CARCINOMA OF RECTUM Carcinoma Rectum Colorectal ca 3










, localised liver")



- Slides: 19
CARCINOMA OF RECTUM
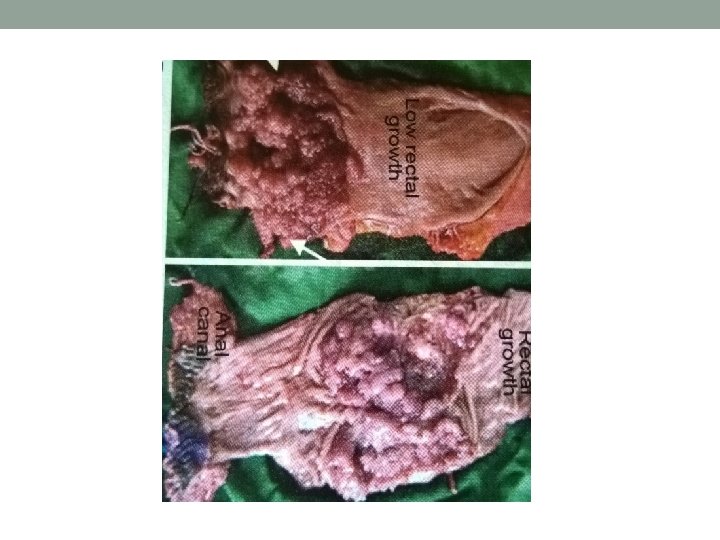
Carcinoma Rectum • Colorectal ca 3 rd commonest in men and 4 th commonest among women • Pathology- normal epi> adenoma with mild dysplasia> intermediate> severe> ca in situ> invasive ca • Well, moderately, poorly differentiated or anaplastic ca • Ulcerative/ proliferative • Columnar cell, colloid ca
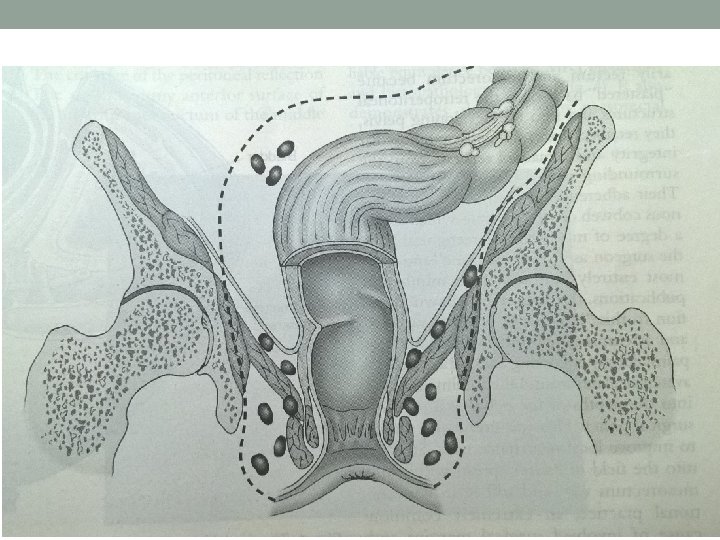
Spread • Local- circumferential: 6 months for ¼ circumference. Deeper: mesorectum, ureters, prostate, seminal vesicles, bladder, vagina, uterus, sacrum, sacral plexus • lymphatic- upto 1 -2 cm from anal verge, upwards to pararectal LN of Gerota. Atypical- widespread lymphatic permeation in Anaplastic ca
• Venous- late. Liver, lung, adrenals, brain • Peritoneal- upper rectal growth
• Normal colonic mucosa>dysplastic aberrant crypt foci>early adenoma>intermediate adenoma>late adenoma>ca in situ>invasive ca • Tumour suppressor genes- APC gene, p 53 gene, STK 11 gene. • Mismatch Repair Gene, microsatellite instability. • Oncogenes- k ras.
Etiology • Diet- red meat, saturated fatty acid. • Alcohol and smoking • FAP, HNPCC, Adenoma. • Ulcerative colitis, Crohn’s disease. • Family history of rectal carcinoma.
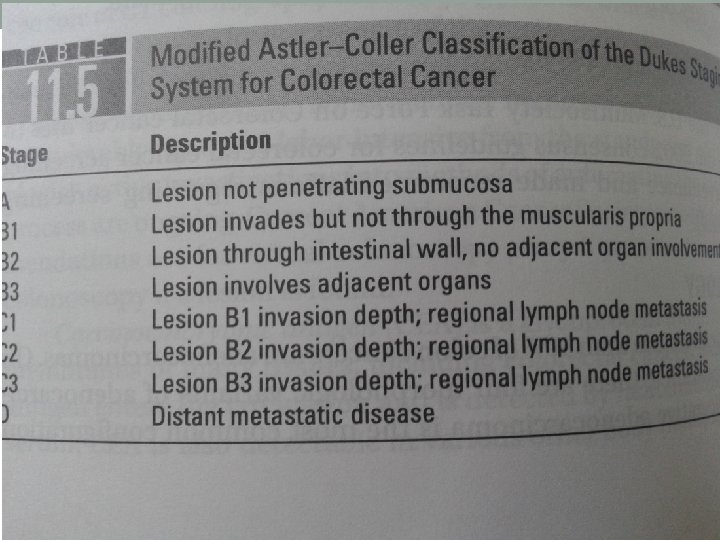
Staging • Dukes: A- tumour confined to bowel wall B- spread beyond serosa to adjacent structures, no nodes C- Lymph nodes involved • TNM: Tx- primary cannot be assessed, T 0 - no evidence of primary, T 1 - tumour invades upto submucosa, T 2 - tumour upto muscularis propria, T 3 - invades upto subserosa or upto pericolic or pararectal tissue at unperitonealised area, T 4 invasion of adjacent organ or perforation
• N 0 - no regional nodes, N 1 - 1 to 3 nodes, N 2 - metastasis to 4 or more regional nodes • M 0 , M 1
Clinical Features • Usually > 55 years, rarely in younger- FAP • Bleeding – fresh • Tenesmus, spurious diarrhoea, bloody slime • Altered bowel habits, weight loss • Pain- colicky, due to obstruction, continuous due to deeper invasion • Intestinal obstruction, palpable liver, ascites • Rectal digital examination- 90% palpable
Investigations • Sigmoidoscopy, colonoscopy • Biopsy • Ba enema • USG, TRUS • CT abdomen • MRI
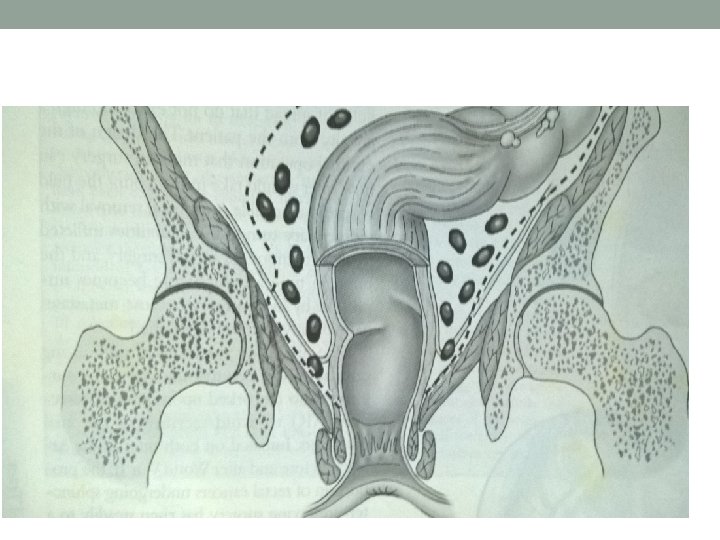
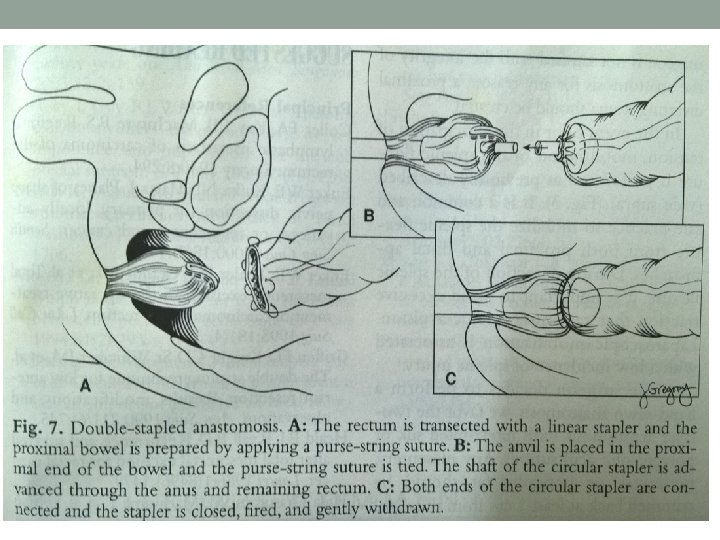
Treatment- Surgical • Principle- radical excision of rectum with mesorectum, involved LN(TME), localised liver metastasis if any. If advanced- palliative resection/ colostomy • Surgeries- Anterior resection, Abdominoperitoneal resection with colostomy, Transanal resection, Colostomy. • Open or laparoscopic approach, robotic surgery
Anterior Resection
Abdomino-perineal Resection
• Radiotherapy- Pre op if locally advanced. Post op. Palliative if inoperable/ painful local recurrence • Chemotherapy-Folinic acid, 5 FU, Oxaliplatin(FOLFOX) or Folinic acid, 5 FU, Irinotecan(FOLFIRI). Capecitabine • Monoclonal antibodies- Bevacizumab, cetuximab.