Calcium Metabolism and Parathyroid Disease James Mc Kinley

Calcium Metabolism and Parathyroid Disease James Mc. Kinley MD University of Texas Health Center at Tyler

Calcium Metabolism n Hypercalcemia – will be our primary focus n n n Causes Diagnosis Treatment Hypocalcemia – briefly Eucalcemia – won’t be discussed at all! Hyperparathyroidism n n n Causes Diagnosis treatment

Calcium Metabolism n n 99% of total body calcium resides in bone Remainder n n n 40% bound to serum proteins 13% complexed with anions 47% free ionized calcium – physiologically active form, regulated by vitamin D and PTH

Calcium Metabolism n n Decreased serum calcium stimulates PTH secretion within seconds PTH ½ life in serum is 4 minutes

Parathyroid Hormone n Renal effects n n Increase calcium reabsorption and increased phosphorus excretion from renal tubule Stimulates renal 1 -alpha-hydroxylase to activate vitamin D Bone effects – stimulates osteoclastic bone reabsorption Net effect – increase serum calcium, decrease serum phosphorus
 increases calcium and phosphorus absorption")
Vitamin D n Active form (1, 25–OH vitamin D) increases calcium and phosphorus absorption from GI tract

Calcium Metabolism n What can go wrong?

Hypercalcemia - Symptoms n n n Depend on Calcium level, rapidity of onset, state of hydration Most develop symptoms at a level > 12 mg/d. L, virtually all symptomatic > 14 Vague symptoms – fatigue, weakness, anorexia, nausea, polyuria, dehydration, lethargy, stupor, coma
 – most")
Hypercalcemia - Etiology n n n n Primary Hyperparathyroidism Cancer (metastatic, lymphoma) – most common in hospitalized patients Multiple Myeloma Hyperthyroidism Hypervitaminosis D (or A) Immobilization Sarcoidosis Addisonian crisis

Hypercalcemia n n n Idiopathic/spurious – venous stasis, postmenopausal women Thiazide diuretics – hold for 2 weeks Hypocalciuria – Familial Hypocalciuric Hypercalcemia Paget’s dz – hypercalcemia in conjunction with immobilization Milk-Alkali syndrome – excessive intake of Na. HCO 3 and milk (calcium salt) Aluminum toxicity - rare
 Treat")
Hypercalcemia - Treatment n n Treat if symptomatic (mental status changes, confusion, delusions) Treat if serum calcium > 15 n n NS bolus until volume restored, then 100 – 200 ml/hr and Lasix 40 – 80 mg (1 mg/kg) q 4 -6 hours Bisphonates (onset 24 -48 hrs) Calcitonin 4 – 8 IU q 6 -8 hrs (onset immediate, resistance develops in 24 -48 hrs) Empiric Mg and K
 Males > 60")
Hyperparathyroidism n n n Most common disorder of hypercalcemia (ambulatory patients) Males > 60 years : 100/100, 000 Females > 60 years : 300 -400/100, 000 All ages : 250/100, 000 Patients usually > 50 years of age Females > males 4 : 1

Hyperparathyroidism n 1 person in 1000 will need parathyroid surgery

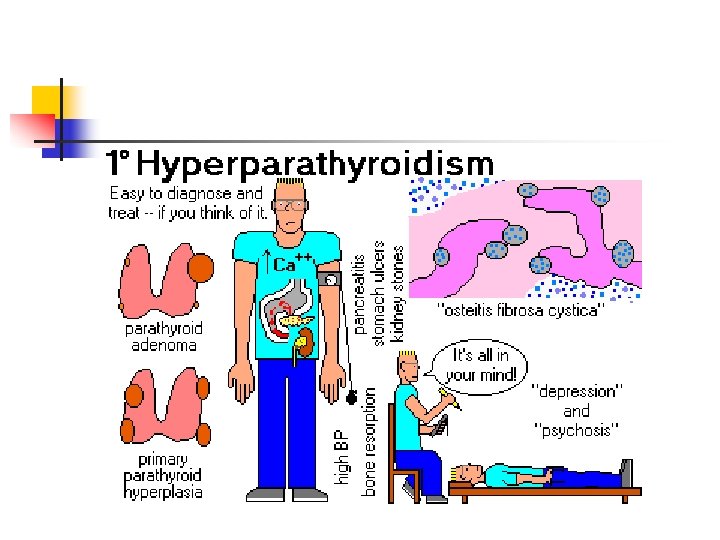
hyperparathyroidism

Hyperparathyroidism Symptoms n n Painful bones, renal stones, abdominal groans, and psychic moans Bone and joint pain, renal stones – late findings

Hyperparathyroidism – Signs/symptoms n Skeletal n n n Bone pain and tenderness Cystic bone lesions (brown tumors) Skeletal demineralization Spontaneous fracture (compression fx’s) Osteoporosis Osteitis fibrosa cystica

Hyperparathyroidism – signs/symptoms n Renal n n Nephrolithiasis Nephrocalcinosis Decreased GFR Polydipsia/polyuria

Hyperparathyroidism – signs/symptoms n GI n n n Abdominal distress Gastroduodenal ulcer Pancreatitis Constipation Pancreatic calcification Vomiting, anorexia, weight loss

Hyperparathyroidism – signs/symptoms n Mental/psychiatric n n n Fatigue Apathy Anxiety Depression Psychosis Coma/ diffuse EEG changes

Hyperparathyroidism – signs/symptoms n Neuromuscular n n Cardiovascular n n n Muscle weakness, hypotonia HTN Short QT interval Articular/periarticular n Arthralgias/gout/pseudogout/calcifications

Hyperparathyroidism – signs/symptoms n Ocular n n n Band keratopathy Conjunctivitis Conjunctival calcifications

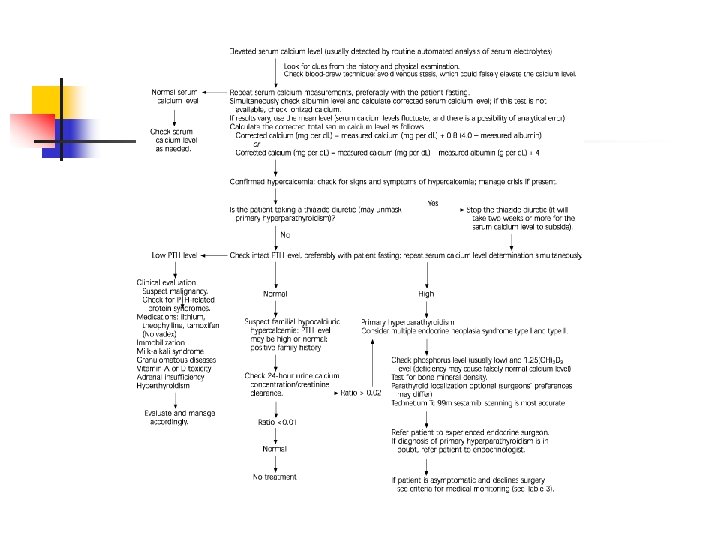
Hyperparathyroidism Diagnosis n Elevated serum calcium n n n Repeated measurements (can vary, minimal venous occlusion, fasting) Ionized calcium may be more accurate, but not widely available, must be sent on ice, etc. Corrected for serum albumin Elevated serum parathyroid hormone (intact) Usually found during workup for osteoporosis or elevated calcium in lab work

Hyperparathyroidism n Primary hyperparathyroidism n n Inappropriate secretion of PTH 85% single parathyroid adenoma 14 – 15% diffuse hypertrophy of PT gland < 0. 5 -1% parathyroid carcinoma (palpable)

Parathyroid Adenoma

Hyperparathyroidism n Secondary n n n Results from physiologic or pathophysiologic response to hypocalcemia Can result from vitamin D deficiency or decreased calcium intake(dietary or malabsorption) Most cases due to chronic renal failure – decreased production of activated vitamin D

Hyperparathyroidism n Tertiary n n n Due to prolonged hypocalcemia (usually due to chronic renal failure) This results in parathyroid gland hyperplasia May need parathyroidectomy

Hyperparathyroidism n Elevated calcium and PTH – Now what?

Hyperparathyroidism – localize the lesion n n Diagnostic studies – 80 -85% of PT glands in normal location 15 -20% ectopic – anywhere from hyoid bone superiorly to the aortopulmonary window inferiorly (anterior superior mediastinum most common)

Hyperparathyroidism Imaging n n n Ultrasound CT scan FNA MRI Angiography (with/without selective vein sampling) Sestamibi scan – with SPECT scanning, give 3 -D image, 91% sensitivity, 98. 8% specificity

Sestamibi scan

Surgery n n n With localization, minimally invasive endoscopic procedure, small incision, as fast as 15 minutes PTH should drop to normal/near normal after surgery, confirm proper treatment If not, explore both sides of neck 90 – 95% success rate 1% morbidity
 Post op hypocalcemia")
Surgery n n 20 – 30 % experience temporary hypoparathyroidism (hypocalcemia) Post op hypocalcemia nadir at 20 hrs (to 36), normalizes by the following day (post op day 2 -3) Undetectable PTH at 8 hours, normal by 30 hours Post op calcium replacement only if symptomatic or positive Trousseau’s or Chvostek’s sign

Hypocalcemia - Symptoms n n n Paresthesias, muscle stiffness and cramps, fasciculations, tetany Lower seizure threshold CHF, dysrhythmia, hypotension

Hypocalcemia - Treatment n n n Check ionized calcium if able 10 – 30 ml of 10% calcium gluconate solution IV over 10 minutes (150 ml D 5 W) Calcium infusion start at 0. 5 mg/kg/hr Telemetry Check serum calcium q 2 – 4 hours

Hyperparathyroidism – medical treatment n Criteria n n n Only mild serum calcium elevation No previous life threatening hypercalcemia Normal renal status (c. c. > 70%, no stones, nephrocalcinosis) Normal bone status (dexa > -2. 5) asymptomatic
 n n n")
Hyperparathyroidism – medical management n Monitoring (evidence level C, consensus opinion) n n n Biannual serum calcium (PTH? ) Annual serum creatinine Annual bone density testing

Hyperparathyroidism – Medical Management n Recommendations n n n Modest intake of calcium (1000 – 1200 mg per day) Vitamin D (400 – 600 IU per day) Up to 25% will develop surgical indications
")
Hyperparathyroidism n Surgical indications n n n n Symptoms (stones, nephrocalcinosis, osteitis fibrosa cystica) Serum calcium > 1 mg per d. L above normal Renal function reduced > 30% ( compared to age matched controls) Osteoporosis (T score < -2. 5) Patient age < 50 years Medical surveillance not desirable or possible Surgery requested by the patient

Secondary and Tertiary Hyperparathyroidism n n Goal is to normalize calcium values Supplement calcium and vitamin D ESRD patients need phosphate binders Tertiary hyperparathyroidism and severe metabolic bone disease, may need parathyroidectomy

Calcium metabolism n n n Kidney – PTH Bone – PTH GI – Vitamin D Hyper and hypocalcemia Hypercalcemia – hyperparathyroidism most common cause in ambulatory patients

Hyperparathyroidism n n Dx : Calcium and PTH levels Parathyroid adenoma most common cause of hyperparathyroidism Imaging/localizing techniques Tx : surgery vs medical management

References n n n n Taniegra ED, Hyperparathyroidism. Am Fam Physician 2004; 69: 333 -9, 340 Pou AM, Rosen FS, Parathyroid Disease: Diagnosis and Treatment. Grand Rounds, UTMB, Dept of Otolaryngology 3/27/2002 Bailey BJ, Calhoun KH, et al. Atlas of Head and Neck Surgery-Otolaryngology. Second Edition. Lippincott Williams and Wilkins. Philadelphia, PA. c. 2001: 236245. Dackiw AP, Sussman JJ, et al. Relative Contributions of Technetium Tc 99 m Sestamibi Scintigraphy, Intraoperative Gamma Probe Detection, and the Rapid Parathyroid Hormone Assay to the Surgical Management of Hyperparathyroidism. Archives of Surgery. 2000; 135: 550 -557. Marx SJ. Medical Progress: Hyperparathyroid and Hypoparathyroid Disorders. The New England Journal of Medicine. 2000; 343: 1863 -1875. Mitchell BK, Merrell RC, Kinder BK. Localization Studies in Patients with Hyperparathroidism. Surgical Clinics of North America. 1995; 75: 483 -498. Reber PM, Hunter, H. Hypocalcemic Emergencies. Medical Clinics of North America. 1995; 79: 93 -106. Handbook of Emergency Cardiovascular Care for Healthcare Providers. American Heart Association. 2004.

Picture References n n n Slide 12: www. aafp. org/afp/20040115/333. html Slide 16: www. endotext. org Slide 13: www. pathguy. com Slides 26: www. edcenter. med. cornell. edu Slide 33: www. parathyroid. com
- Slides: 45