CALCINEURIN INHIBITORS Specific Tcell inhibitors Cyclosporine It is
 Cyclosporine It is a cyclic polypeptide with 11 amino")
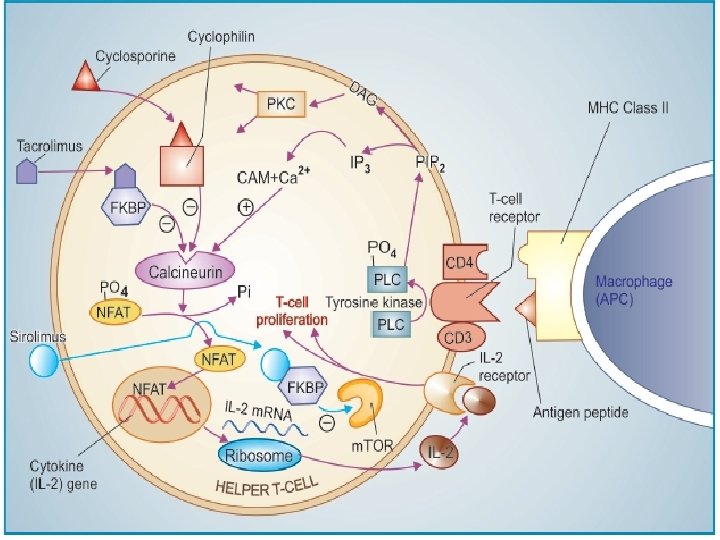
CALCINEURIN INHIBITORS (Specific T-cell inhibitors) Cyclosporine It is a cyclic polypeptide with 11 amino acids, obtained from a fungus and introduced in 1977 as a highly selective immunosuppressant which has markedly increased the success of organ transplantations. It profoundly and selectively inhibits T lymphocyte proliferation, IL-2 and other cytokine production as well as response of inducer T cells to IL-1, without any effect on suppressor T-cells. Lymphocytes are arrested in G 0 or G 1 phase. Cyclosporine is most active when administered before antigen exposure, but can, in addition, suppress the responses of primed helper T cells; hence useful in autoimmune diseases as well. Cyclosporine selectively suppresses cellmediated immunity (CMI), prevents graft rejection and yet leaves the recipient with enough immune activity to combat bacterial infection. Unlike cytotoxic immunosuppressants, it is free of toxic effects on bone marrow and RE (reticuloendothelial) system. Humoral immunity remains intact. However, it is nephrotoxic.

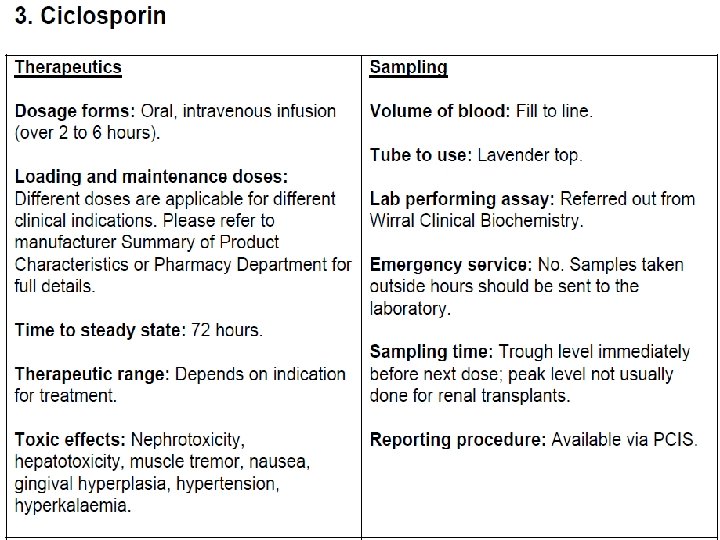
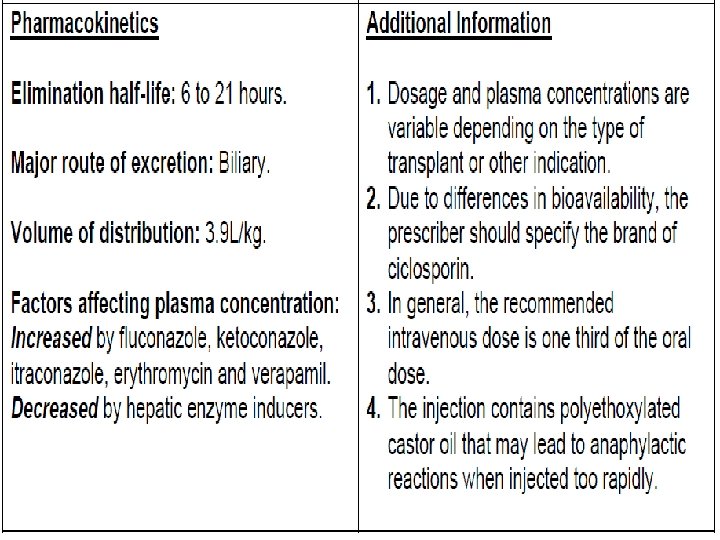
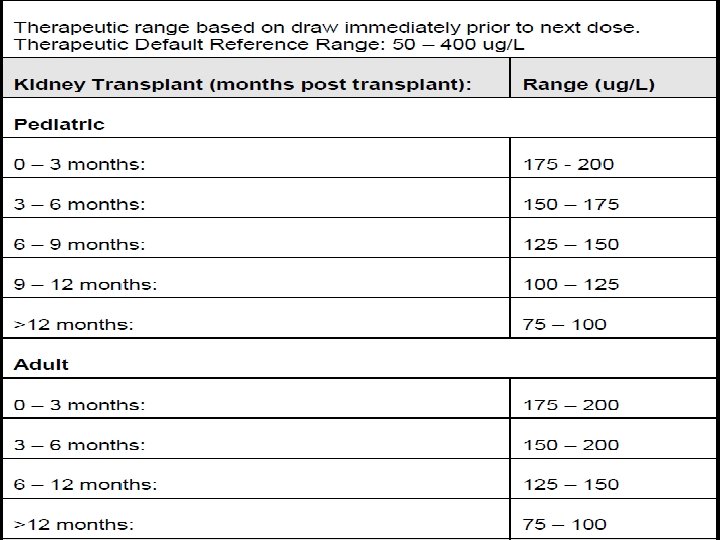
Cyclosporine is the most effective drug for prevention and treatment of graft rejection reaction. It is routinely used in renal, hepatic, cardiac, bone marrow and other transplantations. For induction it is started orally 12 hours before the transplant and continued for as long as needed. When graft rejection has started, it can be given i. v. , because oral bioavailability is low, dependent on presence of bile and is highly variable. Blood level monitoring is required for effective therapy. It is concentrated in WBCs and RBCs, metabolized in liver by CYP 3 A 4 and excreted in bile. The plasma t½ is biphasic 4– 6 hr and 12– 18 hr. Dose: 10– 15 mg/kg/day with milk or fruit juice till 1– 2 weeks after transplantation, gradually reduced to maintenance dose of 2– 6 mg/kg/day. Therapy may be started with 3– 5 mg/kg i. v. infusion.

Cyclosporine is a second line drug in autoimmune diseases, like severe rheumatoid arthritis, bronchial asthma, inflammatory bowel disease, dermatomyositis, etc. and in psoriasis, especially to suppress acute exacerbations. It is generally used along with corticosteroids or Mtx. Good results have been obtained in some cases of aplastic anaemia. Adverse effects are milder, rise in BP, precipitation of diabetes, anorexia, hyperkalaemia, hyperuricaemia, opportunistic infections, hirsutism, gum hyperplasia, tremor and seizures. Drug interactions Cyclosporine can interact with a large number of drugs. All nephrotoxic drugs like aminoglycosides, vancomycin, amphotericin B and NSAIDs enhance its toxicity toxic—the major limitation, and impairs liver function.

§By depressing renal function, it can reduce excretion of many drugs. §Phenytoin, phenobarbitone, rifampin and other enzyme inducers lower its blood levels so that transplant rejection may result. §On the other hand, CYP 3 A 4 inhibitors erythromycin, ketoconazole and related drugs inhibit its metabolism to increase bioavailability and cause toxicity. §Potassium supplements and K+ sparing diuretics can produce marked hyperkalaemia in patients on cyclosporine. Indication Idiopathic Thrombocytopenic Purpura (ITP) Interstitial Cystitis Juvenile Idiopathic Arthritis (JIA) Kidney Transplant Rejection Liver Transplant Rejection Nephritis, Lupus Psoriasis Severe Ulcerative Colitis Uveitis Refractory Ulcerative colitis Severe, active Rheumatoid arthritis Severe, recalcitrant Plaque psoriasis Suppressed tear production Bone Marrow Transplant Rejection. Glomerulonephritis minimal lesion. Glomerulosclerosis, Focal Segmental. Graft Versus Host Disease (GVHD) Heart Transplant Rejection

Absorption The absorption of cyclosporine from the gastrointestinal tract is incomplete and variable. Protein binding In the plasma, approximately 90% is bound to proteins, primarily lipoproteins. In blood, the distribution is concentration dependent. Approximately 33% to 47% is in plasma, 4% to 9% in lymphocytes, 5% to 12% in granulocytes, and 41% to 58% in erythrocytes. Metabolism Hepatic, extensively metabolized by the cytochrome P 450 3 A enzyme system in the liver. Route of elimination Elimination is primarily biliary with only 6% of the dose excreted in the urine.

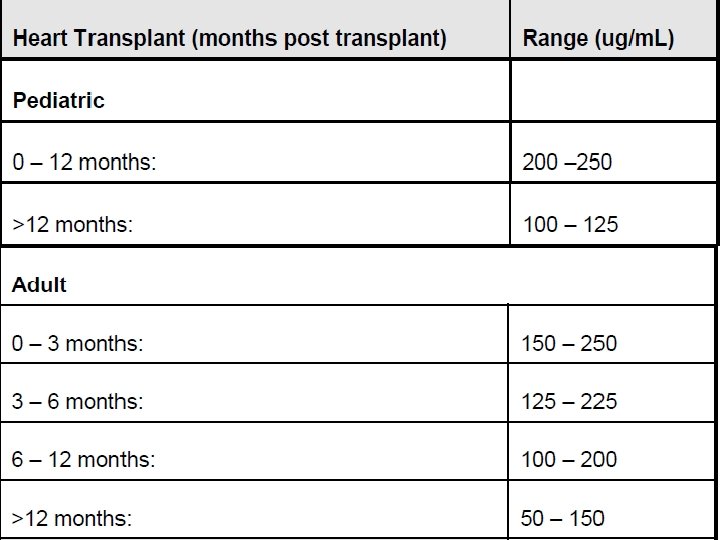
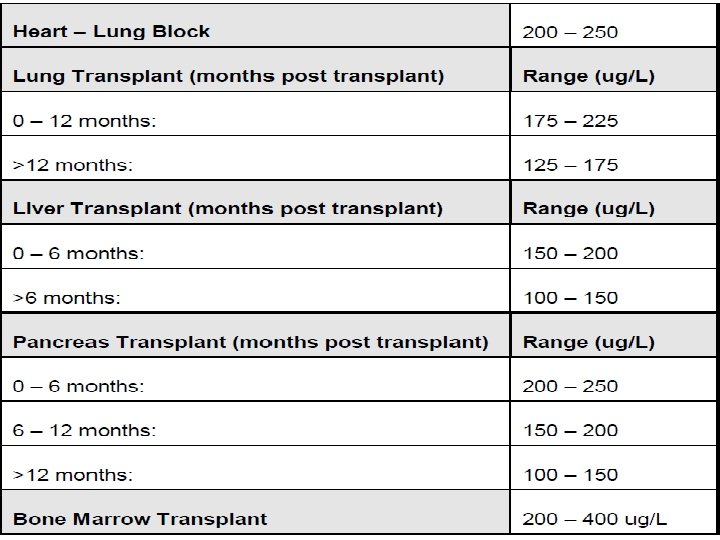
Food Interactions v. Avoid salt substitutes containing potassium. v. Avoid taking with grapefruit or grapefruit juice as grapefruit can significantly increase serum levels of this product. v. Red wine may reduce cyclosporine levels due to increased metabolism, therefore it appears prudent to avoid red wine (white wine does not appear to affect cyclosporine metabolism). v. When taken with a meal, AUC and Cmax of cyclosporine decreased. Therapeutic drug monitoring HPLC method EMIT (enzyme multiplied immunoassay technique)
- Slides: 12