Cardiac Arrest and Cardiopulmonary Resuscitation in Hospital Setting






 or ventricular tachycardia (VT)")



















 were developed in Australia and consist of doctors and nurses")

- Slides: 37
Cardiac Arrest and Cardiopulmonary Resuscitation in Hospital Setting By Prof. Ramadan Nafae Professor and Head of Chest Diseases Department Faculty of Medicine Zagazig University
History v. Before the introduction of open-chest cardiac massage and electrical reversal of ventricular fibrillation (VF), resuscitation was successful primarily in victims of respiratory arrest. v The combined procedures of positive-pressure ventilation, closedchest precordial compression, and electrical defibrillation were introduced into clinical practice in 1960 by a retired Johns Hopkins University Dean of Engineering, W. B. Kouwenhoven, who worked in collaboration with a surgical resident, J. R. Jude, and graduate student of biomedical engineering, G. G. Knickerbocker. This ushered in the modern era of CPR.
Pathogenesis of cardiac Cardiac arrest isarrest characterized by abrupt cessation of mechanical activity of the heart and loss of spontaneous and effective circulation. electrical mechanism of cardiac arrest Pulseless electrical activity and asystole (20%) VF/VT(80%)
Etiolog y
Diagnosis 1. Unexpected loss of consciousness in the unmonitored patient. 2. Loss of palpable central arterial pulse. 3. Respiratory arrest in a patient previously breathing spontaneously. Differential Diagnosis 1. Syncope or vasovagal reactions. 2. Coma. 3. “Collapse”. 4. Seizures.
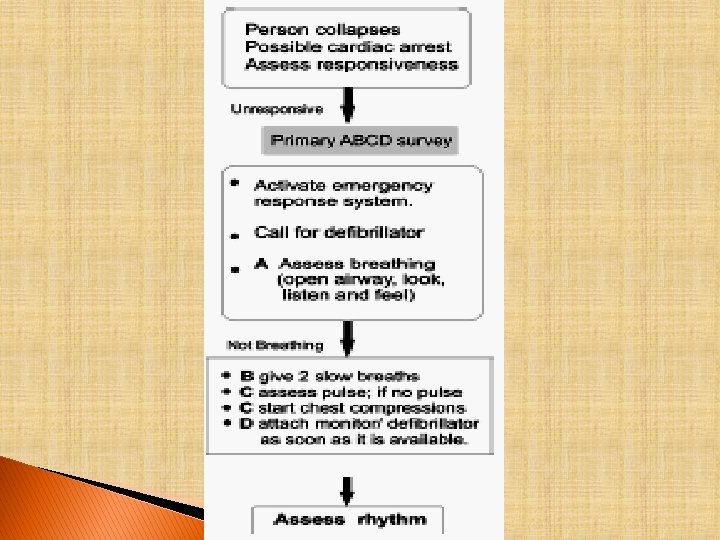
Management American Heart Association Chain of Survival
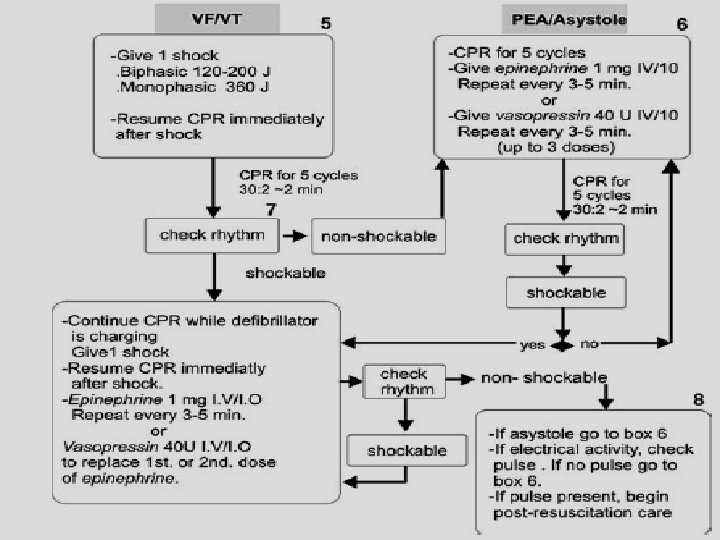
Initial management in the hospital setting If ventricular fibrillation (VF) or ventricular tachycardia (VT) is the first rhythm encountered, up to three DC shocks should be delivered as soon as possible, at energy settings of 200 J, 200 J and then 360 J. If the rhythm is other than VF, immediately proceed to the non. VF/VT protocol. If the rhythm cannot be identified immediately: Gain control of th airway, commence basic CPR and establish intravenous (IV) access while waiting for rhythm monitoring equipment to arrive.
Ventricular fibrillation Ventricular tachycardia
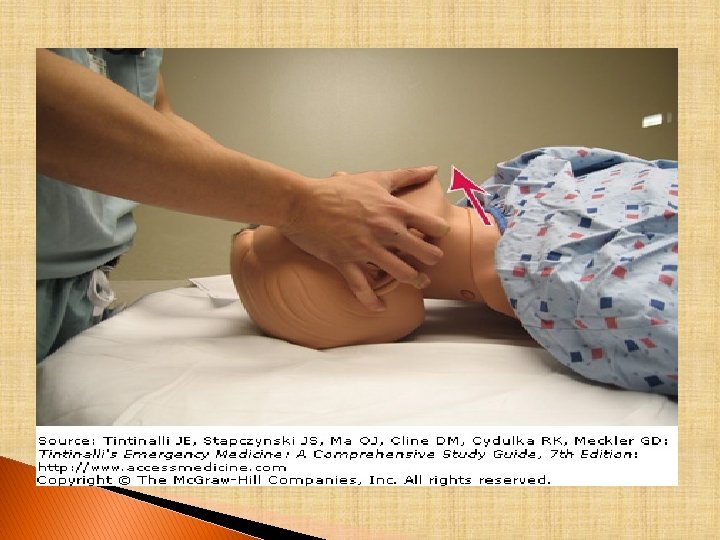
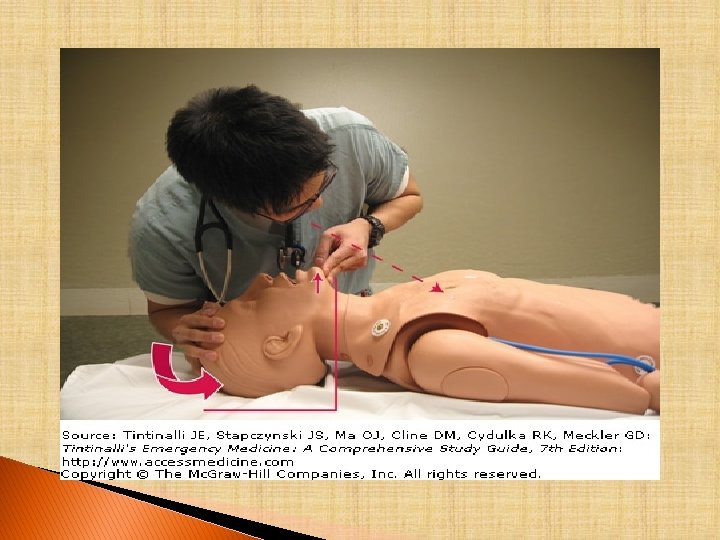
Technique of CPR Establish an effective airway ♦The three basic airway manoeuvres are head tilt, chin lift and jaw thrust. ♦The airway must be cleared of any foreign matter or obstruction with finger sweeps (community) or suction (hospital) and positioning. ♦Initially use mouth-to-mask or bag-and-mask ventilation. ♦Intubation with a tracheal tube will give better control of the airway. ♦If intubation is difficult, do not persevere – ensure adequate ventilation and oxygenation with a simpler technique such as a laryngeal mask.
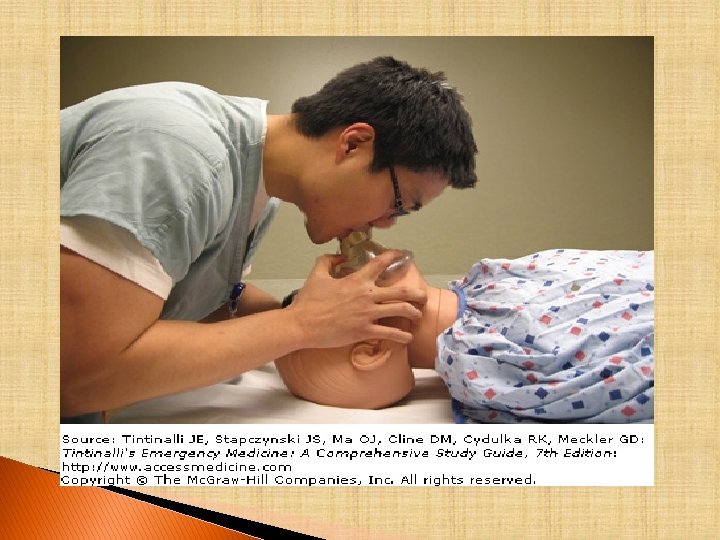
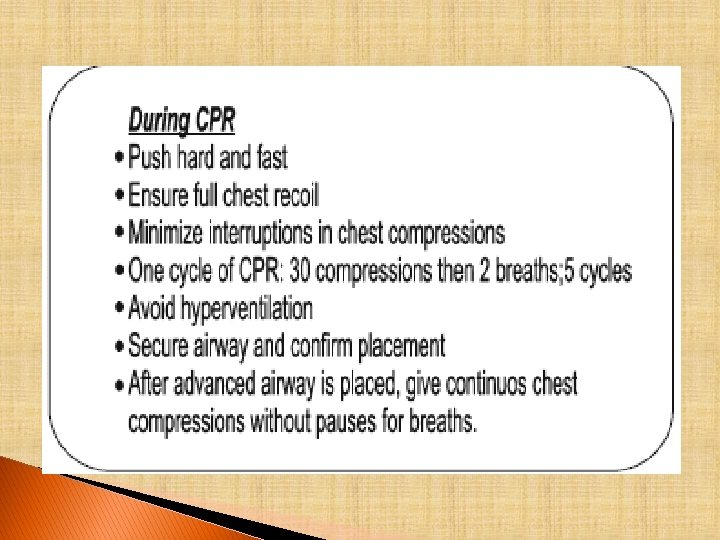
Ventilation Either via mouth mask or bag mask ventilation. Use the most high Fio 2 possible (100% O 2). Ventilations should be performed with a tidal volume of 5– 7 m. L/kg of ideal body weight. Single rescuer or two rescuer, nonintubated patient: give two breaths after every 30 compressions. Two rescuers, intubated patient: give breaths at a rate of 8– 10 breaths/min. Do not pause in chest compressions for ventilations.
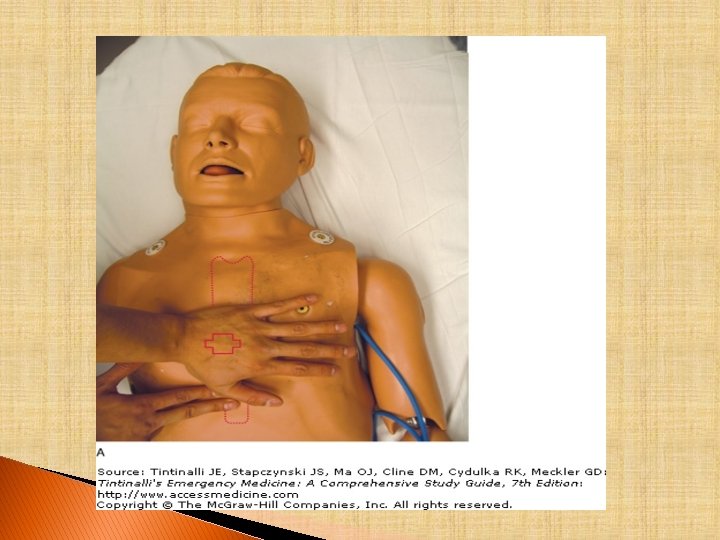
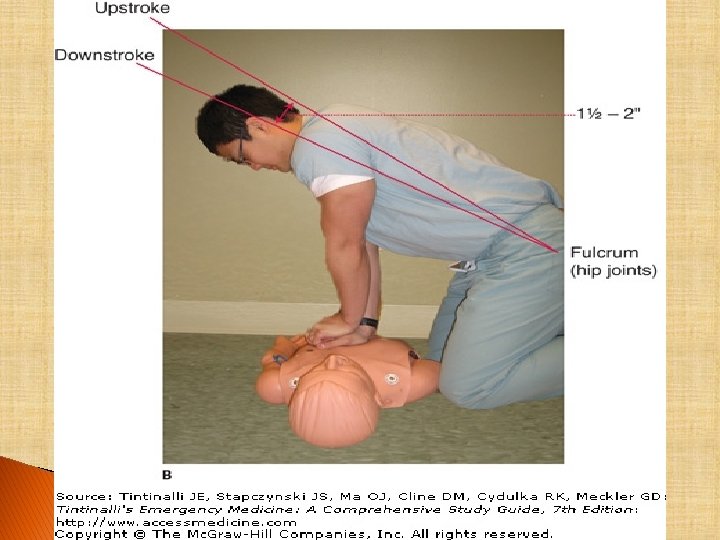
Circulation ♦Check for a carotid or femoral pulse. If there is no pulse or only a weak pulse and the blood pressure is too low to be measured, start external chest compression. ♦Rescuer’s hand located in the lower margin of sternum. ♦Heel of one hand is placed on the lower half of the sternum and the other hand is placed on top of the hand on the sternum so that the hands are parallel. ♦Elbows are locked in position, the arms are straightened, and the rescuer’s shoulders are positioned directly over the hands, providing a straight thrust. ♦The sternum is depressed 11/2– 2 in. in normal-sized adults with each compression at a rate of 100/min. .
Effective CPR, at best, will give a cardiac output that will be 25– 30% of normal, a systolic blood pressure (BP) of 60– 80 mm. Hg and a diastolic pressure of approximately 40 mm. Hg. Cardiac output will decline with time. After 15 minutes, it will be only 15% of normal. The ‘chest thump’ as an initial manoeuvre to convert VF may be used in monitored VF/pulseless VT arrests as it will occasionally result in conversion. However, the ‘chest thump’ should not delay the administration of DC shock.
Cardiac monitoring and dysrhythmia recognition: v. Defibrillation is the major determinant of survival in cardiac arrest due to VF or pulseless VT. v. Resume chest compressions after delivering one shock. Relationship between the interval before attempted defibrillation and hospital discharge after out-of-hospital cardiac arrest
Drug therapy during CPR may be given by the following routes: Peripheral vein (antecubital or external jugular are preferred). Central venous line (subclavian or internal jugular Intraosseous (IO) cannulation provides access that is safe and effective for drug delivery, fluid resuscitation, and blood sampling. Endotracheal: Medications should be administered at 2– 2. 5 times the recommended intravenous (IV) dose and should be diluted in 10 m. L of normal saline or distilled water, a catheter should be passed beyond the tip of the endotracheal tube, and the medication sprayed quickly followed by several quick insufflations.
Drug s Vasopressor Agents
Adrenaline q. Its alpha vasoconstrictor action diverts the blood flow, increasing the flow to vital organs and increasing coronary and cerebral perfusion pressures. q. Adverse effects include increased myocardial oxygen consumption (VO 2), subendocardial ischemia and arrhythmia. q. Adrenaline is still the first line drug for use in patients who have VF/VT unresponsive to defibrillation, a systole and pulseless electrical activity (PEA). q. It must be emphasized that adequate chest compression is critical if one is to gain the full beneficial effects of
Vasopressin qnaturally occurring antidiuretic hormone vasopressin is a vasoconstrictor at high doses via the. V 1 receptor. q. It is recommended by some to be used in VF/VT refractory to shock and adrenaline. q One dose only at 40 units. The half-life of vasopressin is 10– 70 minutes.
Sodium bicarbonate The indications for the use of sodium bicarbonate in CPR are few: qpre-existing metabolic acidosis. qhyperkalaemia. qoverdosage with tricyclic drugs. It may also be useful in prolonged CPR (e. g. more than 20 minutes). q. Give sodium bicarbonate (50 mmol) IV as a bolus dose and then use regular arterial blood gas determinations to guide further treatment
Calcium chloride q. Calcium is indicated for hyperkalaemia and hypocalcaemia and in cases in which it is suspected that there is toxicity due to calcium channel blocking drugs. q. Give calcium chloride (10%) 2– 4 mg/kg. Repeat after 10 minutes if necessary. Atropine q. Atropine may reverse extremes of bradycardia and even ventricular asystole after intense vagal stimulation, especially during anesthesia or surgical procedures. In these instances, 1 mg of atropine sulfate is injected intravenously and repeated in 3 to 5 minutes if bradyarrhythmia persists.
Amiodarone q. Amiodarone is useful in both supraventricular and ventricular arrhythmia, particularly in patients with impaired left ventricular function. q 150 mg IV over 10 minutes Otherthen an infusion of 1 mg/min inotropes for 6 hours. q. Combinations of other drugs, such as dobutamine, dopamine, noradrenaline and isoprenaline, may have a place in ‘fine-tuning’ cardiovascular function spontaneous circulation has been re-established. after
Defibrillation q. Defibrillation depolarizes the myocardium and allows the most rapid natural pacemaker, the sinoatrial node, to drive the heart’s rhythm. q. Immediate defibrillation is the treatment of choice for VF or Vt. q If VF or VT without an output is the first rhythm encountered, up to three sequential countershocks of 200 J, 200 J and then 360 J should be delivered, with no CPR in between. q. The defibrillator operator is responsible for determining that staff members are clear of the bed at the time of
Further management Check for and correct reversible 5 T’s: causes 5 H’s: Hypoxaemia Hypovolaemia Hypothermia Hydrogen ion – acidosis Hyper/hypokalaemia and metabolic disorders Tamponade Tension pneumothorax Toxins/poisons/drug s Thrombosis – coronary Thrombosis – pulmonary
q. Continue CPR: when conducting tests, procedures or reviewing an ECG, do not interrupt the CPR for more than a few seconds. q. A spontaneous palpable pulse is the best evidence that cardiac output has returned. Immediately resume CPR if the pulse is not detected. Brain resuscitation q. The most effective way to maintain cerebral function is to provide efficient CPR. q. Inducing hypothermia following successful resuscitation is currently being studied. Initial studies show improved neurologic outcome.
Poor Prognostic indicators after CPR q. The purpose of CPR is to prevent sudden, unexpected death, not to prolong meaningless life. q. Brainstem signs such as pupil size and reaction to light are unreliable indicators of neurological status during CPR.
Post-cardiopulmonary resuscitation q. It is important to correct as many ‘correctables’ as possible. q. Obtain a post-resuscitation chest x-ray to exclude pulmonary barotrauma, aspiration pneumonia, gastric dilatation and check the position of the ETT and invasive monitoring devices in the thorax (e. g. temporary pacemakers, central venous catheters). q. Regarding neurological damage, most studies have shown that if there is to be full neurological recovery, it will occur within the first 48 hours after cardiac arrest, Otherwise there will be varying degrees of permanent damage resulting from the global ischaemia at the time of arrest.
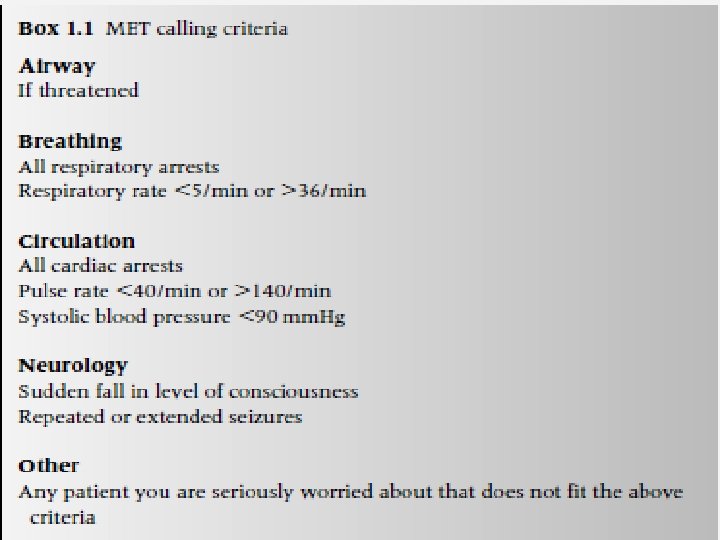
Prevention of cardiopulmonary q. Because of the increased monitoring and awareness arrests in ICUs, it probably is no coincidence that patients in intensive care rarely experience unexpected cardiorespiratory arrest. q. It is therefore important that the entire staff of a hospital become better educated in how to recognise patients who are rapidly deteriorating. q. There is some evidence that the cardiac arrest team would be more successful being rapidly deployed to patients who were at high risk of having an arrest, rather than to those who had actually arrested.
Medical emergency teams (METs) were developed in Australia and consist of doctors and nurses trained in advanced resuscitation skills. The idea is that seriously abnormal vital signs trigger an emergency call, rather than waiting for cardiopulmonary arrest.