Can we rely on imaging and biomarkers for

Can we rely on imaging and biomarkers for preemptive antifungal therapy in hematological patients? Claudio Viscoli Professor of Infectious Disease, University of Genova Chief, Division of Infectious Disease, San Martino University Hospital, Genova, Italy

A comprehensive approach to the diagnosis of IFI Host Laboratory Diagnosis Imaging Clinical aspects

Underlying disease in invasive aspergillosis 595 patients Patterson et al, Medicine, 2000

Underlying disease phase and primary site of infections n° 391 patients Pagano et al, Haematologica 2001

CHARACTERISTIC PATTERNS OF INVASIVE ASPERGILLOSIS IN COMMONLY AFFECTED PATIENT GROUPS UNDERLYING CONDITION TIMING OF INVASIVE ASPERGILLOSIS Acute Leukemia; Multiple Mieloma, stage II/III; Chronic leukemia in blast crisis; aplastic anemia; autologous bone marrow or PSC transplantation During induction chemotherapy (75%); During maintenance or consolidation treatments (25%). Maily related to neutropenia Allogeneic bone marrow or PSC transplantation, especially if matched unrelated or mismatched donor Early during neutropenia (20 -30%); Late (median 100 days) (75%), mainly related to severe GVHD and high-dose steroids

• 8988 admissions • 71 positive cultures for Aspergillus • Incidence rate 0. 4% (37 proven/probable diseases as from EORTC-MSG criteria)

A comprehensive approach to the diagnosis of IFI Host Laboratory Diagnosis Imaging Clinical aspects
 Thoracic pain (76%) Hemoptysis (54%) Fever Neurological signs")
Aspergillosis syndrome • • Cough (92%) Thoracic pain (76%) Hemoptysis (54%) Fever Neurological signs Nasal bleeding Nasal discharge Skin lesions
 §Cough")
CLINICAL SYMPTOMS IN 45 CASES OF IA IN HSCT PATIENTS §Fever 34/45 (75%) §Cough 12/45 (27%), §Dyspnoea 12/45 (27%) §Chest pain 9/45 (20%). §No sign or symptom 3 (positive GM with multiple pulmonary nodules on CT scan). § Radiological pulmonary lesions were mainly represented by nodules (8/42, 19%), cavitations (10/42, 24%) and wedge-shaped consolidations (4/42, 10%). §Notably, the halo sign was never found. Mikulska et al, BMT 2009

A comprehensive approach to the diagnosis of IFI Host Laboratory Diagnosis Imaging Clinical aspects
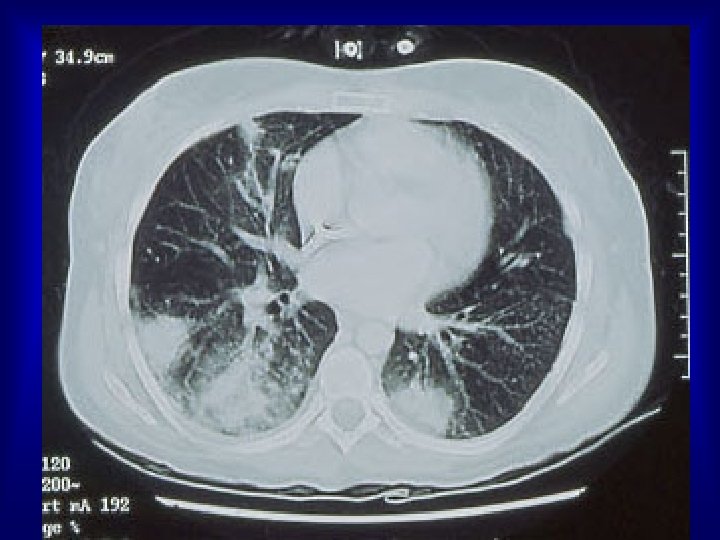
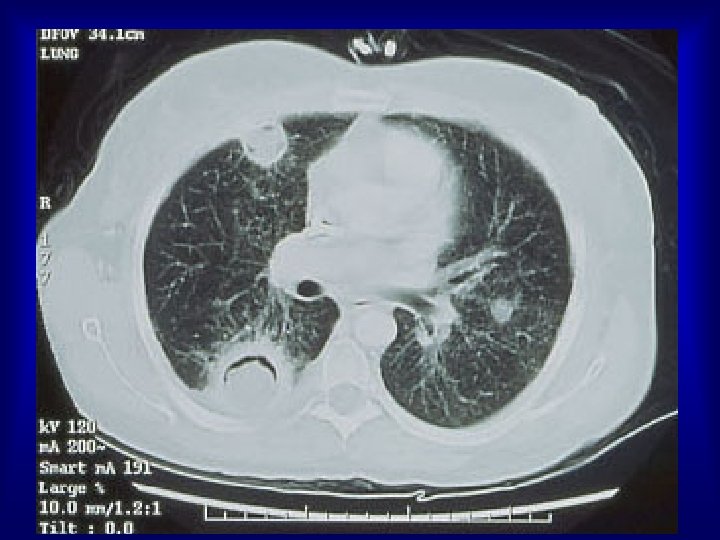

Invasive pulmonary aspergillosis IPA Normal lung IPA occurs in ~7% of acute leukaemia patients, 10 -15% allogeneic BMT patients www. aspergillus. man. ac. uk

Unequivocal ‘Halo sign’ surrounding a nodule Halo sign Herbrecht, Denning et al, NEJM 2002; 347: 408 -15.

CT scan evolution during IPA Peripheral halo triangolar shape Air-crescent sign d 0 - d 5 High value d 5 - d 10 not specific Neutropenia d 10 - d 20 delayed PMN >> 500 Caillot et al. J Clin Oncol. 2001; 19: 253 -9.

Early use of high-resolution CT scan for the diagnosis of pulmonary aspergillosis • Allows significantly earlier diagnosis and therapy (5 -10 days) • Associated with overall improved survival • Allows early surgical resection Caillot et al, JCO, 1997 Heussel et al, JCO, 1999

Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery (CAILLOT et al. J Clin Oncol 1997) S U R V I V A L systematic CT-scan on indication 0 50 100 150 200 days RETROSPECTIVE ANALYSIS n = 37 SYSTEMATIC CT-SCAN BEFORE AFTER DAYS TO DIAGNOSIS FROM HOSPITAL ADMISSION FROM FIRST SUSPICION SUGGESTIVE CT-SCAN PRE-DIAGN 31 ± 9 7± 5 1/8 21 ± 5 2± 1 23 / 25
 §Cough")
CLINICAL SYMPTOMS IN 45 CASES OF IA IN HSCT PATIENTS §Fever 34/45 (75%) §Cough 12/45 (27%), §Dyspnoea 12/45 (27%) §Chest pain 9/45 (20%). §No sign or symptom 3 (positive GM with multiple pulmonary nodules on CT scan). § Radiological pulmonary lesions were mainly represented by nodules (8/42, 19%), cavitations (10/42, 24%) and wedge-shaped consolidations (4/42, 10%). §Notably, the halo sign was never found. Mikulska et al, BMT 2009

A comprehensive approach to the diagnosis of IFI Host Laboratory Diagnosis Imaging Clinical presentation

Aspergillosis: obtaining a diagnosis Sputum Bronchoalveolar lavage Galacto mannan, glucan, PCR Galactomannan, glucan, PCR CT scan Fine needle biopsy Surgical biopsy (adapted from Ben de Pauw, 2001)

Traditional methods • Positive blood culture • Candida, Fusarium, Cryptococcus and others; not Aspergillus, Mucor • Positive histology from site of infection • allows generic diagnosis of fungal infection • requires positive culture for etiological definition • Positive culture from site of infection • limitation due to contamination/colonization problems • may require positive histology for confirmation, depending on site

NON INVASIVE DIAGNOSTIC TESTS FOR FUNGAL INFECTIONS Species specific PCR Genus specific Fungi and bacteria galactomannan capsular antigen Panfungal-PCR (1 3)-ß-D-glucan C-Reactive Protein (CRP), procalcitonin (PCT), interleukin-6 (IL-6)
-ß-D-glucan (BDG) CHARACTERISTICS üIt’s a component of the fungal cell wall üThere are")
(1 3)-ß-D-glucan (BDG) CHARACTERISTICS üIt’s a component of the fungal cell wall üThere are 4 differnt commercial system üFDA approved 2004 as a support for the diagnosis of IFI üPANFUNGAL TEST Positive in Aspergillus Candida Pneumocystis carinii Fusarium Trichosporon Saccharomyces cerevisiae Acremonium Histoplasma capsulatum Doe’nt detect Cryptococcus Zygomicetes
-ß-D-glucan (BDG) LIMITS • Need of glucan-free tools; • Important risk of contamination")
(1 3)-ß-D-glucan (BDG) LIMITS • Need of glucan-free tools; • Important risk of contamination (glucan is ubiquitarious) FALSE POSITIVE q q q q Emodyalisis membranes Albumin (Usami 2002, Ohata 2003) (Miyazaki 1995, Yoshioka 1989) Immunoglobulins (Ogawa 2004) Gauzes (Kimura 1995) Hyperbilirubinemia, hypertriglyceridemia (Pickering 2004) Antibiotics (amoxicillin-clavulanate) (Mennink-Kersten 2006) Pseudomonas aeruginosa infections (Mennink-Kersten 2008)
-ß-D-glucan (BDG) Obayashi et al. CID 2008:")
(1 3)-ß-D-glucan (BDG) Obayashi et al. CID 2008:




Comparison of empirical and PCR-based preemptive antifungal therapy in 408 allogeneic stem cell transplant recipients • PCR screening twice weekly during stay in hospital and once weekly after discharge until D 100 • Antifungal therapy initiation – PCR group: in PCR+ patients with signs of infection and in patients with 2 consecutive PCR + – Empirical treatment group: 5 d of febrile neutropenia Antifungal therapy Proven invasive aspergilosis PCR based n = 196 Empiric n = 207 109 (56%) 11 76 (37%) 16 (p<0. 05) • Reduction in early mortality (D 30) in patients receiving PCR-based therapy but no difference in mortality at D 100 and D 180 (Hebart et al. ASH 2004)

Clinical Infectious Disease 2005; 41: 1242 -50

136 episodes 16% 117 febrile episodes 19 no fever + 82 defervesence 9 cases positive CT 10 positive GM antigen 19 cases for pre-emptive antifungals

19 no fever 35% 136 episodes 117 febrile episodes 82 defervesence 30 persistent fever 11 unexplained relapses 41 candidates empirical antifungals
 trial run in 12")
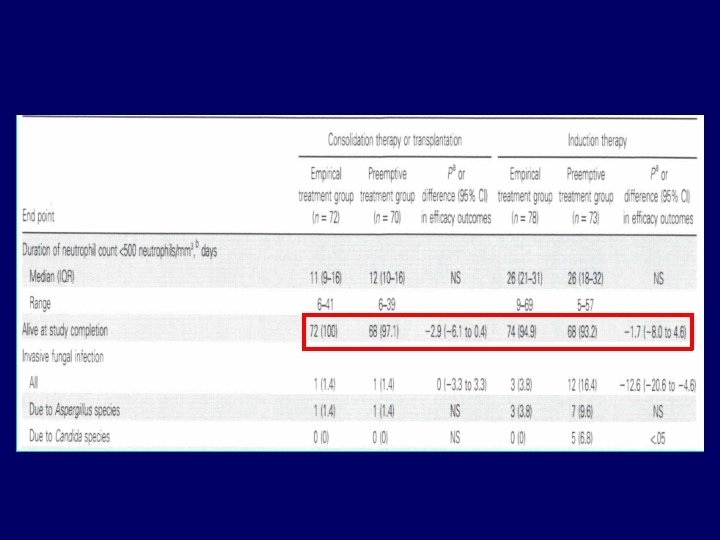
PREVERT Study Design • Prospective multicentric, unblinded, randomised (1: 1) trial run in 12 French centers between April 2003 February 2006 • Non-inferiority trial (< 8% difference in ITT and PP) • Randomisation stratified on center, induction vs consolidation, and antifungal prophylaxis • Proven and probable IFI: EORTC-MSG definitions • Primary endpoint: survival either 14 days after recovery from neutropenia or at 60 days if persistent neutropenia Cordonnier et al. ASH 2006

Empirical v. Preemptive antifungal therapy in high risk neutropenic patients PREVERT STUDY Overall survival p=ns Invasive fungal infections *p<0. 02

Current situation • Pre-emptive therapy logical, feasible, safe and probably costeffective • However, not all centers can perform lung CT scan and GM monitoring as often as required • For this reason, empirical therapy remains standard practice in some smaller centers • Big centers start approaching pre-emptive therapy • No drug has been tested in a comparative way for this indication • Drugs approved for empirical or targeted therapy are likely working (caspo, L-Am. B, vorico).

My opinion • Diagnosis of IFI is a complex intellectual exercise leading to different degrees of diagnostic certainty and requiring experience, prudence and the availability of relatively sophisticated and/or invasive diagnostic tools (culture, biopsy, CT, GM, glucan? ) • The lower the risk (host factors) the higher the evidence required • The strategy of how using the antigen-detection tests and/or PCR is still controversial and subject to personal interpretations • Pre-emptive therapy has been shown to be safe and effective
- Slides: 42