Cancer Risk Assessment for Personalized Screening and Prevention
















 Recommendation Routine screening mammogram in 1 year. Cancer")






 Recommendation Routine screening mammogram in 1 year. Cancer")



 Recommendation Routine screening mammogram in 1 year. Cancer")



- Slides: 34
Cancer Risk Assessment for Personalized Screening and Prevention of Cancer Caroline Peterson, D. O. FACOOG Director, Cancer Screening and Prevention for Kettering Health Network
Innovation and Collaboration Results • • • Centered Concept • • • Population Health Innovation/Technology Evidence Based Medicine • • Patient Medical Home Best Practice Preventative Care Quality Measures Best Outcomes Cost Savings Revenue Enhancement
Incorporating Hereditary Cancer Risk Assessment Into Your Practice
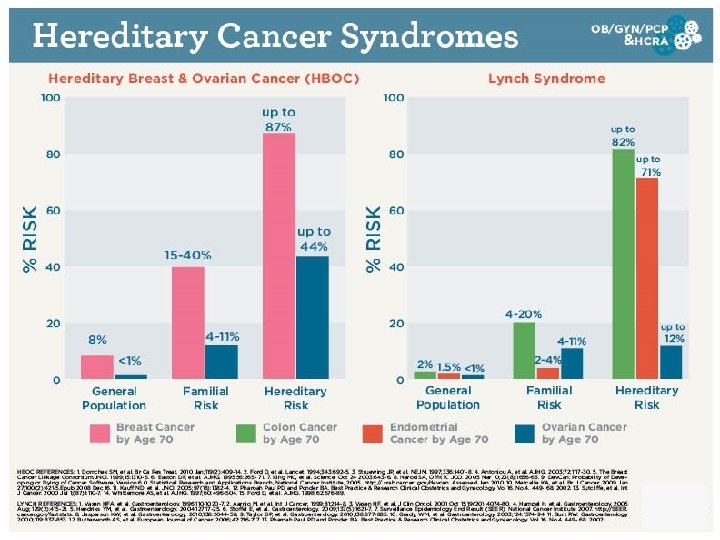
Summary: Currently known genetic markers for Breast Cancer ER- Br. Ca Pre-Menopausal ER+ Br. Ca Post-Menopausal
Precision Medicine
Risk Stratification
Moving Forward Together
Information Challenges Confusion Implementat ion
The Ambry C. A. R. E. Process Analyse Recommendations Customized Efficiency Lake Health Systems – Recommended Ambry C. A. R. E. Workflow Progeny Screening & Risk Model Assessment Begin, and Progeny Risk Assessment Report is Generated Patient Meets Testing Criteria No Patient Notified w/ Avg Risk Pamphlet – Schedule next Screen 1 Yr out Notify Patient that they are considered High Risk – Provide High Risk Pamphlet Yes Patient Reviews Pre. Test Education Video Schedule Patient at CPC or GYN Clinic CPP Collects GT Sample / Submits to Ambry via Progeny/Ambry Port GT Order GT Results Reported within Progeny
Gynecological and Medical History
Surgical and Family History
Pedigree
Cancer Risk Assessment Calculation The clinician will click the “Calculate” button and all risk factors are sent to the CRA Health cancer risk calculator. Within 15 seconds, all CRA Health risk models send the cancer risk scores back to the patients Epic medical record discretely. Results will be available in the risk screening navigator and in the patients chart.
Cancer Risk Recommendations in Epic
Cancer Risk Results and Statements in Epic
Mammo Screening ASSESSMENT : Negative (1) Recommendation Routine screening mammogram in 1 year. Cancer Risk Assessment was performed. Analysis reveals the following: 5 -year breast cancer risk: 3. 3% Lifetime breast cancer risk: 12. 9% HNPCC Mutation risk (Lynch Syndrome) : 0. 1% HBOCRisk: Elevated Risk Calculation Thresholds: >=20% LIFETIME BREAST, CONSIDER GENETIC TESTING AND BREAST MRI. >5% HNPCC Mutation risk (Lynch Syndrome), CONSIDER GENETIC TESTING. Elevated HBOC Risk, CONSIDER GENETIC TESTING.
Case Example #1 CHEK 2 positive result Cancer Family History Information • Patient: breast ca (lobular) @ 50 • Mother: breast ca @ 46 • Maternal Grandmother: breast ca @ 56 Patient Information • 57 year old female • DN, 3/25/1959 • Medicare Replacement • $0 out of pocket
Case Example #2 PMS 2 positive result Cancer Family History Information • Patient: NO CANCER DIAGNOSIS • Maternal Aunt: breast ca @ 50 • Maternal Grandmother: breast ca @ 67 • Paternal Uncle: CRC @ 62 • Paternal Cousin: CRC @ 35 Patient Information • 31 year old female • NS, 6/9/1985 • Key Benefit Adminstrators • $0 out of pocket
Pedigree
Moving Forward Together
Case Example #3 HIGH RISK NEGATIVE result Cancer Family History Information • Patient: NO CANCER DIAGNOSIS • Mother: breast ca @ 45 • Maternal Grandmother: breast ca @ 65 Patient Information • 48 year old female • DEH, 9/19/1969 • Medical Mutual of OH • $0 out of pocket
Risk Mutation & Risk Breast Ca Claus Chemoprevention MRI Personalized screening Gail Chemoprevention Personalized screening Hereditary BRCAPRO Genetic Testing Chemoprevention MRI Personalized screening Hormonal Tyrer Cuzick Pathologic Genetic Testing Chemoprevention MRI Personalized screening
Mammo Screening ASSESSMENT : Negative (1) Recommendation Routine screening mammogram in 1 year. Cancer Risk Assessment was performed. Analysis reveals the following: 5 -year breast cancer risk: 3. 3% Lifetime breastcancerrisk: 23% HNPCC Mutation risk (Lynch Syndrome) : 0. 1% HBOC Risk: Elevated Risk Calculation Thresholds: >=20% BREAST, CONSIDER GENETIC TESTING AND BREAST >=20%LIFETIME BREAST, CONSIDER GENETIC TESTING ANDMRI. BREAST MRI. >5% HNPCC Mutation risk (Lynch Syndrome), CONSIDER GENETIC TESTING. Elevated HBOC Risk, CONSIDER GENETIC TESTING.
Workflow-integrated Clinical Decision Support • Patient-entered family history and risk factors via Tablet or website • Risk calculations using standard models Recommendations >20% risk of breast cancer (Tyrer Cuzick, BRCAPRO, Claus) • Elevated-Risk Patients Receive appropriate MBI/MRI Screening 26 Gamma Medica, Inc. - Confidential
Breast Cancer Develops Before it’s Detected
Chemoprevention v Risk Reducing Medications SERMS : Selective Estrogen Regulating Modulators • Tamoxifen – Nalvadex, Soltamox • Raloxifene – Evista • Ospemifene – Osphena • Bazedoxifene + Conjugated Estrogen - Duavee
Mammo Screening ASSESSMENT : Negative (1) Recommendation Routine screening mammogram in 1 year. Cancer Risk Assessment was performed. Analysis reveals the following: 5 -yearbreastcancerrisk: 3. 3% 5 -year Lifetime breast cancer risk: 23% HNPCC Mutation : 5. 6% HNPCC Mutationrisk(Lynch. Syndrome) : 5. 6% HBOC Risk: Elevated Risk Calculation Thresholds: >=20% LIFETIME BREAST, CONSIDER GENETIC TESTING AND BREAST MRI. >5%HNPCCMutation risk GENETIC TESTING. >5% risk (Lynch. Syndrome), CONSIDER GENETIC TESTING. Elevated. HBOC Risk, CONSIDER GENETIC Elevated GENETICTESTING.
Multiple cancers can be associated with a single gene. If you are using a narrower testing approach, you may miss critical information, which may compromise patient outcomes. A single gene can be associated with multiple cancers.
Overall Objective Point A: Screening Sites Imaging, OB, GI, PCP Point B: Cancer Prevention Center
Preventive Care Navigation Surgery: Prophylactic Surgeries Breast MRI: Annual $ 5, 4, 97, 800 Colonoscopy: More Frequent A Preventative Care: Ongoing management