CARDIAC GLYCOSIDES Part 2 By Darakhshan rizvi CIMS
 By: Darakhshan rizvi CIMS")
CARDIAC GLYCOSIDES (Part 2) By: Darakhshan rizvi CIMS

OVERVIEW § Therapeutic uses of digitalis § Digitalisation § Digitoxin toxicity § Dobutamine § Other drugs used in heart failure

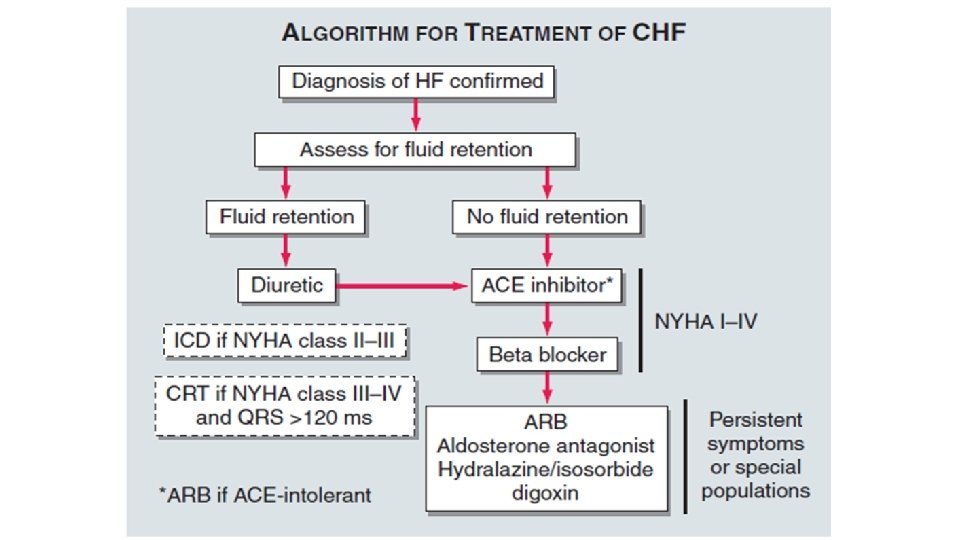
CARDIAC GLYCOSIDES- CLINICAL PEARLS Therapeutic Uses 1. Heart failure with atrial fibrillation (use only when diuretics and ACEI have failed to control the symptoms) – Mild symptoms – slow loading dose – Acute heart failure – rapid digitalization 2. Treatment of atrial arrhythmia (atrial fibrillation & flutter) Used for Acute treatment of CHF as well as for maintainence therapy. Useful in cardiac failure due to ischaemia, hypertension and valvular heart disease.
: Orally A loading dose of 1 -1. 5")
Digitalization Rapid Digitalization (within 24 h): Orally A loading dose of 1 -1. 5 mg is administered over 24 hours in divided doses (0. 5 mg initial dose with 0. 25 mg every 6 h) Monitoring of signs of improvement and toxicity if response is not adequate with loading dose It is followed by dose increment (0. 125 -0. 375 mg) so as to achieve plasma concentration of 0. 5 -1. 8 ng/ml The maintenance dose should be administered once a day as its t 1/2 is about 40 hours.
: IV A loading dose of 0. 5")
Digitalization Very Rapid Digitalization (within 24 h): IV A loading dose of 0. 5 -1. 0 mg is administered over 3 -6 hours in divided doses (0. 25 mg initial iv dose with 0. 1 mg every hour) by slow iv Close monitoring (heart rate, BP, ECG) and signs of therapeutic response for the treatment of termination of PSVT or for heart failure
 Sinus bradycardia b) Ventricular tachyarrythmia c) Ventricular arrhythmias")
DIGITALIS- A/E • Cardiac effects: a) Sinus bradycardia b) Ventricular tachyarrythmia c) Ventricular arrhythmias d) Supraventriculkar arrhythmias • CNS effects- Dizziness, mental confusion • Occular disturbances- Halos , photophobia, blurred vision • GIT disturbances- Anorexia, Nausea, Vomiting • Gynaecomastia in males, and breast enlargement in females

DIGOXIN TOXICITY

DIGOXIN TOXICITY- Treatment 1. Shift the patient to ICU 2. Stop digoxin and K+ depleting diuretics (thiazides/loop diuretics) 3. KCl orally or i. v. is the DOC for tachyarrythmias when serum K+ levels is normal/low 4. Supraventricular arrhythmias are treated with oral or iv propranolol 5. IV lignocaine is DOC for ventricular arrhythmias 6. Digoxin antibodies (Digibind): used only in case of serious digitalis toxicity

IONOTROPIC AGENTS- DOBUTAMINE β 1 in Heart β 2 in Periphery • Ionotropic effect • Chronotropic Effect • ↓ Peripheral Vascular Resistance • Vasodilation • ↑ Renal Blood Flow Dobutamine is used in the starting dose of 2 -3µg/kg/min IV, and modified or decreased as per the response Response is assessed by measuring COP and PCWP

IONOTROPIC AGENTS- DOPAMINE • Dopamine has limited utility in CHF and is not preferred over dobutamine • Exhibits dose- dependent effects 2 -5 µg/kg/min Renal and mesenteric DA receptors Renal and mesenteric vasodilation 5 -10 µg/kg/min 10 -20 µg/kg/min Cardiac β 1 receptors Vascular �receptors Positive ionotropic with little chronotropic effect Vasocontriction and rise in BP (Ionoconstrictor)

IONOTROPIC AGENTS- DOPEXAMINE • Dopexamine is a synthetic agent related to dopamine but it possesses activity at D 1 D 2 and β 2 receptors. • It increases stroke volume and reduces peripheral vascular resistance in patients with low cardiac output, however hypotension and tachycardia may occur.

Phosphodiesterase Inhibitors Effects: Positive myocardial inotropism and dilation of resistance and capacitance vessels. ATP GTP Improvement in cardiac output through ionotropy and by decreasing preload and afterload. c. AMP c. GMP AMP GMP Inactive Substrates PDE Inhibitors PDE-3 Inhibitor: Inamrinone and Milrinone Approved for short-term circulation support in advanced CHF PDE-5 Inhibitor: Sildenafil Use limited to those with isolated right ventricular systolic failure from pulmonary artery hypertension

Phosphodiesterase Inhibitors- Levosimendan MOA LEVOSIMENDAN Inhibits PDE and thus raises the conc. Of c. AMP Sensitizes the cardiac muscle to the action of Ca 2+

NATRIURETIC PEPTIDES ANP Secreted from atrial cardiac myocytes BNP Secreted from ventricular cardiac myocytes A correlation has been found in the circulating level of circulating BNP level and degree of heart failure Hence BNP used for diagnostic as well as prognostic purposes DIURESIS NATRIURESIS VASODILATION

NATRIURETIC PEPTIDES- NESIRITIDE • Nesiritide is a recombinant BNP. • It has diuretic and vasodilator effect with short term infusion. • Nesiritide increases the secretion of Na+ through the kidney, so long term use may precipitate kidney damage. GUIDELINES • Nesiritide is preferred over inotropic agents to relieve dyspnoea in patients of refractory heart failure mainly in cases with risk of arrhythmia. • Initial loading dose (2µg/kg) IV infusion (0. 01µg/kg/min ) * NEWER DRUGS- Carperitide and ularitide are similar to nesiritide and they are under evaluation

DIURETICS – Loop Diuretics • Loop Diuretics act by causing inhibition of Na+ K+ 2 Cl- symporter present at the luminal membrane of the Ascending Limb of Lo. H. • Furosemide, Torsemide, Bumetanide, Ethacrynic Acid are important members of this group. • Faster acting – Short Duration of action

DIURETICS FUROSEMIDE • Possesses vasodilatory action which is responsible for quick relief in LVF and pulmonary oedema (used iv) • DOSE: Furosemide 40 mg bolus followed by i. v. infusion at a rate of 10 mg/hour and increased as per the requirement. • Ascitis due to CHF: Furosemide 20 mg + Spironolactone 50 mg THIAZIDES • These drugs act by inhibiting Na+ Cl- symporter at the luminal membrane of early DT. • Thiazides are used to mobilize the edema fluid in mild to moderate heart failure.
 Aldosterone- Sensitive Na+ Channel")
DIURETICS K+ SPARING DIURETICS ATP- Dependent Na+/K+ Pump (Amiloride; Triamterene) Aldosterone- Sensitive Na+ Channel (Spironolactone; Eplerenone) Are less effective when used alone, however when used in combination with other diuretics they increase their efficacy and reduce the toxicity by reducing renal loss of K+ and Mg+

GUIDELINES FOR USING DIURETICS IN HEART FAILURE AIM: To achieve euvolaemia Prolonged use of loop diuretics is to restore euvolaemia and if there is retention of fluid furosemide can be started with a dose of 40 mg once or twice a day and dose is further increased gradually till the desired response is achieved i. e. diuresis and reduced body mass Subsequently this is followed by minimal dose that can maintain the euvolemia achieved. Loop diuretic is preferred, however if salt and water retention is severe then thiazides should also be used with furosemide. Hypokalemia is likely to occur and this can be corrected by the supplementation of potassium or simultaneous use of potassium sparing diuretics

LIMITATIONS OF DIURETIC THERAPY Electrolyte Imbalance Diuretic Resistance - Poor patient complaince

ACE Inhibitors Captopril, Enalapril, Lisinopril, Perindopril, Ramipril

Release of ANP and Endothelin ↑Afterload Catecholamine Release Myocardial Hypertrophy Death of Myocardial Cells

ACE Inhibitors- Mechanism SHORT TERM MECHANISM LONG TERM MECHANISM ACE Inhibitors cause both Arterial and Venous dilatation and reduction in both the systemic and pulmonary artery resistance. Thus there is reduction in both the preload and afterload.
 In all patients with a recent or")
ACE Inhibitors- Clinical Pearls • Indicated: a) In all patients with a recent or remote history of MI or Acute Coronary Syndrome and reduced EF b) To prevent symptomatic HF c) In all patients with a reduced EF to prevent symptomatic HF • ACEI are used for the treatment of heart failure of all grades (NYHA grade I to IV. ) They are also indicated in cases of asymptomatic left ventricular dysfunction. • The starting dose should be smaller (Captopril 6. 25 mg/ Lisinopril 5 mg/ Ramipril 5 mg) and then gradually the dose may be increased to the desired response and the tolerated dose over days or weeks.
 Losartan, Valsartan, Irbesartan, Telmisartan and Eprosartan MOA • ARBs block")
A-II Receptor Blockers (ARBs) Losartan, Valsartan, Irbesartan, Telmisartan and Eprosartan MOA • ARBs block the AT-1 receptors they block all the actions of A-II and the effect is continued even if the level of A-II comes back to initial value on prolonged use due to synthesis of A-II by other pathways. • ARBS should be used as an alternative in cases where ACEI cannot be used due to any reason.
 ADVANTAGE ARBS are better tolerated due to a better side")
A-II Receptor Blockers (ARBs) ADVANTAGE ARBS are better tolerated due to a better side effect profile. DISADVANTAGE The beneficial effects/ changes which occur due to accumulation of bradykinin are absent when treated with ARBs Combination of ACEI and ARBs should prove to be more useful than either agent used alone due to their different modes of action

β- ADRENERGIC BLOCKERS Myocardial Insult Left Ventricular Dysfunction ↑ Activity of RAAS and SNS Accelerate Cardiac Remodelling & worsen myocardial function ↓ Sympathetic Overactivity Role of β ↓ Heart Rate and optimizing blockers myocardial O 2 demand ↓ Myocardial apoptosis and fibrosis ↓ Cardiac Remodelling

β- ADRENERGIC BLOCKERS- CLINICAL PEARLS • Greatest utility of B blockers has been shown in mild to moderate (NYHA class I, III) cases of DCM with systolic dysfunction in which they are now routinely co-prescribed unless contraindicated. • Encouraging results have been obtained in class IV cases as well, but use in severe failure could be risky and needs constant monitoring. • There is no place for B blockers in decompensated patients. B blockers should be stopped during an episode of acute heart failure and recommenced at lower doses followed by up-titration after compensation is restored. Conventional therapy should be continued along with them.

β- ADRENERGIC BLOCKERS- CLINICAL PEARLS • Starting dose should be very low-then titrated upward as tolerated to target level. • A long-acting preparation (e. g. sustained release metoprolol) or 2 -3 times daily dosing to produce round-the-clock β blockade should be selected.

β- ADRENERGIC BLOCKERS- CLINICAL PEARLS • Beta blockers should not be administered to patients with heart failure who have bradycardia, heart block or hemodynamic instability. • Should not be given in patients of ashthma.

HYDRALAZINE • Directly acting vasodilator • MOA: Hydralazine molecules combine with receptors in the endothelium of arterioles– NO release – Relaxation of vascular smooth muscle – fall in BP • Hydralazine is useful in heart failure by reducing both pulmonary and systemic vascular resistance. • It produces arteriolar vasodilation and thus it reduces the afterload, but has negligent effect on veins (capacitance vessels)

HYDRALAZINE- CLINICAL PEARLS • Hydralazine may be preferred in patients of heart failure with renal dysfunction as hydralazine increases the renal blood flow by reducing the renal vascular resistance. • It is useful in combination with or without some venodilator such as IDN in patients of heart failure who are already taking diuretics, ACEI and digoxin. • Starting dose 10 -20 mg TDS – Increased upto 100 mg TDS over days or weeks depending on the requirement or response achieved

HYDRALAZINE- SIDE EFFECTS • • • Hypotension Headache Hypersensitivity SLE GI Upset

CALCIUM CHANNEL BLOCKERS MOA CCBs block voltage- sensitive L-type Ca 2+ channels by binding to � 1 subunit Prevent entry of Ca 2+ into the cell and reduce the frequency of Ca 2+ channel opening Decrease activity of heart - ↓ HR - ↓AV Conduction - ↓ Contractility Relaxation of smooth muscles in blood vessels (Vasodilation)

CALCIUM CHANNEL BLOCKERS Dihydropyridines Nifedipine, Amlodipine, Nicaripine, Felodipine, Isradipine, Nisoldipine Short Acting: May lead to reflex tachycardia, so not used. Long Acting: Effective as they reduce afterload but reflex tachycardia is minimal Phenylalkylamine Verapamil Negative Ionotropic Effect, so not used. Benzothiazepine Diltiazem Negative Ionotropic Effect, so not used. Clinical Trials on the role of CCBs for CHF have provided inconclusive results.

CALCIUM CHANNEL BLOCKERS- ADRs Nifedipine • • Hypotension Palpitation Reflex Tachycardia Oedema Flushing Dizziness Sedation Verapamil • • • Constipation Sinus Bradycardia Oedema AV block Headache Diltiazem • • • Headache Hypotension Bradycardia Oedema AV Block

VASOPEPTIDASE INHIBITOR Sampatrilat, Omapatrilat, Fasidotrilat Neutral Endopeptidase Ѳ VASOPEPTIDASE INHIBITORS ↑ Natriuretic Peptide • Improves cardiac function in heart failure patients • A/E- Angioedema, cough and dizziness Ѳ Angiotensin Converting Enzyme ↓ Angiotensin II

VASOPRESSIN RECEPTOR ANTAGONISTS LOW CARDIAC OUTPUT Brain releases VASOPRESSIN Vaptans block Vasopressin V 1 receptor antagonists may be useful when total peripheral resistance is increased. Relcovaptan- Selective V 1 antagonist Conivaptan- V 1 A/V 2 receptor outcome

ENDOTHELIN RECEPTOR BLOCKERS Endothelin 1 Bosentan, Tezosentan • Bosentan is a non- selective endothelin antagonist used orally and proved useful in animal models of heart failure • Tezosentan is another endothelin antagonist and is under evaluation for treatment of heart failure. • Sitaxentan and Ambrisentan are ETA selective antagonist and these may prove useful in heart failure. Prepro ET Big ET ET Converting Enzyme (ECE) Mature ET RECEPTORS ET-A Vascular Smooth Muscle Vasoconstriction ET-B Endothelial Cells Release of NO
 is responsible for conversion of big ET 1")
PHOSPHORAMIDON • Endothelin converting enzyme (metalloprotease) is responsible for conversion of big ET 1 to intracellular ET 1. Endothelin 1 Prepro ET Big ET ET Converting Enzyme (ECE) Mature ET • Phosphoramidon is an inhibitor of this enzyme and thus prevents the RECEPTORS action of endothelin and so its use is similar to endothelin receptor ET-B ET-A antagonist, if found suitable. Vascular Smooth Muscle Vasoconstriction Endothelial Cells Release of NO

Ivabradine: A Sinoatrial node modulator Ivabradine increases stroke volume, fully preserves myocardial contractility and relaxation, atrioventricular conduction, and ventricular repolarization, as well as blood pressure.

NEWER DRUG TAGETS • Newer Inotropes • • Cardiac myosin activators- Omecamtiv mecarbil Na/K-ATPase inhibitors- Istaroxime Ryanodine receptor stabilizers- JTV-519(K 201), S 107, S 44121 SERCA 2 a activators- MYDICAR • Vasodilators- Relaxin • Neuregulins • recombinant human NRG-1β 2 • Novel RAAS blockers • Direct renin inhibitors- Oral Aliskiren, IV Remikiren, IV Enalkiren • Angiotensin receptor & neprilysin inhibitors- LCZ 696, AHU 377 , Candoxatril, Ecadotril • Aldosterone blockers • Non steroidal minrelocorticoid receptor antagonist-PF 3882845, BR-4628 • Aldosterone synthase inhibitors- FAD 286, LCI 699

CLINICAL SUMMARY STAGE A High Risk with No Symptoms

CLINICAL SUMMARY STAGE B Structural Heart Disease, No Symptoms

CLINICAL SUMMARY STAGE C Structural Heart Disease, Previous or Current Symptoms

CLINICAL SUMMARY STAGE D Refractory Symptoms requiring special intervention

Physician expertise and the ability to improve clinical outcomes can make a genuine difference in the lives of heart failure patients

- Slides: 50