Cancer Education Day Lung Cancer Screening Update Kirenza












- Slides: 13
Cancer Education Day Lung Cancer Screening Update Kirenza Francis, MD, FRCPC, DABR Windsor Radiological Associates May 13, 2016
NO DISCLOSURES
Recent Changes in Recommendations due to National Lung Screening Trial • 2002 -2010 • 53, 454 participants • Participants: 55 -74 yo, 30 pack year smoking history current or former smokers • Low Dose Chest CT versus Chest X-ray for 3 years • Followed for and average for an average of 6. 5 years
NATIONAL LUNG CANCER SCREENING RESULTS • Low-dose helical CT scans had a 20 percent lower risk of dying from lung cancer than participants who received standard chest Xrays • 3 fewer deaths per 1, 000 people screened in the CT group compared to the chest X-ray group over a period of about 7 years of observation (17. 6 per 1, 000 versus 20. 7 per 1, 000, respectively
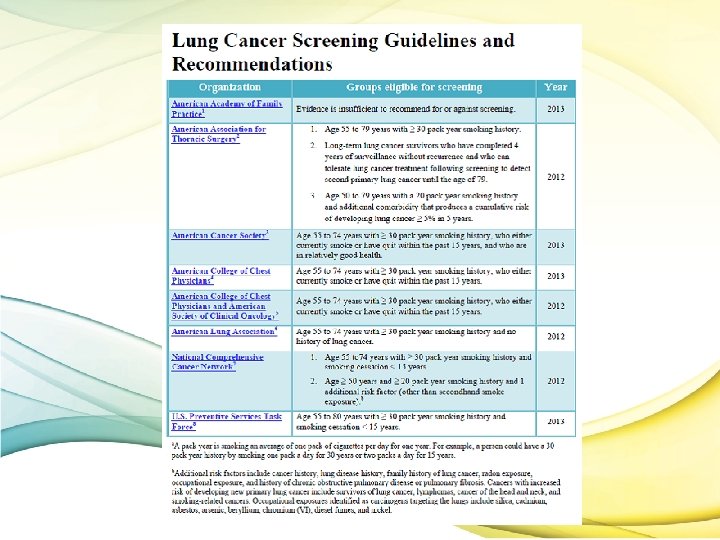
US PREVENTATIVE SERVICES TASK FORCE 2013 • The USPSTF recommends annual screening for lung cancer with low-dose computed tomography (LDCT) in adults aged 55 to 80 years who have a 30 pack-year smoking history and currently smoke or have quit within the past 15 years. Screening should be discontinued once a person has not smoked for 15 years or develops a health problem that substantially limits life expectancy or the ability or willingness to have curative lung surgery.
CANDADIAN TASK FORCE ON PREVENTATIVE HEALTH CARE 2016 • For adults aged 55– 74 years with at least a 30 pack-year smoking history who currently smoke or quit less than 15 years ago, we recommend annual screening with low-dose computed tomography (LDCT) up to three consecutive times. Weak recommendation • It is possible that longer or more intensive screening might yield additional benefits, but there is not strong evidence (from an RCT) to support such a recommendation.
Canadian Task Force on Preventative Health Care
AMERICAN COLLEGE OF RADIOLOGISTS SOCIETY OF THORACIC RADIOLOGIST PRACTICE PARAMETERS • “Maximum intensity projection (MIP) reconstruction is a technique that may be useful to increase the sensitivity for lung nodule detection. ”
LUNG CANCER SCREENING CONSIDERATIOINS • • • Pros Reduction in cancer death Earlier Stage Detection Safe, Noninvasive Discovery of ancillary findings (NLST All cause mortality was not different if lung cancer deaths excluded) • Cons • Cost • High False Positive – (When the NLST screening test was positive 96. 4% of the LDCT and 94. 5% of CXR exams were falsepositive, • Patient Anxiety • Incidental Findings • Radiation Risk
RADIATION RISK MEASUREMENT • An estimate of the uniform, whole-body equivalent dose that would produce the same level of risk for adverse effects that results from the non-uniform partial body irradiation. The unit for the effective dose is also the sievert (Sv)
RADIATION RISK –COMMON DOSES • CT Low Dose Chest for Lung Cancer Screening • Lumbar Spine X-rays • Normal Background Radiation – Toronto – Winnipeg • Yearly Exposure Domestic Airline Crew • Routine CT Chest • CT Abdomen and Pelvis • Occupational Radiation Limits 1 -1. 5 m. Sv 2 -3 m. Sv/yr 1. 6 m. Sv/yr 4. 1 m. Sv/yr 3 m. Sv/yr 7 m. Sv 10 m. Sv 50 m. Sv/yr
THANK YOU