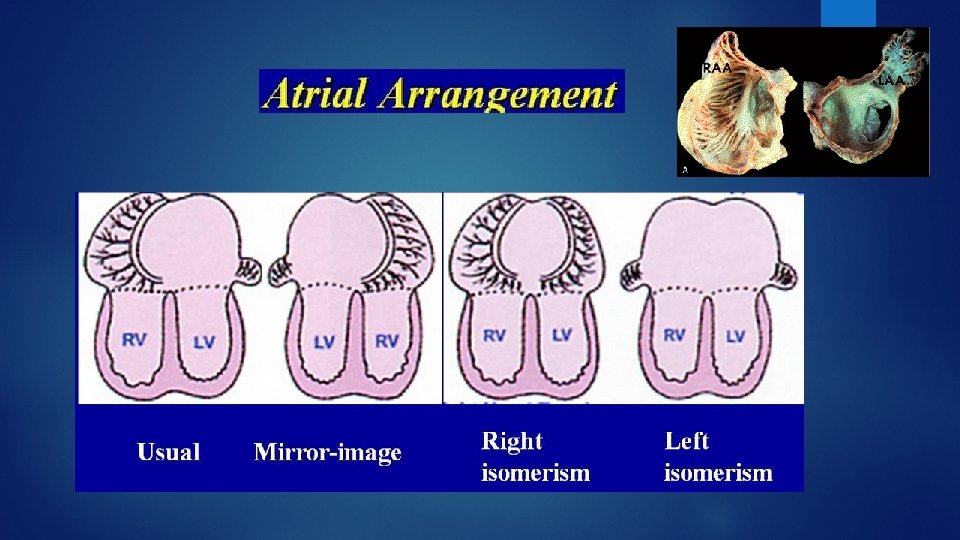
Sequential segmental analysis I: Cardiac position and apex orientation II: Atrial arrangement III: Atrioventricular connection IV: Ventriculoarterial connections V: Associated malformations and function of segment
Echocardiography with colour flow imaging Analysis A segmental sequential review of all structures involved by the congenital anomalies Sequential attention to independently addressed six segments, and position or malposition of the heart and abdominal viscera Systemic and pulmonary veins Atrial situs AV connection Ventricles and infundibulum VA connection Great arteries and ductus arteriosus
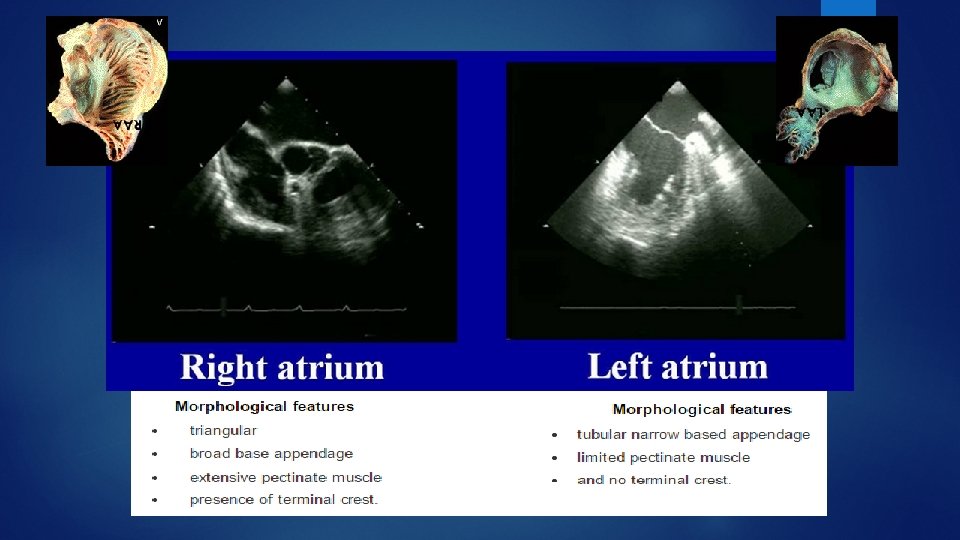
Atrial and visceral situs are generally considered together because they are usually concordant Systemic and pulmonary venous connections play a key role in the assessment of atrial situs. 1. Caval position and connection 2. Hepatic veins 3. Coronary sinus 4. Pulmonary venous connections often define the left atrium, and the suprahepatic inferior vena cava (IVC) often defines the right atrium Visceral (abdominal) situs is determined by the sidedness of the liver and stomach
The relationship between septum primum and septum secundum is the most reliable determinant of atrial situs Morphologic right atrium The inferior rim of septum secundum Best seen by echocardiography as the superior limbus of the fossa ovalis Morphologic left atrium The remnant of septum primum best seen by echocardiography as the valve of the fossa ovalis.
Atrioventricular Connections and Atrioventricular Valve Morphology Commitment (AV malalignment—overriding, crisscross) Insertion (chordal attachment—straddling) Leaflet numbers Papillary muscles (position, number, abnormality—parachute) Leaflet abnormalities (cleft, thickening—stenosis) Tricuspid valve Mitral valve Septal chordal attachments Low septal annular attachment No septal chordal attachments High septal annular attachment Triangular orifice (midleaflet) Elliptical orifice (midleaflet) Three leaflets Several papillary muscles Two leaflets Two large papillary muscles Empties into right ventricle Empties into left ventricle
Ventricular Situs and Morphology the cardiac base to apex axis ventricular locations, relationships, and morphology Cardiac position (levocardia, dextrocardia, mesocardia) Ventricular relations (anterior, posterior, superior, inferior, right, left) Papillary muscles (two discrete versus multiple irregular) Right ventricle Left ventricle Large apical trabeculations Small apical trabeculations Coarse septal surface Smooth upper surface Septal and parietal bands No septal or parietal band Receives tricuspid valve Receives mitral valve Tricuspid-pulmonary discontinuity Mitral-aortic continuity Muscular outflow tract (infundibulum) Muscular-valvular outflow tract Crescentic in cross section Circular in cross section Thin free wall (3 -5 mm) Thick free wall (12 -15 mm)
Great Artery Relations Commitment (AV malalignment—overriding, crisscross) Insertion (chordal attachment—straddling) Leaflet numbers Papillary muscles (position, number, abnormality—parachute) Leaflet abnormalities (cleft, thickening—stenosis) Eight basic types of great artery relationships are possible based on the aortic and pulmonary valve positions at the level of the semilunar valves Right posterior aorta (normally related) Right lateral aorta (side by side) Right anterior aorta (d-malposed) Directly anterior aorta Left anterior aorta (l-malposed) Left lateral aorta (left side by side) Left posterior aorta (inverted normal) Directly posterior aorta
Standard subcostal view
Cardiac position 1 location : most of the cardiac mass left / right / midline Levoposition or dextroposition or mesoposition 2. cardiac base to apex axis in subcostal four-chamber view
liver, hepatic veins, inferior vena cava (IVC), stomach, spleen, and abdominal aorta are obtained
The visceral situs is considered ambiguous because it does not conform to the classical patterns of situs solitus or inversus Their positions and venous connections can and must be accurately defined before corrective surgical procedures can be performed splenic status by locating the stomach and interrogating the area posterior and lateral to the stomach denser echocardiographic appearance than the liver and its comma-shaped curvilinear splenic vein The positions of the liver, stomach, IVC, and aorta must be individually described Polysplenia : interruption of suprahepatic portion the IVC with azygous continuation, the hepatic veins will connect directly to the atrium and a midline location of abdominal aorta
bilateral superior vena cavae direct to the ipsilateral atrium, interruption of the IVC with azygous or hemiazygous continuation to the superior vena cava (SVC), and various anomalous pulmonary venous connections Direct pulmonary venous connections to the ipsilateral atrium, as well as complete or partial connections to the right or left superior vena cava
Pulmonary situs defined by the relationship of the pulmonary arteries to their adjacent bronchi In a morphologic right lung, the pulmonary artery travels anterior to the upper lobe and intermediate bronchi. In contrast, a morphologic left lung is characterized by a pulmonary artery that courses over the main bronchus and posterior to the upper lobe bronchus the distance from the carina to the origin of the upper lobe bronchus is 1. 5 to 2 times greater for the morphologic left lung than for the right lung
Cardiac segments are evaluated not only according to morphology but also in terms of spatial orientation the position and orientation of the ventricular septum determine the location of the ventricular chambers levocardia, therefore, the ventricles are right anterior and left posterior. in dextrocardia they usually are right posterior and left anterior Mesocardia is characterized by a vertical midline septum
Echo modified from the right or left parasternal and subcostal positions to adequately delineate VA connections and great artery relationships Parasternal long- and short-axis scans are particularly helpful in determining concordant, discordant, or double-outlet connections suprasternal scans should be obtained to assess the proximal pulmonary and aortic arch anatomy. The aortic arch should be determined as right or left sided and the brachiocephalic branching pattern defined. position of the aorta is described relative to the pulmonary trunk right posterior aorta
Situs Ambiguus right atrial (asplenia) or left atrial (polysplenia) isomerism Dextrocardia with situs ambiguus was the most common
Heterotaxy with right isomerism Greek “heteros”: different and “taxis”: arrangement Isomerism (from the Greek “isos, ” equal) similarity of bilateral structures that are normally morphologically asymmetric Strong concordance between a morphologic right bronchus, a trilobed right lung, and a morphologic right atrial appendage In right isomerism, the bronchi are symmetric morphologic right, the lungs are trilobed, and the atrial appendages exhibit right morphologic features.
Situs ambiguus with asplenia Cardiac : The sinus nodes are paired because bilateral superior vena cavae are attached to bilateral morphologic right atria. The P-wave axis is normal because the right sinus node is usually the dominant atrial pacemaker The atrioventricular conduction system is equipped with 2 nodes often connected by a sling of tissue Supraventricular tachycardia is attributed to reentry between paired atrioventricular nodes. relatively consistent relation between the type of isomerism and the type of congenital heart disease common atrium, common atrioventricular valve, morphologicsingle ventricle, functional single ventricle (hypoplasticright or left), pulmonary stenosis or atresia, absent coronary sinus, total anomalous pulmonary venous connection bilateral ductus arteriosus. Ventricular and great arterial connections are usually discordant.
Noncardiac midline abnormalities tracheoesophageal fistula, meningomyelocele, encephalocele, cerebellar agenesis, cleft lip, cleft palate, and horseshoe kidney. Lungs : bilateral morphologic right bronchi, bilateral trilobed lungs Abdomen : The spleen is the only organ that is left-sided from its inception, because it develops in the left side of the dorsal mesogastrium. A relation exists between right isomerism and asplenia 5% of cases, however, a normal-sized spleen resides in the right upper quadrant. Howell-Jolly bodies and Pitted red cells in peripheral blood smears A wandering spleen can be mistaken for absence Gastrointestinal disorders include biliary atresia and intestinal malrotation, transverse liver
Asplenia / Ivemark syndrome normal birth weight male predominance Neonatal cyanosis is invariable, conspicuous, and often evident in the first 24 hours Survival is determined largely by coexisting congenital heart disease and noncardiac disorders Most deaths occur within the first few months
X-ray : discloses a transverse liver, bilaterally symmetric bronchi overpenetrated chest x-ray to determine whether the bronchi are symmetric right or symmetric left Thoracic echocardiography identifies morphologic right and left atrial appendages Abdominal USG discloses a transverse liver, an aorta that is anterior to or on the same side of the spine as the inferior vena cava, and hepatic veins that drain into the inferior cava as it joins a right-sided atrium. A spleen cannot be detected.
Heterotaxy with left isomerism: more prevalent in women bilateral morphologic left bronchi, bilateral morphologic bilobed lungs, bilateral morphologic left atrial appendages, bilateral superior vena cavae attached to bilateral morphologic left atria, an absent or atretic sinoatrial node, common atrium, common atrioventricular valve, atrioventricular septal defect, and partial anomalous pulmonary venous connection. The pulmonary veins can be connected in a symmetric fashion, 2 to the right-sided atrium and 2 to the left-sided atrium
polysplenia syndrome The most distinctive and therefore the most diagnostically useful clinical feature is inferior vena caval interruption with azygous continuation, in which the suprarenal segment of the inferior cava is absent, and the infrarenal segment continues as the azygos or hemiazygous vein Fetal complete heart block is presumptive evidence of in utero left isomerism Intrauterine loss for fetuses with left isomerism is greater Polysplenia characterized by a cluster of multiple splenules
Morbidity and mortality are determined by coexisting cardiovascular malformations and by noncardiac anomalies, which are usually gastrointestinal(malrotation, biliary atresia, esophageal atresia and congenital short pancreas) 20% die as neonates; 50% do not survive adolescence vena caval connections are necessarily to a morphologic left atrium, so the sinus node is absent or hypoplastic. The atrial pacemaker is therefore ectopic, and the P-wave axis is abnormal. The ectopic atrial pacemaker can shift from 1 site to another or may fire slowly (ectopic atrial bradycardia). Atrial fibrillation and atrial flutter are occasional. Complete atrioventricular block occurs in approximately 1 in 5 cases blocked at the level of the penetrating bundle, resulting in nodoventricular discontinuity and a narrow QRS interval
transverse liver is accompanied by symmetric left bronchi, heart is usually left sided. The stomach tends to be on the side opposite the descending aorta. Inferior vena caval interruption with azygous continuation is best identified on the frontal chest x-ray The aorta and inferior vena cava lie anterior to or on the same side of the spine. When there is inferior vena caval interruption with azygous continuation, hepatic veins connect directly to the atrium without joining the inferior cava
Lower incidence of associated pulmonary outflow tract obstruction and a more frequent occurrence of bilateral pulmonary venous connections to the ipsilateral atrium common-inlet ventricle of right ventricular morphology and double-outlet right ventricle Most common complex : dextrocardia, atrial situs ambiguus, ventricular inversion, and VA concordance with left posterior aorta.
Treatment depend on the specific lesion encountered conotruncal abnormalities (TGA/DORV), surgical correction two-ventricular-type repair such as an arterial switch procedure (Jatene, Kaye–Damus–Stansel, or Aubert procedure), or ventricular septal defect (VSD) closure connecting the systemic ventricle to the aorta, transsection of the pulmonary artery, and establishment of pulmonary ventricle to pulmonary artery continuity with an extracardiac conduit.
complex malformations associated with situs ambiguous common atrium with common-inlet single ventricle or unbalanced ventricles, and complex malformations associated with criss-cross AV relations and severe AV valve straddling surgical palliation directed toward function as a single ventricle such as with systemic–pulmonary artery shunts, Glenn-type shunts, bidirectional cavopulmonary shunts, and finally the modified Fontan procedures special efforts must also be directed toward surgical establishment of appropriate venous connections or relief of venous stenosis Medical management of complications of progressive hypoxia and polycythemia, progressive ventricular fibrosis, and ventricular failure, stroke, and brain abscess associated with such lesions