CARCINOMA OESOPHAGUS BENIGN TUMORS AND CYSTS i Leiomyoma

CARCINOMA OESOPHAGUS

BENIGN TUMORS AND CYSTS i. Leiomyoma ii. Cyst iii. Polyp iv. Papilloma v. Lipoma vi. Haemangioma vii. Adenoma viii. Granular cell myoblastoma

AETIOLOGY i. 45 – 75 yrs, M>F ii. Alcohol and tobacco iii. Malnutrition, vitamin deficiency, anaemia, poor oral hygiene iv. Plummer Vinson Syndrome v. Achalasia

PREMALIGNANT CONDITIONS i. iii. iv. v. Hiatus hernia and GERD Barrett’s oesophagus Irradiation oesophagitis Corrosive oesophagitis from Lye Oesophageal diverticulum
 • Histologically >95% are squamous cell carcinomas")
PATHOLOGY • Highest incidence- Lower 1/3 (>50%) • Histologically >95% are squamous cell carcinomas • Adenocarcinomas (<5%) develop from – The junctional columnar epithelium from the distal oesophsgus – Barrett’s mucosa – Glanduar epithelium – Ectopic gastric mucosa

SPREAD i. Local infiltraton – longitudinal and circumferential stricture formation ii. Lymphatic spread – to regional LN, as well as by submucous lymphatic permiation and embolism resulting in satellite lesions well beyond the apparent margin of the growth iii. Haematogenous spread – rare and usually late – liver, lungs, brain, bones

CLINICAL FEATURES • Non-specific symptoms – Retrosternal discomfort – Indigestion – Weight loss – Occult mild anaemia • Progressive dysphagia – Insidious onset – Solids > liquids

Clinical findings suggestive of advanced malignancy include – Recurrent laryngeal nerve palsy, – Horner’s syndrome, – Chronic spinal pain and – Diaphragmatic paralysis

INVESTIGATIONS • Barium oesophagogram – Irrgular mucosal filling defect – Distortion of the oesophageal lumen – Annular stricture – Rat-tail filling defects • Oesopagoscopy – 1 st line of diagnosis • Broncoscoy • CT

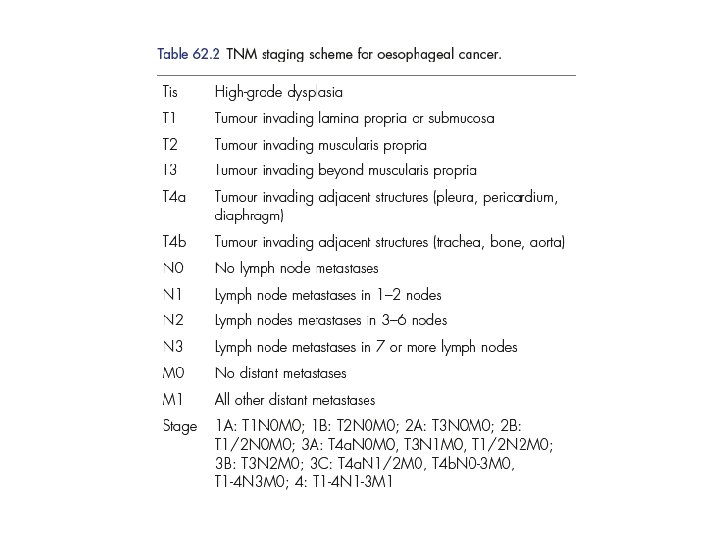
• Endoscopic ultrasound – the depth of spread of a malignant tumour through the oesophageal wall (T 1– 3), – the invasion of adjacent organs (T 4) and – metastasis to lymph nodes (N 0 or N 1) – It can also detect contiguous spread downward into the cardia and more distant metastases to the left lobe of the liver. • PET Scan (18 FDG)

Barium study

Oesophagoscopy

Bronchoscopy

TREATMENT PRINCIPALS: • At the time of diagnosis, around two-thirds patients will already have incurable disease. • The aim of palliative treatment is to overcome debilitating or distressing symptoms while maintaining the best quality of life possible for the patient. • As dysphagia is the most common symptom the principal aim of palliation is to restore adequate swallowing.

• The principle of oesophagectomy is to deal adequately with the local tumour in order to minimise the risk of local recurrence and achieve an adequate lymphadenectomy to reduce the risk of staging error. • A number of studies support the view that the proximal extent of resection should ideally be 10 cm above the macroscopic tumour and 5 cm distal.

• If nodes are present, then multimodal approach should be used like—curative resection; radiotherapy and chemotherapy. • Outcome of surgery depends on location of tumour; number, location and size of nodes; tumour grading. • Surgery alone is best suited to patients with disease confined to the oesophagus (T 1, T 2) without nodal metastasis (N 0).
: • Treated")
APPROACH TO TUMOUR AT VARIOUS LEVELS Post cricoid tumour (Squamous cell carcinoma): • Treated mainly by radiotherapy. • Often pharyngolaryngectomy is done along with gastric or colonic transposition. But complications are more in this procedure. Free jejunal transfer is the other option.
: • Treated mainly by radiotherapy. • Mc. Keown")
Upper third growth (Squamous cell carcinoma): • Treated mainly by radiotherapy. • Mc. Keown three phased oesophagectomy Initially laparotomy is done to mobilise the stomach. Then thoracotomy through right 5 th space is done and oesophagus is mobilised. Through right side neck approach, oesophagus with growth is removed. Anastomosis between pharynx and stomach is done in the neck.

Thoracoscopic resection for esophageal cancer: A review of literature Miguel A Cuesta, Joris JG Scheepers, Donald L van der Peet, Alexander AFA Veenhof Journal of Minimal Access Surgery, Vol. 3, No. 4, October-December, 2007, pp. 149 -160
: • Ivor Lewis operation (Lewis-Tanner two-phased oesophagectomy): After")
Middle third growth (Squamous cell carcinoma): • Ivor Lewis operation (Lewis-Tanner two-phased oesophagectomy): After laparotomy stomach is mobilised. Pyloroplasty is done. Through right 5 th space thoracotomy is done and growth with tumour is mobilised. Partial oesophagectomy and oesophagogastric anastomosis is done in the thorax. • If the growth is inoperable, palliative radiotherapy is given.
: • Here through left thoracoabdominal approach,")
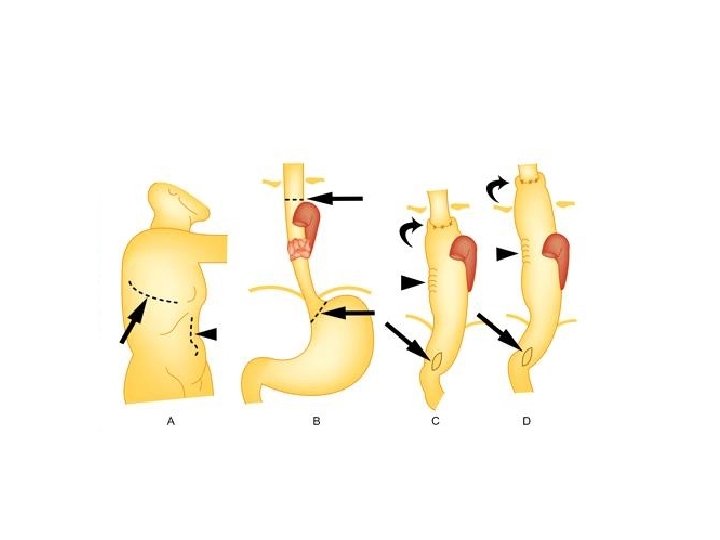
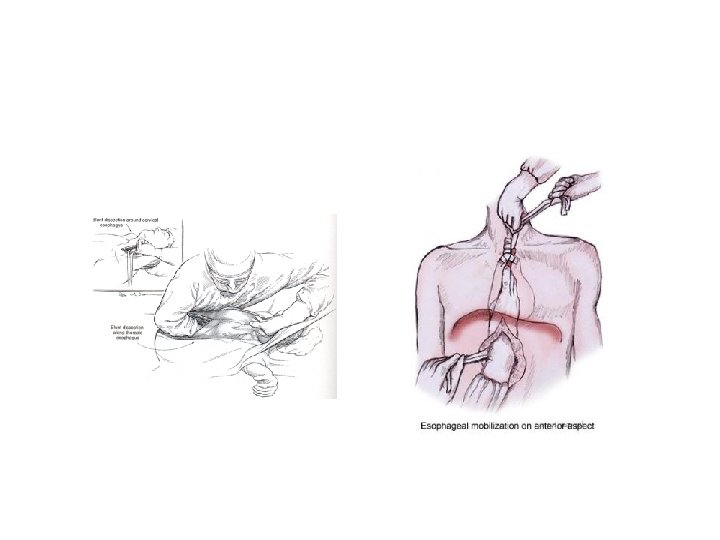
Lower third growth (Squamous cell carcinoma + adenocarcinoma): • Here through left thoracoabdominal approach, partial oesophagogastrectomy is done with oesophagogastric anastomosis. • Orringer approach, i. e. transhiatal blind total oesophagectomy with anastomosis in the left side of the neck. Through laparotomy, stomach and lower part of the oesophagus are mobilised. Through left sided neck approach, upper part of the oesophagus is mobilised using finger. Blind dissection is completed by meeting both fingers above and below in the thorax. Later oesophagus is pulled up out above through the neck wound and removed. Continuity is maintained in the neck. It is a palliative surgery.

Oesophageal substitutes: • Stomach • Colon • Jejunum • Transposition is done through posterior mediastinum (shortest route), right pleural space (transpleural), retrosternal or subcutaneous route.

PALLIATIVE TREATMENT • It is to relieve pain, dysphagia and to prevent aspiration and bleeding. • Palliation therapy is done – – – If patient is not fit for major surgery. If there is blood spread. If there is adjacent organ spread. If there is peritoneal/liver spread.

Palliative external radiotherapy • 3000 Rads. Severe mucositis, stricture and fistula formation are the complications. Intraluminal RT • Brachytherapy (radiation intraluminally). Loading catheter is placed using endoscope and applicator is fixed to mouth to give 1500 c. Gy radiation with least systemic effects.

Chemotherapy • Cisplatin; methotrexate; 5 FU; palcitaxel, etoposide, bleomycin. Intubation • Used for tracheo-oesophageal fistula or external compression. • Tubes used – Atkinson, Celestin, Souttar, Mousseau-Barbin tube
 – uncovered / plastic covered • Endoscopic laser")
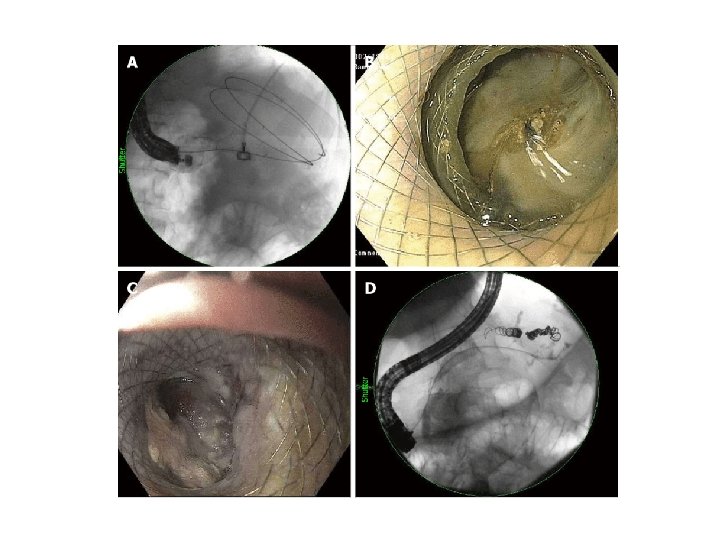
ENDOSCOPY: • Self-expanding metal stents (SEMS) – uncovered / plastic covered • Endoscopic laser • Endoscopic diathermy • Endoscopic photodynamic therapy

Surgery • Transhiatal Orringer’s blind oesophagectomy is a palliative surgical procedure. • Kirschner palliative gastric bypass done in advanced carcinoma oesophagus wherein mobilised stomach is brought to neck via retrosternal or subcutaneous route and anastomosed to divided cervical oesophagus. Lower cut end of oesophagus is anastomosed to a jejunal loop. Here oesophagus is not addressed (left alone).

PROGRESSION • • • Cancer cachexia Sepsis, mediastinitis Immunosuppression Malignant tracheo-oesophageal fistula Erosion into major blood vessel—bleeding
- Slides: 32