Cardiac Circulation Blood in the heart chambers does

Cardiac Circulation • Blood in the heart chambers does not nourish the myocardium • The heart has its own nourishing circulatory system consisting of: • Coronary arteries—branch from the aorta to supply the heart muscle with oxygenated blood • Cardiac veins—drain the myocardium of blood • Coronary sinus—a large vein on the posterior of the heart, receives blood from cardiac veins • Blood empties into the right atrium via the coronary sinus https: //www. youtube. com/watch? v=3_PYn. WVo. Uz. M

Brachiocephalic trunk Left common carotid artery Superior vena cava Left subclavian artery Right pulmonary artery Aortic arch Ascending aorta Pulmonary trunk Right pulmonary veins Right atrium Right coronary artery in coronary sulcus (right atrioventricular groove) Anterior cardiac vein Right ventricle Marginal artery Small cardiac vein Inferior vena cava (a) Ligamentum arteriosum Left pulmonary artery Left pulmonary veins Left atrium Auricle of left atrium Circumflex artery Left coronary artery in coronary sulcus (left atrioventricular groove) Left ventricle Great cardiac vein Anterior interventricular artery (in anterior interventricular sulcus) Apex

Blood Flow Through the Heart • Superior and inferior venae cavae dump blood into the right atrium • From right atrium, through the tricuspid valve, blood travels to the right ventricle • From the right ventricle, blood leaves the heart as it passes through the pulmonary semilunar valve into the pulmonary trunk • Pulmonary trunk splits into right and left pulmonary arteries, which carry blood to the lungs

Blood Flow Through the Heart • In the lungs, blood picks up oxygen and drops off carbon dioxide • Oxygen-rich blood returns to the heart through the four pulmonary veins • Blood enters the left atrium and travels through the bicuspid valve into the left ventricle • From the left ventricle, blood leaves the heart via the aortic semilunar valve and aorta

Capillary beds of lungs where gas exchange occurs Pulmonary Circuit Pulmonary arteries Pulmonary veins Aorta and branches Venae cavae Left atrium Right atrium Left ventricle Heart Right ventricle Systemic Circuit KEY: Oxygen-rich, CO 2 -poor blood Oxygen-poor, CO 2 -rich blood Capillary beds of all body tissues where gas exchange occurs

Pathway of Blood Through Heart • Right side of the heart • • Superior vena cava (SVC), inferior vena cava (IVC), and coronary sinus Right atrium Tricuspid valve Right ventricle Pulmonary semilunar valve Pulmonary trunk Pulmonary arteries Lungs

Pathway of Blood Through Heart • Left side of the heart • • Four pulmonary veins Left atrium Mitral valve Left ventricle Aortic semilunar valve Aorta Systemic circulation
 Inferior vena cava (IVC) Coronary sinus Right atrium Tricuspid valve")
Superior vena cava (SVC) Inferior vena cava (IVC) Coronary sinus Right atrium Tricuspid valve Right ventricle Pulmonary semilunar valve Oxygen-poor blood Pulmonary trunk Pulmonary arteries SVC Coronary sinus Right atrium IVC Pulmonary trunk Tricuspid valve Right ventricle Pulmonary semilunar valve Oxygen-poor blood is carried in two pulmonary arteries to the lungs (pulmonary circuit) to be oxygenated. To lungs Pulmonary capillaries Oxygen-rich blood returns to the heart via the four pulmonary veins. To heart Oxygen-rich blood

To heart Oxygen-poor blood returns from the body tissues back to the heart. Oxygen-poor blood Oxygen-rich blood Systemic capillaries To body Oxygen-rich blood is delivered to the body tissues (systemic circuit). Aorta Pulmonary veins Aortic semilunar valve Left atrium Mitral valve Left ventricle Aorta Aortic semilunar valve Left ventricle Mitral valve Left atrium Four pulmonary veins
 Inferior vena cava (IVC) Coronary sinus Right atrium Tricuspid valve")
Superior vena cava (SVC) Inferior vena cava (IVC) Coronary sinus Right atrium Tricuspid valve Right ventricle Oxygen-poor blood Pulmonary semilunar valve Pulmonary trunk Pulmonary arteries SVC Coronary sinus Pulmonary trunk Right atrium Tricuspid valve Pulmonary semilunar valve Right ventricle IVC To heart Oxygen-poor blood is carried in two pulmonary arteries to the lungs (pulmonary circuit) to be oxygenated. Oxygen-poor blood returns from the body tissues back to the heart. Systemic capillaries To body To lungs Pulmonary capillaries Oxygen-rich blood returns to the heart via the four pulmonary veins. Oxygen-rich blood is delivered to the body tissues (systemic circuit). Aorta To heart Pulmonary veins Aortic semilunar valve Left atrium Mitral valve Left ventricle Aorta Aortic semilunar valve Left ventricle https: //www. youtube. com/watch? v=BEWj. OCVEN 7 M Mitral valve Left atrium Four pulmonary veins Oxygen-rich blood

• Equal volumes of blood are pumped to pulmonary and systemic circuits • Pulmonary circuit is short, low-pressure circulation • Systemic circuit is long, high-friction circulation • Anatomy of ventricles reflects differences • Left ventricle walls are 3 times thicker than right • Pumps with greater pressure

Coronary Circulation • Coronary circulation • • Functional blood supply to heart muscle itself Shortest circulation in body Delivered when heart is relaxed Left ventricle receives most of coronary blood supply

• Coronary arteries • Both left and right coronary arteries arise from base of aorta and supply arterial blood to heart • Both encircle heart in coronary sulcus • Branching of coronary arteries varies among individuals • Arteries contain many anastomoses (junctions) • Provide additional routes for blood delivery • Cannot compensate for coronary artery occlusion • Heart receives 1/20 th of body’s blood supply

• Left coronary artery supplies interventricular septum, anterior ventricular walls, left atrium, and posterior wall of left ventricle; has two branches: • Anterior interventricular artery • Circumflex artery • Right coronary artery supplies right atrium and most of right ventricle; has two branches: • Right marginal artery • Posterior interventricular artery
 Left coronary")
Aorta Pulmonary trunk Superior vena cava Left atrium Anastomosis (junction of vessels) Left coronary artery Right atrium Circumflex artery Right coronary artery Right ventricle Right marginal artery Left ventricle Anterior interventricular artery Posterior interventricular artery

• Coronary veins • Cardiac veins collect blood from capillary beds • Coronary sinus empties into right atrium; formed by merging cardiac veins • Great cardiac vein of anterior interventricular sulcus • Middle cardiac vein in posterior interventricular sulcus • Small cardiac vein from inferior margin • Several anterior cardiac veins empty directly into right atrium anteriorly

Superior vena cava Great cardiac vein Anterior cardiac veins Coronary sinus Small cardiac vein Middle cardiac vein

Problems • Angina pectoris • Thoracic pain caused by fleeting deficiency in blood delivery to myocardium • Cells are weakened • Myocardial infarction (heart attack) • Prolonged coronary blockage • Areas of cell death are repaired with noncontractile scar tissue

Aorta Left pulmonary artery Superior vena cava Right pulmonary artery Right pulmonary veins Left pulmonary veins Auricle of left atrium Left atrium Right atrium Inferior vena cava Great cardiac vein Coronary sinus Posterior vein of left ventricle Right coronary artery (in coronary sulcus) Left ventricle Posterior interventricular artery (in posterior interventricular sulcus) Middle cardiac vein Apex Posterior surface view Right ventricle

A “heart attack” is also known as • angina. • pericarditis. • congestive heart failure. • myocardial infarction.

A “heart attack” is also known as • angina. • pericarditis. • congestive heart failure. • myocardial infarction.

Intrinsic Conduction System of the Heart: Setting the Basic Rhythm • Cardiac muscle is able to initiate its own contraction in a regular way, but its rate is influenced by both intrinsic and extrinsic factors • The intrinsic conduction (nodal) system increases the rate of heart contraction and ensures that the heart beats as a unit This is very similar to the one-way generation of action potentials that travel down the axon. The signals that stimulate cardiac muscle contraction also travel one-way throughout the intrinsic conduction system.

• Coordinated heartbeat is a function of: 1. Presence of gap junctions 2. Intrinsic cardiac conduction system • Network of noncontractile (autorhythmic) cells • Initiate and distribute impulses to coordinate depolarization and contraction of heart https: //www. youtube. com/watch? v=SMXBR_YFocs

• Action potential initiation by pacemaker cells • Cardiac pacemaker cells have unstable resting membrane potentials called pacemaker potentials or prepotentials • Three parts of action potential 1. Pacemaker potential: K+ channels are closed, but slow Na+ channels are open, causing interior to become more positive 2. Depolarization: Ca 2+ channels open (around 40 m. V), allowing huge influx of Ca 2+, leading to rising phase of action potential 3. Repolarization: K+ channels open, allowing efflux of K+, and cell becomes more negative

Pacemaker potential This slow depolarization is due to both opening of Na+ channels and closing of K+ channels. Notice that the membrane potential is never a flat line.

Depolarization The action potential begins when the pacemaker potential reaches threshold. Depolarization is due to Ca 2+ influx through Ca 2+ channels.

Repolarization is due to Ca 2+ channels inactivating and K+ channels opening. This allows K+ efflux, which brings the membrane potential back to its most negative voltage.
 node")
Intrinsic Conduction System of the Heart: Setting the Basic Rhythm • Sinoatrial (SA) node is the heart’s pacemaker • Atrioventricular (AV) node is at the junction of the atria and ventricles • Atrioventricular (AV) bundle (bundle of His) is in the interventricular septum • Bundle branches are in the interventricular septum • Purkinje fibers spread within the ventricle wall muscles https: //www. youtube. com/watch? v=RYZ 4 da. Fw. Ma 8
 node (pacemaker) Left atrium Atrioventricular (AV) node Right atrium")
Superior vena cava Sinoatrial (SA) node (pacemaker) Left atrium Atrioventricular (AV) node Right atrium Bundle branches Atrioventricular (AV) bundle (bundle of His) Purkinje fibers Interventricular septum

Heart Contractions • Intrinsic conduction system enforces 75 beats per minute • Contraction is initiated by the sinoatrial node (SA node) • Sequential stimulation occurs at other autorhythmic cells • Force cardiac muscle depolarization in one direction—from atria to ventricles

Heart Contractions • Once SA node starts the heartbeat • Impulse spreads to the AV node • Then the atria contract • At the AV node, the impulse passes through the AV bundle, bundle branches, and Purkinje fibers • Blood is ejected from the ventricles to the aorta and pulmonary trunk as the ventricles contract

Problem • Defects in intrinsic conduction system may cause: • Arrhythmias: irregular heart rhythms • Uncoordinated atrial and ventricular contractions • Fibrillation: rapid, irregular contractions • Heart becomes useless for pumping blood, causing circulation to cease; may result in brain death • Treatment: defibrillation interrupts chaotic twitching, giving heart “clean slate” to start regular, normal depolarizations https: //www. youtube. com/watch? v=8 A 0 klj. QU 48 U

Problem • Defective SA node may cause ectopic focus, an abnormal pacemaker that takes over pacing • If AV node takes over, it sets junctional rhythm at 40– 60 beats/min • Extrasystole (premature contraction): ectopic focus of small region of heart that triggers impulse before SA node can, causing delay in next impulse • Heart has longer time to fill, so next contraction is felt as thud as larger volume of blood is being pushed out • Can be from excessive caffeine or nicotine

Problem • To reach ventricles, impulse must pass through AV node • If AV node is defective, may cause a heart block • Few impulses (partial block) or no impulses (total block) reach ventricles • Ventricles beat at their own intrinsic rate • Too slow to maintain adequate circulation • Treatment: artificial pacemaker, which recouples atria and ventricles

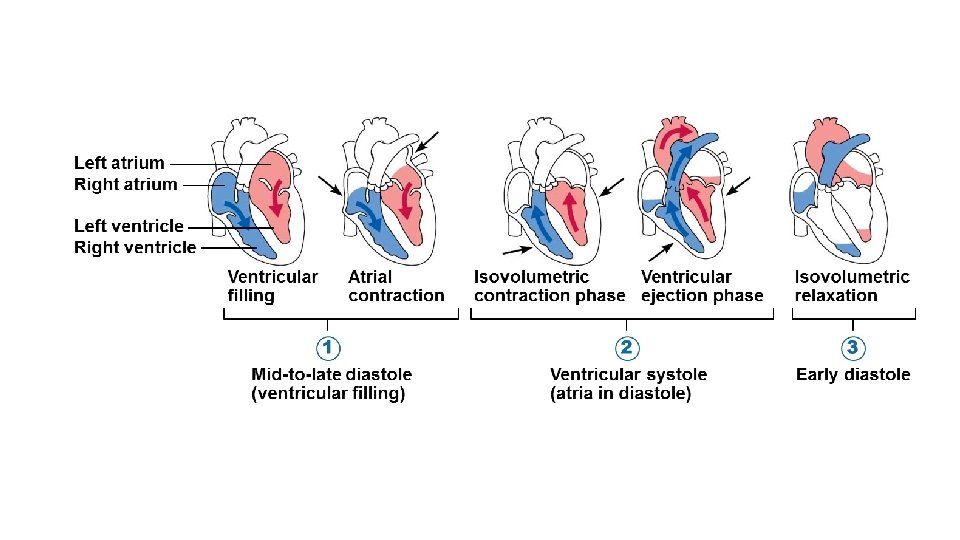
Cardiac Cycle & Heart Sounds • Cardiac cycle refers to one complete heartbeat • Systole contraction • Diastole relaxation • Heart beats approximately 75 times per minute • Cardiac cycle length is normally 0. 8 second
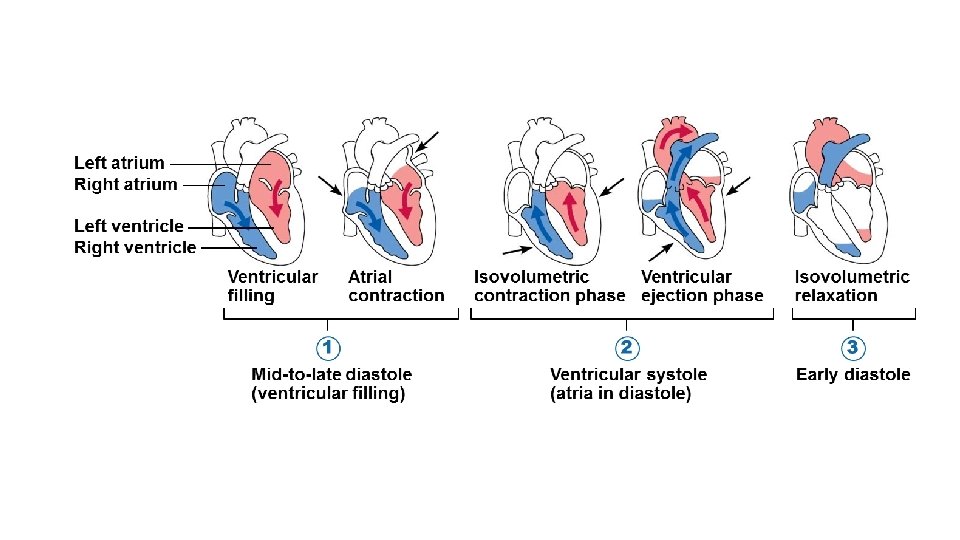

Cardiac Cycle & Heart Sounds • Mid-to-late diastole • • • Pressure in heart is low Blood flows passively into the atria and into ventricles Semilunar valves are closed Atrioventricular valves are open Atria contract and force blood into ventricles

Cardiac Cycle & Heart Sounds • Ventricular systole • • • Blood pressure rises as ventricles prepare to contract Atrioventricular valves close causing first heart sound, “lub” Semilunar valves open as blood pushes against them Blood travels out of the ventricles through pulmonary trunk and aorta Atria are relaxed and filling with blood

Cardiac Cycle & Heart Sounds • Early diastole • At the end of systole, all four valves are briefly closed at the same time • Second heart sound is heard as semilunar valves close, causing “dup” sound • Closure prevents blood backflow into ventricles • Atria finish refilling as pressure in heart drops • Ventricular pressure is low • Atrioventricular valves open

Another problem • Faulty valves reduce the efficiency of the heart as a pump and result in abnormal heart sounds (murmurs)
 • Amount of blood pumped by each side")
Cardiac Output • Cardiac output (CO) • Amount of blood pumped by each side (ventricle) of the heart in one minute • Stroke volume (SV) • Volume of blood pumped by each ventricle in one contraction (each heartbeat) • About 70 ml of blood is pumped out of the left ventricle with each heartbeat • Heart rate (HR) • Typically 75 beats per minute
 SV")
Cardiac Output • CO = HR SV • CO = HR (75 beats/min) SV (70 ml/beat) • CO = 5250 ml/min = 5. 25 L/min
 controls")
Regulation of Heart Rate • Heart rate is modified by: 1. Neural (ANS) controls • Sympathetic nervous system • Parasympathetic nervous system 2. Hormones and ions 3. Physical factors

Regulation of Heart Rate • If SV decreases as a result of decreased blood volume or weakened heart, CO can be maintained by increasing HR and contractility • Positive chronotropic factors increase heart rate • Negative chronotropic factors decrease heart rate • Heart rate can be regulated by: • Autonomic nervous system • Chemicals • Other factors

• Autonomic nervous system regulation of heart rate • Sympathetic nervous system can be activated by emotional or physical stressors • Norepinephrine is released and binds to 1 -adrenergic receptors on heart, causing: • Pacemaker to fire more rapidly, increasing HR • Increased contractility • Parasympathetic nervous system opposes sympathetic effects • Acetylcholine hyperpolarizes pacemaker cells by opening K+ channels, which slows HR • Has little to no effect on contractility

• Heart at rest exhibits vagal tone • Parasympathetic is dominant influence on heart rate • Decreases rate about 25 beats/min • Cutting vagal nerve leads to HR of 100

• Chemical regulation of heart rate • Hormones • Epinephrine from adrenal medulla increases heart rate and contractility • Thyroxine increases heart rate; enhances effects of norepinephrine and epinephrine • Ions • Intra- and extracellular ion concentrations (e. g. , Ca 2+ and K+) must be maintained for normal heart function • Imbalances are very dangerous to heart
 Low blood High blood")
Crisis stressors (physical or emotional trauma; increased body temperature; exercise) Low blood High blood pressure or blood volume Sympathetic nervous system activity Crisis has passed Increased venous return Decreased venous return Increased contractile force of cardiac muscle Heart rate (beats/min) KEY: Increases, stimulates Reduces, inhibits Initial stimulus Physiological response End result Decreased blood volume (hemorrhage) Activation of skeletal muscle and respiratory “pumps” Hormones: epinephrine, thyroxine Parasympathetic nervous system controls (via vagus nerves) Exercise Stroke volume (ml/beat) Cardiac output (ml/min)

Things to know: • Hypocalcemia: depresses heart • Hypercalcemia: increases HR and contractility • Hyperkalemia: alters electrical activity, which can lead to heart block and cardiac arrest • Hypokalemia: results in feeble heartbeat; arrhythmias

• Other factors that influence heart rate • Age • Fetus has fastest HR; declines with age • Gender • Females have faster HR than males • Exercise • Increases HR • Trained atheles can have slow HR • Body temperature • HR increases with increased body temperature
 • If persistent, may")
Problems: • Tachycardia: abnormally fast heart rate ( 100 beats/min) • If persistent, may lead to fibrillation • Bradycardia: heart rate slower than 60 beats/min • May result in grossly inadequate blood circulation in nonathletes • May be desirable result of endurance training
 • Progressive condition; CO is so low")
More problems • Congestive heart failure (CHF) • Progressive condition; CO is so low that blood circulation is inadequate to meet tissue needs • Reflects weakened myocardium caused by: • Coronary atherosclerosis: clogged arteries caused by fat buildup; impairs oxygen delivery to cardiac cells • Heart becomes hypoxic, contracts inefficiently • Persistent high blood pressure: aortic pressure 90 mm. Hg causes myocardium to exert more force • Chronic increased ESV causes myocardium hypertrophy and weakness • Multiple myocardial infarcts: heart becomes weak as contractile cells are replaced with scar tissue • Dilated cardiomyopathy (DCM): ventricles stretch and become flabby, and myocardium deteriorates • Drug toxicity or chronic inflammation may play a role https: //www. youtube. com/watch? v=afr. RNjs. Wn 9 s

• What congestive heart failure does: • Either side of heart can be affected: • Left-sided failure results in pulmonary congestion • Blood backs up in lungs • Right-sided failure results in peripheral congestion • Blood pools in body organs, causing edema • Failure of either side ultimately weakens other side • Leads to decompensated, seriously weakened heart • Treatment: removal of fluid, drugs to reduce afterload and increase contractility
- Slides: 54